57
THE EFFECT OF THE TREATMENT AND THE COLLATERAL FACTORS DURING THE EPILEPSY
Marioara Nicoleta FILIMON1, Smaranda Rodica GOŢIA2, Laura GOŢIA2, Ion George DAN1
1
West University of Timisoara, Faculty of Chemistry Biology Geography, Department of Biology, Pestalozzi, 16, 300115, Romania 2
University of Medicine and Pharmacy “Victor Babes” Timisoara, Departament of Phisiology, E. Murgu, 2, 300041, Timisoara, Romania
ABSTRACT
The epilepsy is a chronic, paroxysmal clinical syndrome, with sudden beginning and ending. In major crises, it is characterized by fainting, tonic and clonic convulsions. When the epileptic crises are repeated, then we can talk about the epilepsy as a disease. It is not a form of intellectual retardation or a physical disease and it is not contagious. If the epilepsy shows up during childhood, it can disappear during adolescence or at the beginning of the adult life. The reasons are not clearly known, lots of people have a primary unidentified cause. Sometimes the epilepsy is the result of: brain traumatism, brain tumor, brain infections or brain vascular accidents. It is difficult to find a diagnosis for the epilepsy. It is made by the neurologist, using electroencephalography. This study present the dynamic evolution of a meal patient that was diagnosted whith epilepsy at the age of 7 mounth until the aget of 21.
KEY WORDS: epilepsy, epileptic crises, electroencephalography
INTRODUCTION
Epilepsy, a disease with a great clinical variability, has a genetic determinism, but it is also influenced by exogene factors, which can act even from the first period of birth and then during the whole life of the individual. The diagnosis is established based on the medical, on the description of the crisis (especially by people who are closer). History of the pacient by the clinical exam, by the electroencephalograph route in crisis and intercrisis.
Sometimes, it can be established by a computerized tomography or by the nuclear magnetic resonance, for secondary causes. The convulsions can show up at every age. Studies made in developed countries showed that 2 4 % from the citizens have recurrent crises in a certain moment during their lifetime. In the countries from the third world and in the urban areas, the incident is doubled. The epileptic crisis can last from a few seconds until several minutes and their presence is like the anatomical fix point of origin.
58
spasm, salivation, mastication, waves of heat, cold, pain, orgasm), sensorial and auditory (noises, voices, sounds), sensorial and visual (bright spots, stars, kaleidoscopic images, flames, explosions, imaginary people or animals, grotesque visions), sensorial, olfactive and gustative (unpleasant impressions) or a phenomenon called “already seen” or “never seen”; physical (delirious, obsessive phenomenon), for instance “that they hear their own thoughts.”
The major paroxysmal (slowly or quickly) is automatically followed by faint and convulsions. The convulsive phase lasts almost 60 seconds, meanwhile the patient is not breathing. Then comes the phase with the profound, loud breath, with hipersalivation, which can last a few seconds. Later, the patient wakes up, after a period of physiological sleep. When he wakes up, the patient doesn’t remember anything or is confused. After the crisis, the patient can suffer of: a cephalic crisis, drowsiness or the previous neurological disturbance can persist, especially those from the aura, lasting from minutes to days.
The differential diagnosis of the complex partial convulsions includes especially absences like petit mall and psychotic estates. The petit mall absences start and end suddenly, lasts only a few seconds, usually it is not followed by anxiety, it doesn’t establish an aura or automatisms with a diagnosis value. The complex partial crisis does not constitute an explanation for the violence or the deliberate crimes.
Like it was mentioned above, lots of partial crisis can develop rapidly into convulsions, before stopping the epileptic unload. Sometimes, the convulsions appear before any kind of focal signs. In these cases, the studied systematic electroencephalogram, the brain imagery or the limited paresis, may indicate the epileptic fixed point and the injury which was caused. The primary generalized epilepsies may have different forms, depending on the patient’s age in the beginning, nature and extension of the structured brain lesion or the associated metabolic.
Through convention, the primary generalized epilepsies can be divided concerning the presence or the absence of the convulsions (Borundel, 2006). Factors which may precipitate or accelerate the frequent epileptic crisis are multiple. Some of these factors are: dismetabolic factors (progressive brain anoxia, hypoglycemia, disturbance of the hydroelectrolytic metabolism, endocrine affections, gastrointestinal affections, cardiac insufficiency, and renal insufficiency), toxic factors (the use of alcohol), effort, physical trauma (Ion and co. 1999).
