w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Medication
adherence
in
patients
with
juvenile
idiopathic
arthritis
Liana
Silveira
Adriano
a,b,∗,
Marta
Maria
de
Franc¸a
Fonteles
a,
Maria
de
Fátima
Menezes
Azevedo
b,
Milena
Pontes
Portela
Beserra
a,
Nirla
Rodrigues
Romero
aaUniversidadeFederaldoCeará(UFC),Fortaleza,CE,Brazil bHospitalInfantilAlbertSabin(HIAS),Fortaleza,CE,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received27January2015
Accepted24November2015
Availableonline30May2016
Keywords:
Medicationadherence
Juvenileidiopathicarthritis
Pharmaceuticalcare
a
b
s
t
r
a
c
t
Objective:Theaimofthisstudywastoinvestigatepharmacologicaltreatmentadherenceof
patientswithjuvenileidiopathicarthritis,attendedinanoutpatientpharmacyatatertiary
hospitalinnortheasternBrazil.
Methods:Theanalysisofadherencewasperformedalongwithcaregivers,througha
struc-turedquestionnairebasedonMorisky,GreenandLevine,whichenabledthecategorization
ofadherencein“highest”,“moderate”or“low”grades,andthroughevaluatingmedication
dispensingregisters,whichclassifiedtheactofgettingmedicationsatthepharmacyas
“regular”or“irregular”.DrugRelatedProblems(DRP)wereidentifiedthroughthenarrative
ofcaregiversandclassifiedaccordingtotheSecondGranadaConsensus.Then,a
pharma-ceuticalorientationchartwithinformationaboutthetherapeuticregimenwasapplied,in
ordertofunctionasaguideforissuesthatinfluencedadherence.
Results:Atotalof43patientswasincluded,withameanageof11.12years,and65.1%(n=28)
werefemale.Applyingthequestionnaire,itwasfound“highest”adherencein46.5%(n=20)
patients,“moderate”adherencein48.8%(n=21),and“low”adherencein4.7%(n=2).Through
ananalysisofthemedicationdispensingregisters,alowerlevelofadherencewasobserved:
only25.6%(n=11)oftheparticipantsreceived“regularly”themedications.Twenty-sixDRP
wasidentified,and84.6%(n=22)wereclassifiedasreal.Therewerenosignificant
associa-tionsbetweensocio-demographicvariablesandadherence,althoughsomecaregivershave
reporteddifficultyinaccessingthemedicinesandinunderstandingthetreatment.
Conclusion: Ourfindingsshowedproblemsintheadherenceprocessrelatedtoinattention,
forgetfulnessandirregularityingettingmedicines,reinforcingtheneedforthedevelopment
ofstrategiestofacilitateabetterunderstandingoftreatmentandtoensureadherence.
©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND
license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](L.S.Adriano).
http://dx.doi.org/10.1016/j.rbre.2016.05.004
2255-5021/©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/
Adesão
ao
tratamento
farmacológico
em
pacientes
com
artrite
idiopática
juvenil
por
meio
de
questionários
Palavras-chave:
Adesãoaotratamento
farmacológico
Artritejuvenilidiopática
Atenc¸ãofarmacêutica
r
e
s
u
m
o
Objetivo: Investigar a adesão ao tratamento farmacológico de pacientes com artrite
idiopáticajuvenil,atendidosnafarmáciaambulatorialdehospitalterciáriodoNordeste
doBrasil.
Métodos: Aanálisedaadesãofoifeitajuntoaoscuidadores,pormeiodequestionário
estru-turadocombasenotestedeMorisky,GreeneLevine,queviabilizouacategorizac¸ãoda
adesãoem“máxima”,“moderada”ou“baixa”,edaavaliac¸ãodosregistrosdedispensac¸ão
dosmedicamentos,queclassificouaretiradademedicamentosnafarmáciacomo“regular”
ou“irregular”.Osproblemasrelacionadoscommedicamentos(PRM)foramidentificadospor
meiodanarrativadoscuidadoreseclassificadosconformeoSegundoConsensodeGranada.
Emseguida,aplicou-seumatabeladeorientac¸ãofarmacêutica,quecontéminformac¸ões
sobreoesquematerapêutico,deformaaesclarecerquestõesqueinfluenciavamaadesão.
Resultados: Participaram43pacientes,commédiade 11,12anos,65,1%,(n=28)dosexo
feminino. Por meio do questionário, verificou-se adesão “máxima” em 46,5% (n=20)
dos pacientes,“moderada”em 48,8%(n=21)e “baixa”em 4,7%(n=2). Peloregistrode
dispensac¸ão,observou-seumníveldeadesãomenor:apenas25,6%(n=11)dosparticipantes
receberamosmedicamentos“regularmente”.Identificaram-se26PRM,84,6%(n=22)
clas-sificadoscomo“reais”.Nãoforamobservadasassociac¸õessignificativasentreasvariáveis
sociodemográficaseaadesão,emboraalgunscuidadorestenhamrelatadodificuldadede
acessoaomedicamentoedecompreensãodotratamento.
Conclusão: Nossosachadosdemonstraramfalhasnoprocessodeadesão,relacionadasao
descuido,esquecimentoeàirregularidadeparareceberosmedicamentos,oquereforc¸aa
necessidadedeestratégiasparafacilitaracompreensãodotratamentoegarantiraadesão.
©2016ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC
BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Juvenileidiopathicarthritis(JIA)referstoaclinically
heteroge-neousgroupofpatientswitharthritisofunknowncause,with
morethansixweeksdurationthatstartsupto16yearsold.1
Thetreatmentofarthritisincludeseducationofthepatient
andhisfamily,drugtherapy,physiotherapy,psychosocial
sup-port,occupationaltherapyandsurgicalapproaches.Indrug
therapies, generallyanti-inflammatorynon-steroidal drugs,
corticosteroids, synthetic and biological disease-modifying
antirheumatic drugs, and immunosuppressants are used,2
inordertocontrolpainand toachieveclinicalinactivityor
remission.3
However,asthe completeresolutionofthe diseaseisof
uncommonoccurrence,mostchildrenandadolescentsneed
tousemultiplemedicationsforalongperiodoftime,
espe-ciallyinpolyarticularformsofarthritis.4 Thisaspect,along
withotherfactors,contributestoapooradherenceto
treat-ment of children and adolescents with chronic rheumatic
diseases.5
TheWorldHealthOrganizationconsidersthatinadequate
adherence totreatmentofchronic diseasesis aworldwide
problemofgreatmagnitudeand definesthat adherence to
treatmentcomprisesaphenomenonsubjecttotheinfluence
ofmultiplefactorsthatdirectlyaffectthepatientand
deter-minethebehaviorwithrespecttotherecommendationsfor
thetreatmentofdiseaseandthat,moreover,theyarerelated
tosocio-demographicconditions,thedisease,thetreatment,
therelationshipofhealthprofessionalswiththepatientand
alsotothepatienthim/herself.6
Crespo et al. suggested that physicians and
pharma-cists who follow the patient with arthritisshould perform
integrated actions in an effort to identify the emergence
of problems related to prescription drugs, including
non-adherence to treatment and, from this point, carry out
interventionstoreduceandpreventtheseproblems.7
Inthissense,thepresentstudyaimedtoanalyzethe
adher-encetopharmacologicaltreatmentofpatientswithJuvenile
Idiopathic Arthritisunder outpatientmonitoringina
pedi-atrichospitalinNortheasternBrazil,andidentifydrug-related
problemsthatcaninfluenceinthisprocess.
Patients
and
methods
The study was conducted inan outpatient pharmacy ofa
public hospitalin northeasternBrazil,considered as a
ref-erenceintertiarycareinpediatricarea,where,in2012,130
patientswithJIAwerefollowed.Inclusioncriteriawere:child
or adolescent (17 years and 11 months), witha confirmed
diagnosisofJIAthroughclinicalandlaboratorytests,
consid-ering: onset before age of 16, duration of symptoms less
than six weeks, with exclusion of the possibility of other
causes.1ThepatientshouldberegisteredintheSpecialized
caregivershouldattendtheoutpatientpharmacyofthe
hos-pitalduringthestudyperiodinordertoreceive medicines.