At children, we have the following forms of crisis:
59
simple absence, which lasts only 1 or 2 seconds and is characterized by the loss of consciousness. Usually, the patient is blinking rapidly, with a 3 4 Hz. The head of the child falls, the eyelids and sometimes the arms are rhythmically contracting, enuresis and short motor automatism can occur. At children severely affected, these episodes appear ten or even a hundred times. complex absence, longer ones, can last from 15 to 30 minutes, rarely more than a minute.
The crisis is characterized by a sudden, short, unconscious contraction of the entire body or in a certain part of the body. The phenomenon takes place, as it is normal, during the somnolence, before falling asleep. Slight, repetitive, unconscious contractions affect more girls than boys, and it can occur more in the arms then in the legs. This kind of epilepsy usually affects teenagers. A pain can be felt in the shoulders and arms. Frequently, the route of the EEG has a bifrontal, iritative activity with a 3,5 4 Hz. The slow activity is similar to the petit mall. Pathologically and genetically, it is closer to the petit mall and it has a reduced risk of tonic and clonic convulsions for the future (Andreoli and co. 1999).
The improvement of the studied subject is based on several collateral factors, like: the willingness of the patient to talk freely about his disease, strictly and efficiently respecting the treatment, respecting a balanced lifestyle (without alcohol, smoking, disco powerful noises, discontinuous lights), support from the family, permanent and unconditional support from colleagues and friends, the entourage, the created environment has a positive influence on the patients life quality.
Tests of sensorimotor function were given to 60 ambulatory epileptic patients, half with grand ma1 and half with temporal lobe seizures, none with neurological abnormalities; and to 50 control persons, 30 of them healthy and 20 with medical illness. The tests involved tapping, pointing, flow of speech, attention span, perception of "ambiguous figures" and adjustment to reversed glasses. The patients were significantly different from normal control persons and from patients with medical illness. The patients with grand ma1 and with temporal lobe epilepsy were also clearly different from each other, in that temporal lobe epileptics had more deficit in motor control, in flow of speech, attention span, and adjustment to reversed glasses, whereas patients with grand ma1 epilepsy were relatively intact. Since the deficits were related to the age at onset and duration of the disease, the disease may have been causative. A questionnaire listing 55 attributes to be graded on a 5 point scale was filled out by 300 respondents to obtain their opinion of patients with seizures. Unfavourable characteristics were attributed to epileptics more often than favourable ones. The same questionnaire was filled out by 53 ambulatory patients, who were much more apt to ascribe favourable attributes to themselves than were the respondents (Remschmidt, 1973).
60
perspective of adolescents and consider issues in the context of a developmental perspective. A focus group technique was used. Twenty two adolescents aged between 12 years 4 months and 18 years 0 months (6 males and 16 females) were stratified by age (12–13, 14–15 and 16+ years) into six focus groups. Data were transcribed and QSR NUD*IST 4.0 was used to help generate central themes. Several procedures were undertaken to increase validity and reliability of findings. Analysis identified two main themes comprising (a) issues related to adolescent development (identity formation) and (b) epilepsy related variables, with five and four main sub themes, respectively (‘peer acceptance’, ‘development of autonomy’, ‘school related issues’, ‘epilepsy as part of me’ and ‘future’, and ‘medication issues’, ‘seizures’, ‘knowledge of epilepsy’ and ‘sense of uncertainty’). The main issues related to peer acceptance and development of autonomy. In contrast to previous studies, academic difficulties were not highlighted as an issue. No significant age related differences in issues were identified. A conceptual model representing these findings is presented and clinical implications and suggestions for future research are reported.
The formation of a coherent sense of identity, separate from parents, is recognised as one of the core developmental tasks of adolescence. Adolescence is a time of significant transition in terms of biological changes, alteration in one’s role and development of appropriate and healthy peer relationships. Successful completion of these tasks is vital for healthy identity formation (i.e. the process by which an individual develops a comfortable and coherent idea of who they are, which relies heavily on positive evaluation by both themselves and other people). Difficulties with identity formation directly impact on the adolescent’s quality of life (QOL), i.e. “the individual’s evaluation of the quality of their lives as it relates to their own personal expectations”. Problems can result in depersonalisation and subsequently lead to low self esteem, depression, loneliness, anxiety and behavioural. Studies have consistently shown that epilepsy impacts on both peer relationships and the development of independence and autonomy in children and adolescents. Risk factors for poor QOL in teenagers have been identified as aged between 14 and 17 years, ‘active’ epilepsy and greater seizure severity14, higher numbers of medications, longer duration of illness and co morbid learning difficulties. Some studies have suggested that young people who are seizure free do not demonstrate poorer QOL than age matched controls. However, comparison of QOL in adolescents with epilepsy, diabetes and asthma, have found poorer QOL in those (Mcewan and co., 2004).