Weconsideredasprimarycaregiverthatpersonwho
admin-istersthemedicineand/ormonitorsthetreatmenttogether
withthepediatricpatient,toobtainasamplebyconvenience.
Exclusioncriteriawere:patientswithcaregiversshowingany
limitations that preventedanswering the questionnaire,or
whosecompanionswerenotthecaregiversresponsiblebythe
therapy.
The caregiver of each patient with JIA was asked to
answer the questionnaireon adherence, composed oftwo
blocks: the first block approached sociodemographic data,
wherevariablesrelatedtothepatient(genderandage)and
to the caregiver (education, origin, current working status
and family income), as well as the degree ofrelationship
between the caregiver and the patient were obtained; the
second block dealt withthe evaluation ofadherence, with
aninitialquestionthat identifiedifthe responsibleforthe
administration of the drug was the caregiver or the child
himself, followed by four questions related to the
adher-enceaccordingtoMorisky,GreenandLevinetest(adapted),8
with questions directed to the caregiver. Thus, each
posi-tiveresponsewasassignedavalueof1point.Afinalscore
ofzeroindicated‘high’adherence,1–2indicated‘moderate’
adherence, 3–4, ‘low’ adherence. An analysis of the
num-berofaffirmativeanswerstoeachquestionwasperformed,
in order to identifywhich parameter was more related to
non-adherence.
Afterthequestionnaire,thecaregiverwasaskedtorelate
howthemedicineswerebeingused.Thecaregiverwasfreeto
expresstheirperceptionsregardingthetreatmentinprivate
andinacomfortablemanner.Fromthereports,itwaspossible
toidentifyDrugRelatedProblems(DRP),whichwereclassified,
accordingtotheSecondConsensusofGranada,inproblemsof
need,effectivenessorsafety.9DRPratingwasstillconsidered
as‘real’,whentherewasamanifestation,or‘potential’,inthe
faceofthepossibilityofocurrence.10
Inthefaceofthemaindifficultiesofthecaregiverregarding
treatment,apharmaceuticalorientationtablewasdrawnup,
filledwithinformationonthetreatmentregimen(dose,
sched-ule, recommendations forintake with food, conservation),
basedonthemedicalprescription.Atthetimeofdispensing
thedrug,boththecaregiverandthepatientreceivedthetable
aswellastherelevantguidelines.
Adherence to treatment was evaluated by analyzing
the drug dispensing registers of the outpatient pharmacy
that provides the following medications for patients with
JIA: chloroquine, azathioprine, leflunomide, cyclosporine,
methotrexate, etanercept and adalimumab. During four
months,thebooksandannotationsoftheoutpatient
phar-macydispensingregister were evaluated monthly foreach
studyparticipant,inordertoverifytheoccurrenceofdelays
inobtainingthemedicinesbythecaregiver.Theanalysisof
thedrugdispensingregisterswasbasedonthemethodused
byGomesetal.,whichrankedtheobtainingofmedicinesin
thepharmacyas‘regular’or‘irregular’.11
Anadjustmentofthecriteriausedwascarriedout with
the purpose of its adaptation to the particular
medica-tions used for JIA, given that the dosage varies, namely,
chloroquine,azathioprine,leflunomideandcyclosporineare
daily agents; methotrexate and etanercept, weekly agents;
andadalimumab,everyotherweekagent.Intheoutpatient
pharmacyofthehospital,medicationsarereceivedin
suffi-cientquantityforonemonth.Thus,forpatientsusersofdaily
agents,itwasconsideredas‘irregular’thedelayofmorethan
oneday;forpatientsusersofweeklyagents,itwasconsidered
as‘irregular’thedelayofmorethaneightdays;andfinally,for
patientsusersofeverytwoweeksagents,itwasconsideredas
‘irregular’thedelayofmorethantwoweeks.
Finally, weestablishedastatisticalrelationshipbetween
thelevelofadherencetotreatmentandsocio-demographic
variables,usingtheStatisticPackageforSocialSciences(SPSS)
version16.0,andapplyingthechi-squaredtestwitha
signifi-cancecriterionforp<0.05.
TheprojectwasapprovedbytheHospitalResearchEthics
Committee, within the regulations governing research on
human beings under registration number 097/2011. The
informedconsentwassignedbycaregivers.