61
autonomic symptoms, and by an EEG [electroencephalogram] that shows shifting and/or multiple foci, often with occipital predominance.” The purpose of this review is to provide guidance for appropriate diagnosis and management of Panayiotopoulos syndrome.
Autonomic epileptic seizures and autonomic status epilepticus are the cardinal manifestations of Panayiotopoulos syndrome. Autonomic seizures in Panayiotopoulos syndrome consist of episodes of disturbed autonomic function with emesis as the predominant symptom. Other autonomic manifestations include pallor (or, less often, flushing or cyanosis), mydriasis (or, less often, miosis), cardiorespiratory and thermoregulatory alterations, incontinence of urine and/or feces, hypersalivation, and modifications of intestinal motility. In approximately one fifth of the seizures the child becomes unresponsive and flaccid (ictal syncope) before or often without convulsions. Cardiorespiratory arrest is exceptional. Moreconventional seizure symptoms often appear after the onset of autonomic manifestations. The child, who was initially fully conscious, becomes confused and unresponsive. Eyes turn to one side or gaze widely open. Only half of the seizures end with brief hemiconvulsions or generalized convulsions. Convulsive status epilepticus is extremely rare. Autonomic symptoms may be the only features of the seizures. Half of the seizures in Panayiotopoulos syndrome last for 30 minutes, thus constituting autonomic status epilepticus, which is the more common nonconvulsive status epilepticus in normal children. Two thirds of seizures occur during sleep (Covanis, 2006).
62
phenotypes of benign childhood focal seizures are likely to be linked together by a genetically determined, functional derangement of the systemic brain maturation that is age related (benign childhood seizure susceptibility syndrome). This is usually mild but exceptionally it may diverge to serious epileptic disorders such as epileptic encephalopathy with continuous spike and wave during sleep. Links with other benign and age related seizures in early life such as febrile seizures, benign focal neonatal and infantile seizures is possible.Overlap with idiopathic generalized epilepsies is limited and of uncertain genetic significance.Taking all these into account, benign childhood focal seizures and related epileptic syndromes would need proper multi disciplinary re assessment in an evidencebasedmanner (Panayiotopoulos et al, 2008).
MATERIALS AND METHODS
In the present work, we took into consideration the development of the epilepsy in adolescence, by following the dynamic of the obtained electroencephalography, from the day the diagnosis was known, from the first step until the present day.
This study has in view the following aspects: to identify the beginning of the disease and the possible causes; to observe of the treatments efficiency, following in dynamic the EEG (at the age of 7 month) until the age of 6; to identify the causes which brought back the epilepsy crises at the age of 16; to observe of the treatments efficiency at the age of 16 until the present day; the establishment of the factors precursory to the crisis, specific to the studied subject; to identify the progress realized by the use of a balanced lifestyle, specific to somebody who suffers from epilepsy.
The electroencephalogram is a preclinical exploration, which has a bioelectrical brain activity. It is made with the help of an apparatus called electroencephalograph. The bioelectric activity is depicted through some electrodes, changed in a hydro saline solution, used on the scalp, at equal distances, which collects the unloaded bioelectric, formally established in certain parts of the world. The electrodes are connected to an apparatus which amplifies the graph elements. Subsequently, these graph elements are registered on paper. There two types of registration: unipolar and bipolar. The information is gathered longitudinally or transversally (depending on the link between the electrodes).
At an electroencephalogram, we study: the morphology of the wave (form and duration), amplitude (in volts), the wave’s frequency and their topography. According to the group of electroencephalograms with a slow rhythm on a certain derivation, the pathological process can be located, but nothing can be said on the nature and pathology of the process (Mihalas et al, 2000).
63
of registration, the patient and the EEG route are studied in parallel, in order to observe the correlations between the changes of the route, certain motor display and possible changes of the consciousness. Partial reactions are noted as well as the objective ones wince, miotonia, and sleep during the record. In case of comitial crisis, first aid must be given.
The EEG route must be recorded while at rest, in conditions of activation (“cortical, electric activity”). By the aid of certain stimulus, the cortical activation method has a single target: to give birth to the pathological, electric manifestations, absent during the spontaneous EEG route. Usual activations are made on every EEG route, no matter the clinical assignment, because it has a simple technique and the patient goes under no risk.
The EEG diagnosis recommended in the following clinical domains: neurology – epilepsy, meningo encephalitis, degenerative processes, neuro surgery brain trauma, neoplasic, expansive processes, benign tumors, vascular malformations; psychiatry physical disease, neurosis; intensive therapy depth of coma and the diagnosis of clinical death.
The epileptic equivalent is defined through the fact that the patient is in a so called crepuscular state, wandering around without a specific goal in mind, or he is making gestures that he is not really aware of. It’s the same with the epileptic illness, characterized by subentry crisis.
The differential diagnosis epilepsy must eliminate pretending, tetany and hysterical crisis. The last disturbance is released by emotions and physical conflicts. The crisis takes place in front of witnesses. Usually, the patient is choosing the place to fall. During the crisis, the patient has to lie in bed, with untied necktie, opened collar and seatbelt. Eventually, the patient has to be immobilized, in order to avoid the hits, provoked by the convulsions.
The factors precursory to the crisis are generally represented by the loss of balance, powerful headache, indecipherable talking, dim sight, hard breath, a smell, a sound, intermittent light and continuous music. The epilepsy crisis can last from a few seconds (rhythmical movement of a certain part of the body) to a few minutes. The so called grand mall crisis lasts at least 5 minutes. If it lasts more than 5 minutes, then we are talking about a medical urgency.
The lifestyle of an epileptic patient consists of 8 hour sleep, without drinking alcohol, any salt, sweets or excitants. Choosing this kind of profession is the most important decision, because the nature of this disease is above every profession on air, water, by car or by foot.
64
medical treatment is combined with a natural treatment based on tea, juice, hot bath or cold showers and massages (www.terapii_naturiste.com).
RESULTS AND DISCUSSIONS
The present work has in view to follow the general aspects of the nervous system affection, namely the epilepsy. We studied somebody who has been diagnosed with epilepsy and we followed the evolution of the disease from the beginning of the disease until the present day. The followed aspects are: to identify the beginning of the disease and the possible causes, to observe the efficiency of the treatment until the age of 7 month and until the age of 6 to identify the causes which brought back the disease, to follow the efficiency of the treatment recommended at the age of 16 until the present day, to establish the precursory factors of the crisis for this specific patient and to identified the progress of the patient through a balanced lifestyle.
History of the disease
It started on April 26, at the day of his baptism, when the patient had a very high temperature. The parents thought that the cause of the temperature was that the child caught a cold and he was brought to the Municipal Hospital from Orsova for a month. Although, the child was kept in the hospital and he received proper treatment, the epileptic crisis continued the child was sent to the District Hospital from Timisoara, there the medicine was changed to another, but the crisis was rather frequent. For 1 year the child when on using the same treatment, without any changes.
At the age of 1 year and 10 month, the child is brought to the Emilia Elsza nursing home from Bucharest, where he is diagnosed with grand – mall epilepsy. Fenobarbital was recommended to him, which was considered a very dangerous medicine in those times. Later, the patient was brought home, using the same medicine. During 2 years, he was brought to Bucharest, every 3 month, for the doctors to check his health condition. The fenobarbital significantly reduced the convulsive crisis and the child’s health was beginning to improve.
By the age of 4, the visits to Bucharest were reduced from one to three month, to six month. The doze of the medicine was also reduced. At the age of 6, he had his last check – up.
65
A new treatment is recommended to him, based on fenobarbital and keppra. His treatment consisted of 3 tablets of keppra and 1 tablet of fenobarbital per day, during 1 year. During the second year, he had 1 keppra and 1 fenobarbital every morning, every night and half tablet in the evening. Later, he got 2 keppra and 1 fenobarbital. Then, this was reduced to 1 Phenobarbital and half tablet of keppra in the morning and at night. During the treatment, in 4 years, the crisis disappeared completely. Nowadays, the patient still under this treatment, hoping that one day he will end this treatment forever, that the crisis will disappear.