Results
Socio-demographicprofileofpatientsandcaregivers
Atotalof43patientsparticipatedinthestudy,ofwhom65.1%
(n=28)werefemale.Themeanageofthepatientswas11.12
years;23.2%(n=10)ofpatientswereagedunder8years,51.2%
(n=22)wereagedbetween8and14years,and25.6%(n=11)
between15and17years.
Regardingtheprofileofcaregivers,noneshowedlimitation
toansweringthequestionnaire.Themeanageofthe
partici-pantswas41.07years,and90.7%(n=39)werefemale.Among
thesecaregivers,76.8%(n=33)weremothersofpatients,9.3%
(n=4)werefathersand13.9%(n=6)hadanotherrelationship.
72.1%(n=31)livedinthecountryand,withrespecttoworking
status, 55.8%(n=24)were employed,butgenerallyhad low
income:44.2%(n=19)earnedlessthantheminimumwage,
51.2% (n=22) earnedonetotwominimumwages and4.6%
(n=2)earnedmorethanthreetimestheminimumwage.Only
32.6%(n=14)ofthecaregivershadeducationabove
elemen-taryschool.
Evaluationofadherencebyastructuredquestionnaire
Initially, in 81.4% (n=35) ofcases, the caregiver was
iden-tified as the main responsible for the process of taking
medicineathome.However,caregiversreportedthatpatients
usedtobeparticipatory,remindingthecaregiverthatitwas
timetotakethemedicine,whichshowstheco-participation
of children/adolescents in the process of completing the
treatment.
Byanalyzingthequestionnaire,adherencewasclassified
as‘high’in46.5%(n=20),‘moderate’in48.8%(n=21)and‘low’
in4.7%(n=2)ofcases.Wenotedthatthequestionwiththe
highestnumberofpositiveresponses(39.5%,n=17)wasonthe
‘neglectwithmedication administrationschedule,’followed
by the question of ‘forgetting toadminister the medicine’
Table1–Profileofaffirmativeresponsesofcaregivers (n=43)totheadaptedquestionnaireofMorisky,Green andLevine.
Parametersevaluated Yes
n(%)
1.Forgettingtoadministerthemedicine 11(25.6) 2.Carelessattimesabouttakingthemedicine 17(39.5) 3.Discontinuingthemedicinewhenfeelingbetter 2(4.7) 4.Discontinuingthemedicinewhenfeelingworse 4(9.3)
Analysisofadherenceusingthemedicationdispensing register
Intheanalysisofadherenceusingthemedicationdispensing register,itwasobservedthatduringthe four-monthperiod ofthe study,only25.6%(n=11)ofparticipantsreceivedthe agentsregularlyintheoutpatientpharmacy.27.9%(n=12)of participantshadan‘irregular’dispensation(adelayinoneof thestudymonths),30.2%(n=13)hadtwo‘irregular’ dispensa-tionsand16.3%(n=7)hadthree‘irregular’dispensations.
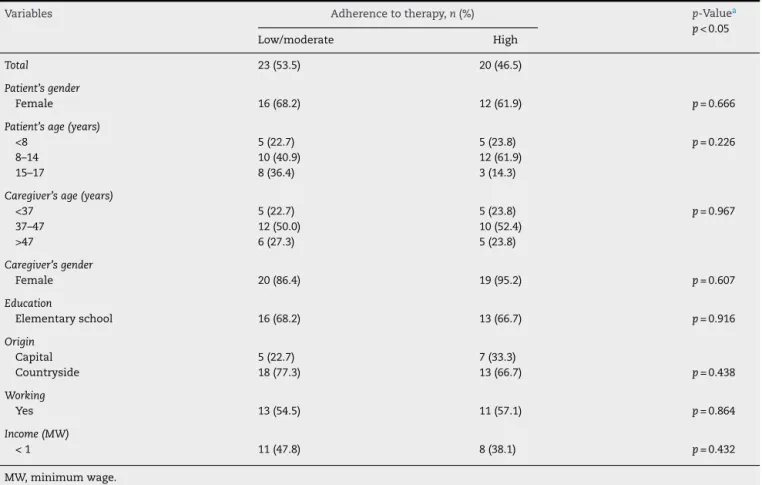
Relationshipbetweenlevelofadherenceand socio-demographicvariables
Therelationshipbetweenadherenceverifiedbythestructured questionnaire and socio-demographic variables ofpatients andcaregivers (Table2)wasevaluated. Concerning
statisti-calanalysis,patientswith‘low’or‘moderate’adherencewere
allocatedinthesamegroup.
The relationship of the variables with the adherence
assessedbyananalysisofmedicationsdispensingregisters
wasalsoestablished(Table3).Inthiscase,forstatistical
anal-ysis,patientswithatleastonedrugdispensationconsidered
as‘irregular’wereplacedinthesamegroup.
In both cases, no statistically significant relationship
between socio-demographic variables and adherence was
found,althoughcaregiversnotlivinginthestatecapitaland
withloweducation levelhavereportedgreater difficulty in
accessingandunderstandingofthetreatment,respectively.
AnalysisofDrugRelatedProblemsandimplementationof theinterventionmodel
Based on medication dispensing registers, the profile of
medicines’usefromSpecializedComponentof
Pharmaceu-tical Assistance for treatment of JIA was checked; it was
observedthat46.5%oftheparticipatingpatientsweretaking
only methotrexate; 18.6% methotrexate+etanercept; 13.9%
methotrexate+leflunomide;4.7%adalimumab;4.7%
azathio-prine; 4.7% azathioprine+chloroquine; 2.3% cyclosporine;
2.3%leflunomide;and2.3%methotrexate+adalimumab.
Inthe analysis ofDrug RelatedProblems, basedon the
reportsofcaregiversthemselvesaboutthetreatment,itwas
observedthat,ofthe43respondents,18didsomeaccountin
whichitwaspossibletoidentifyoneormoreDRP.Asawhole,
26DRPwereidentifiedandinmostcases(38.5%,n=10),the
problemwasrelatedtothelackofuseofanecessarydrug;
followed byanon-quantitativeuncertainty with respectto
thedrug(26.9%,n=7);quantitativeineffectivenessofthedrug
(19.2%,n=5);problemsarisingfromtheuseofan
unneces-sarydrug(11.5%,n=3)andnon-quantitativeineffectiveness
ofthedrug(3.9%,n=1).Ofthetotal26DRP,84.6%(n=22)were
classifiedas‘real’and15.4%(n=4)as‘potential’.
From the identification of DRP, it was possibletodirect
the implementation of the intervention model in order to
clarifythecaregiveronthemainissuesthatnegatively
influ-enced the treatment.The pharmaceuticalorientationtable
hasbeen usedasastrategytofacilitatethe understanding
of the treatment, minimizing forgetfulness and, therefore,
improvingadhesion.
Discussion
Theresultsfoundshowedthatmostpatientshad‘moderate’
or‘low’adherence,whichisrelatedtocompliancefailureinat
leastoneoftheaskeditems.Itwasnoticedthatthemain
ques-tionsassociatedwithnon-adherencewereacarelessnesswith
the medication administration schedule and forgetfulness,
which justifiesthe relevanceofinterventions, forexample,
thetablewiththetherapeuticregimenused,whichorganizes
theschedulesofmedicationtakenandpreventsforgetfulness,
giventhatclinicalimprovementwithJIAisrelatedtoan
appro-priatefulfillmentofanysuitabletreatment.12
Thesocio-demographicprofileoftheparticipatingpatients
was similar to that observed in other studies. We found
a predominance of female patients, which was expected,
consideringthatJIAaffectsaboutthreetimesmorewomen
thanmen.13
Thehighestfrequencyofpatientsaged8–14wasalsofound
both inother national (such asthe study by Santoset al.,
whoreviewedthemedicalrecordsofpatientswithJIAand
fol-lowedupattheRheumatologyDepartmentoftheHospitaldas
Clínicas,UniversidadeFederaldoEstadodeMinasGeraisfrom
2003to2005,whosepatientshadameanageof13.7years14)
andinternationalstudies,suchasthatbyFeldmanetal.,
con-ductedintwohospitalsinVancouver,with175childrenwith
JIA,wherethemeanagewas10.2years.15
Regardingtheprofileofcaregivers,itwasobservedthatthis
taskhasbeenperformedmainlybythepatient’smother–a
pointalreadyobservedinanotherstudyofpatientswithJIA.16
The identification of variables related to
socio-demographicprofileofcaregiverswasconsideredrelevantfor
theapplicationofthequestionnaireandalsofor
implemen-tingtheinterventionmodel,becausethisinformationallows
an initial inference of possible factors that can influence
adherence. Theinformationon education levelis relevant,
so thatonecan communicatethe explanationsadequately
foraclearunderstandingofthecaregiver.Theinformationof
thecaregiver’sorigin(mostofcaregiversinthisstudydidnot
liveinthestatecapital)allowstheidentificationofapossible
difficultyofaccesstomedicinesthatweredispensedbythe
publichealthsystemonlyinthestatecapital.Thelowincome
of many caregivers may hinder the displacement of such
peoplefromthemunicipalitieswheretheylivetothecapital,
as well asthe accessto the medication throughpurchase,
if necessary.Theworkingstatus(itwasreportedthatmost
caregiverswereemployed)mayberelatedtothedifficultyto
Table2–Associationbetweenadherencetotherapyassessedbythestructuredquestionnaireandsocio-demographic variablesofpatientsandcaregivers(n=43).