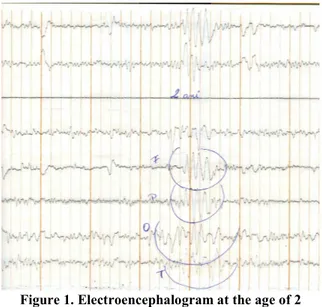
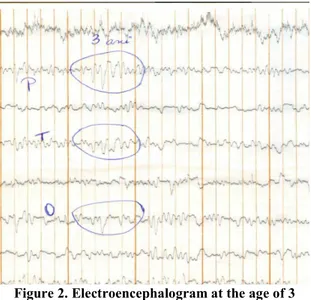
In the following, we will present some electroencephalograms and their explanation, in order to analyze, in dynamic, the way the disease has developed and the efficiency of the treatment. Trying to explain the electroencephalograms recorded at the age of 2 and 3, we discovered the following: paroxysm of biphasic sharp, sharp waves, sharp wave complexes in the temporal frontal regions, temporal parietal and temporal occipital; the activity of the θ and δ sinusoidal waves, grouped in buffets, temporary located with extensions through the frontal, parietal and occipital (fig. 1, 2).
Figure 1. Electroencephalogram at the age of 2
66
Figure 2. Electroencephalogram at the age of 3
During 2003 and 2008, the developing disease has been followed through electroencephalograms. The last electroencephalogram was made in 2004. Respecting the medical treatment was very important in this period. The electroencephalograms are characterized through: isoelectric routes with a normal aspect; predominance of the α rhythm in the posterior occipital temporal and parietal regions; the presence of the β rhythm in the former areas, without modifying them into bright stimulus (fig. 3). In the hyperpnoea, we established the growing amplitude of the α waves.
67
At the age of 16, the crisis was detached again, due to on unbalanced lifestyle (drinking alcohol, smoking, noises and intermittent light). There are more factors which determined the crisis like: emotional stress and the daily intellectual stress from school. By this time, the patient was in high school.
The studied patient who is stressed, becomes mad, looses his temper, he is aggressive, he starts to shiver, then he feels sick and finally he has the crisis. The factors precursory to the crisis were that the patient was loosing his balance, he had a powerful headache, his sight was dim, and he was breathing hard (a strong sigh), indescribable talk and finally the crisis itself.
Lotlley on improvement of the disease was observed. The factors which may have caused this improvement are: the patient’s ability to talk freely about his disease, respecting strictly and efficiently the treatment, having a balanced lifestyle (without alcohol, no smoking, disco powerful noises and intermittent lights), the family’s support, the permanent and unconditioned support from colleagues and friends. The environment, the created background had a positive influence on this patient’s lifestyle.
CONCLUSIONS
The electroencephalogram is a very useful method for diagnosing the epilepsy.
The dynamic follow of the EEG allows establishing an efficient treatment, the changes of the wave rhythm and the improvement of the route EEG.
The patient has to respect a balanced lifestyle (without alcohol, no smoking, disco powerful noises, intermittent light, adequate treatment, and affective support from the dear ones), which brings to the improvement of the disease and eventually to the disappearance of the epileptic crisis at this case.
BIBLIOGRAPHY
Andreoli, T.E., Carpenter, Ch.C.J., Bennett, J.C., Plum, F., 1999 – Cecil Essentials of Medicine, Editura MAST, Ediţia a IV a, Bucureşti.
Borundel, C., 2006 – Medicină internă pentru cadre medii, Editura All, Bucureşti. Covanis, A., 2006 Panayiotopoulos Syndrome: A Benign Childhood Autonomic Epilepsy Frequently Imitating Encephalitis, Syncope, Migraine, Sleep Disorder, or Gastroenteritis, Pediatrics, 118, 1237 1243.
Ion, V., Georgescu, Ş., Câmpeanu, A., Tufănoiu, E., Tudoran, C., Lupescu, I., 1999 Neurologie clinică, Editura All, Bucureşti.
Mcewan, M. J., Espie, C. A., Metcalfe, J., Brodie, M. J., Wilson, M. T., 2004 Quality of life and psychosocial development in adolescents with epilepsy: a qualitative investigation using focus group methods, Quality of Life Research, 13: 15–31.
Mihalaş, G., Goţia, S.R., 2000, Lucrări practice de fiziologie – Explorarea funcţională a aparatelor şi sistemelor, Editura UMFT, Timişoara.
68
Remschmidt, H., 1973, Psychological Studies of Patients with Epilepsy and Popular Prejudice, Epilepsia (Amst.), 14: 347 356.