Variables Adherencetotherapy,n(%) p-Valuea
p<0.05
Low/moderate High
Total 23(53.5) 20(46.5)
Patient’sgender
Female 16(68.2) 12(61.9) p=0.666
Patient’sage(years)
<8 5(22.7) 5(23.8) p=0.226
8–14 10(40.9) 12(61.9)
15–17 8(36.4) 3(14.3)
Caregiver’sage(years)
<37 5(22.7) 5(23.8) p=0.967
37–47 12(50.0) 10(52.4)
>47 6(27.3) 5(23.8)
Caregiver’sgender
Female 20(86.4) 19(95.2) p=0.607
Education
Elementaryschool 16(68.2) 13(66.7) p=0.916
Origin
Capital 5(22.7) 7(33.3)
Countryside 18(77.3) 13(66.7) p=0.438
Working
Yes 13(54.5) 11(57.1) p=0.864
Income(MW)
<1 11(47.8) 8(38.1) p=0.432
MW,minimumwage.
a Significantifp<0.05,chi-squaredtest.
didnot find astatistically significant relationship between
thesevariablesandadherence,possiblybecausetheprofileof
thepopulationservedbythehospitalisveryhomogeneous,
notallowingtheobservationofdifferencesbetweenmoreor
lessadherentgroups.
Consideringthemeanageofpatientsparticipatinginthe
study,one cansee that evenin adolescence,the caregiver
participateswiththe patientinthe drug-takingprocess,as
recommendedintheliterature,whichhighlightsthe
impor-tanceofchildrentoparticipatewiththeirfamiliesinmaking
decisionsabouttheirowntreatment,inamannerappropriate
totheirstageofdevelopmentandtothenatureofthehealth
problemathand.17
Regardingtheassessmentofthedrugdispensingregister,
thismethodisconsideredassuitablefordetectingpatients
atriskofnoteffectively takingthe medication correctlyor
evenofabandoningtreatment.18Inthepresentstudy,through
theanalysisofdrugdispensingregisters,itwaspossibleto
showalowerlevelofadhesionthanthatobservedwiththe
analysisofthequestionnaires.However,wecannotstatein
allcasesthattheirregularityinobtainingthemedicationin
theoutpatientpharmacyisassociatedwithnon-adherence,
becauseinsomesituationsthecaregiver,livingmainlyinthe
interior,chosetobuythemedicines (iftheywere available
forsale directlytotheconsumer,suchascyclosporineand
azathioprine)oruseddrugleftoversfromachangeindosing
regimen.
Asfortherelationshipbetweensocio-demographic
vari-ablesandadherence,andinasimilarwaywithourfindings,
the study by Feldmanet al. foundno association between
socioeconomicstatusandadherencetotreatmentinpatients
withJIA.Thissame studyfoundhighertherapeutic
compli-ancereportedbycaregivers,whoconsideredthehighbenefit
ofdrugtreatmentinpatientswithJIA,thatis,whounderstood
theusefulnessoftreatment,aswellasamongpatientswith
lessseveredisease,observedbycountingfunctionaljoints.12
However,theseparameterswerenotassessedinourstudy.
TheresultsrelatedtoDRPrevealamorefrequent
occur-renceofnecessityproblemswherethepatientdoesnotusea
drugthathe/sheneeds,followedbysecurityproblems,where
thepatientshowsanon-quantitativeuncertaintywiththeuse
ofthe medication,which may be,for instance,an adverse
reaction. Therisk ofadverse events isacommon problem
in patients with chronic rheumatic conditions with direct
influence onadherence,together with the highnumber of
medicationsandthedurationandcomplexityoftreatment.18
ThestudyofSilvaetal.reportsthattheimplementationof
pharmaceuticalinterventions,fromtheidentificationofthe
DRP(seekingtoprovideclearandorganizedinformationin
relation tothe therapeutic regimen) isan effective wayto
optimize treatment. The pharmaceutical carein pediatrics
haspromotedthestreamliningofregulationsandthe
reduc-tionofmedicationerrorsandofadverseevents,aswellasan
Table3–Associationbetweenadherencetotherapyassessedwiththemedicationdispensingregisterand socio-demographicvariablesofpatientsandcaregivers(n=43).
Variables Dispensingregister(%) p-Valuea
p<0.05
Irregular Regular
Total 32(74.4) 11(25.6)
Patient’sgender
Female 20(62.5) 8(72.7) p=0.719
Patient’sage(years)
<8 9(28.1) 1(9.1) p=0.230
8–14 14(43.8) 8(72.7)
15–17 9(28.1) 2(18.2)
Caregiver’sage(years)
<37 9(28.1) 1(9.1) p=0.560
37–47 18(56.3) 4(36.4)
>47 5(15.6) 6(54.5)
Caregiver’sgender
Female 30(93.7) 9(81.8) p=0.267
Education
ElementarySchool 20(62.5) 9(81.8) p=0.291
Origin
Capital 10(31.3) 2(18.2) p=0.698
Countryside 22(68.7) 9(81.8)
Working
Yes 16(50.0) 8(72.7) p=0.294
Income(MW)
<1 15(46.9) 4(36.4) p=0.728
MW,minimumwage.
a Significantifp<0.05,chi-squaredtest.
Our study has some methodological limitations, also
perceivedinotherstudiesassessingtheadherenceinpediatric
patientswithJIA,astheworkofFeldmanetal.Theseauthors
arguethattheapplicationofquestionnairesmay bebiased
totheextentthatcaregiverscanreportthatthattothemis
sociallycorrect,overestimatingpatientcompliance.12
Evalua-tionofthedrugdispensingregister,whileprovidingrelevant
information,hasitslimitations,giventhatsomemedications
couldbeboughtinprivatepharmacies;andbearinginmind
thatthissituationwasnotalwaysreportedbycaregivers,we
cannotstatehowoftenthisactuallyhappened;inaddition,
thefactthatthe drugisreceivedbythecaregiverdoes not
makeit possibletostatethatthe patientwillactuallytake
it.Directmethodsofassessmentofadherencemethods,such
asthedeterminationofserumlevelsofdrugs, wouldallow
ustoobtainmoreaccurateresults.Inthisstudyit wasnot
possibletoassesstheimpactoftheinterventionmodel.Itis
suggestedthatfurtherstudies toevaluatethe treatmentin
patientswithJIAtakeintoaccounttherealizationofa
pharma-cotherapeuticfollow-upprogram,whichwillidentifydifferent
variablesthatwerenotaddressedinthisstudy,butwhichare
ofgreatimportancefortheadherencetothepharmacological
treatment.
Ourfindingsallowustoidentifyandunderstanddifferent
aspectsrelatedtothecurrentscenarioofadherenceto
phar-macologicaltreatment forJIAinthe studypopulation, and
flawswereobservedintheadherenceprocess,mainlyrelated
tonegligencewiththemedicationadministrationschedule,
forgetfulness andirregularityinreceiving thedrugs, which
reinforcestheneedforstrategiesthatfacilitateunderstanding
aboutthetreatmentandensureadherence.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.PettyRE,SouthwoodTR,MannersP,BaumJ,GlassDN, GoldenbergJ,etal.InternationalLeagueofAssociationsfor Rheumatologyclassificationofjuvenileidiopathicarthritis: secondrevision,Edmonton,2001.JRheumatol.2004;31:390–2.
2.MotaLMH,CruzBA,BrenolCV,PereiraIA,Rezende-FronzaLS, BertoloMB,etal.SociedadeBrasileiradeReumatologia. Diretrizesparaotratamentodaartritereumatoide.RevBras Reumatol.2013;53:158–83.
3.PrinceFH,OttenMH,vanSuijlekom-SmitLW.Diagnosisand managementofjuvenileidiopathicarthritis.BMJ.
2010;341:c6434.
4.MachadoC,RupertoN.Consensoemreumatologia
5. BugniVM,OzakiLS,OkamotoKYK,BarbosaCMPL,Hilário MOE,LenCA,etal.Factorsassociatedwithadherenceto treatmentinchildrenandadolescentswithchronic rheumaticdiseases.JPediatr.2012;88:483–8.
6. WorldHealthOrganization–WHO.Adherencetolong-term therapies:evidenceforaction.Geneve:WHO;2003.
7. CrespoR,TorresRA,BlascoJB,RuizAN.Atención
farmacéuticaapacientesconartritisreumatoideypsoriásica entratamientoconetanercept.FarmHosp.2005;29:171–6.
8. CivitaM,DobkinPL,FeldmanDE,KarpI,DuffyCM.
Developmentandpreliminaryreproducibilityandvalidityof theParentAdherenceReportQuestionnaire:ameasureof adherenceinJuvenileIdiopathicArthritis.JClinPsycholMed Settings.2005;12:1–12.
9. SantosH,IglésiasP,Fernández-LlimósF,FausMJ,Rodrigues LM.SegundoConsensodeGranadasobreProblemas RelacionadoscomMedicamentos:traduc¸ãointerculturalde espanholparaportuguês(europeu).ActaMedPort. 2004;17:59–66.
10.IvamaAM,NoblatL,CastroMS,JaramilloNM,OliveiraNVBV, RechN.Atenc¸ãofarmacêuticanoBrasil:trilhandocaminhos: relatório2001–2002.Brasília:Opas;2002.
11.GomesRRFM,MachadoCJ,AcurcioFA,GuimarãesMDC. Utilizac¸ãodosregistrosdedispensac¸ãodafarmáciacomo indicadordanão-adesãoàterapiaanti-retroviralem indivíduosinfectadospeloHIV.CadSaúdePública. 2009;25:495–506.
12.FeldmanDE,CivitaM,DobkinPL,MallesonPN,Meshefedjian G,DuffyCM.Perceivedadherencetoprescribedtreatmentin JuvenileIdiopathicArthritisoveraone-yearperiod.Arthritis CareRes.2007;57:226–33.
13.BellEA.Pharmacotherapyofjuvenileidiopathicarthritis.JPP. 2009;22:16–28.
14.SantosFPST,CarvalhoMAP,PintoJA,RochaACH,Campos WR.Artriteidiopáticajuvenilemumservic¸ode
reumatologia:BeloHorizonte,MinasGerais.RevMedMinas Gerais.2010;20:48–53.
15.FeldmanDE,CivitaM,DobkinPL,MallesonPN,Meshefedjian G,DuffyCM.Effectsofadherencetotreatmentonshort-term outcomesinchildrenwithJuvenileIdiopathicArthritis. ArthritisCareRes.2007;57:905–12.
16.AprilKT,FeldmanDE,PlattRW,DuffyCNM.Comparison betweenchildrenwithJuvenileIdiopathicArthritisandtheir parentsconcerningperceivedtreatmentadherence.Arthritis CareRes.2008;55:558–63.
17.SilvaLIMM,ChavesBMM,VasconcelosASOB,PoncianoAMS, ReisHPLC,FontelesMMF.Ocuidadofarmacêuticoem pediatria.RevSaúdeCrianc¸aAdolesc.2011;3:66–9.
18.BoteroLU,RojasLG,Mu ˜nozPA.Guíadeactuación farmacéuticaenpacientesconartritisreumatoide.1aed.