w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Comparison
between
qualitative
and
real-time
polymerase
chain
reaction
to
evaluate
minimal
residual
disease
in
children
with
acute
lymphoblastic
leukemia
Francisco
Danilo
Ferreira
Paula
a,
Silvana
Maria
Elói-Santos
a,
Sandra
Guerra
Xavier
a,
Mônica
Aparecida
Ganazza
b,
Patricia
Yoshioka
Jotta
b,
José
Andrés
Yunes
b,c,
Marcos
Borato
Viana
a,
Juliana
Godoy
Assumpc¸ão
a,∗aUniversidadeFederaldeMinasGerais(UFMG),BeloHorizonte,MG,Brazil bCentroInfantilBoldrini,Campinas,SP,Brazil
cUniversidadeEstadualdeCampinas(UNICAMP),Campinas,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received26May2015
Accepted14August2015
Availableonline14September2015
Keywords:
Minimalresidualdisease
Polymerasechainreaction
Acutelymphoblasticleukemia
Leukemiafreesurvival
a
b
s
t
r
a
c
t
Introduction:Minimalresidualdiseaseisanimportantindependentprognosticfactorthat
canidentifypoorrespondersamongpatientswithacutelymphoblasticleukemia.
Objective:Theaimofthisstudywastoanalyzeminimalresidualdiseaseusing
immunoglob-ulin(Ig)andT-cellreceptor(TCR)generearrangementsbyconventionalpolymerasechain
reaction followed by homo-heteroduplex analysis and to compare this with real-time
polymerasechainreactionattheendoftheinductionperiodinchildrenwithacute
lym-phoblasticleukemia.
Methods:Seventy-fourpatientsdiagnosedwithacutelymphoblasticleukemiawereenrolled.
Minimalresidualdiseasewasevaluatedbyqualitativepolymerasechainreactionin57and
bybothtestsin44.TheKaplan–MeierandmultivariateCoxmethodsandthelog-ranktest
wereusedforstatisticalanalysis.
Results:Ninepatients(15.8%)werepositiveforminimalresidualdiseasebyqualitative
poly-merasechainreactionand11(25%)byreal-timepolymerasechainreactionconsideringa
cut-offpointof1×10−3forprecursorB-cellacutelymphoblasticleukemiaand1×10−2for
T-cellacutelymphoblasticleukemia.Usingthequalitativemethod,the3.5-year
leukemia-free survivalwassignificantlyhigherinchildrennegativeforminimalresidualdisease
comparedtothosewithpositiveresults(84.1%±5.6%versus41.7%±17.3%,respectively;
p-value=0.004).Therewasnosignificantassociationbetweenleukemia-freesurvivaland
minimalresidualdiseasebyreal-timepolymerasechainreaction.Minimalresidualdisease
byqualitativepolymerasechainreactionwastheonlyvariablesignificantlycorrelatedto
leukemia-freesurvival.
∗ Correspondingauthorat:LaboratóriodeBiologiaMolecular,UniversidadeFederaldeMinasGerais(UFMG),Av.ProfessorAlfredoBalena,
190,sala149,30130-100BeloHorizonte,MG,Brazil.
E-mailaddress:[email protected](J.G.Assumpc¸ão).
http://dx.doi.org/10.1016/j.bjhh.2015.08.003
1516-8484/©2015Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.PublishedbyElsevierEditoraLtda.Allrights
Conclusion: Giventhedifficultiesintheimplementationofminimalresidualdisease
mon-itoringbyreal-timepolymerasechainreactioninmosttreatmentcenters inBrazil,the
qualitativepolymerasechainreactionstrategymaybeacost-effectivealternative.
©2015Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Publishedby
ElsevierEditoraLtda.Allrightsreserved.
Introduction
Withcurrentcureratesof80–85%,moderntreatment
proto-colsforacutelymphoblasticleukemia(ALL)incorporaterisk
stratificationofpatients, inorder tointensifytreatment in
higher-riskpatientsandreduceadverseeffectsofthosewith
greaterprobabilityofcure.1
Several studies haveshown that the detection of
resid-ual leukemiccells,that isminimalresidual disease (MRD),
especiallyatthe end oftheinduction period,isan
impor-tantprognosticfactortoidentifypatientswithhigherriskof
relapse.2–4
Current ALL protocols use immunophenotyping byflow
cytometryorreal-timequantitativepolymerasechainreaction
(RQ-PCR)toevaluateMRD.Bothmethodsarehighlysensitive
andspecificbutcomplexandexpensive.5,6
TheevaluationofMRDbyflowcytometryisafast
quan-titativemethod thatrequires limited sample manipulation
and may reach sensitivities of 10−3 to 10−5 depending on
the number offluorochromes usedin theanalysis (from 3
to9).6However,theexpressionofantigensmayvaryduring
treatmentandnormalBprecursorcellsmayexpressmarkers
similartothoseoflymphoblastsinALL.7
Clonal immunoglobulin (Ig) and T cell receptor (TCR) gene
rearrangements havebeen widely used inMRD evaluation
becauseof theirhigh frequenciesinboth B-ALLand T-cell
acutelymphoblasticleukemia (T-ALL)cells.8 RQ-PCR
analy-sisofrearrangedIgandTCRgeneshashighsensitivity(10−4
to10−5),agooddegreeofstandardization,besidesthe
advan-tageofusingastablesample(DNA).Ontheotherhand,the
highcostandcomplexitymayhinderitsimplementationin
mostoncohematologyunitsindevelopingcountries.6
MRD analysis of Ig and TCR gene rearrangements can
alsobeaccomplishedbyqualitativePCRfollowedby
homo-heteroduplexanalysistodiscriminateclonalPCRamplicons,
amuchsimplermethod.Althoughlesssensitive(10−2to10−3),
the test can be used to identifypatients at higher risk of
relapse.9
Objective
ThisstudyaimedtocompareMRDresultsofqualitativePCR
andthegoldstandard,RQ-PCR.
Methods
Patients
Seventy-four consecutive zero- to 19-year-old patients
with a diagnosis of ALL were investigated. Patients were
identified in three leading institutions in Belo Horizonte,
Minas Gerais, Brazil: Hospital das Clínicas da
Universi-dade Federal de Minas Gerais (UFMG) (n=52); Hospital da
Baleia/Fundac¸ãoBenjaminGuimarães(n=14);andSantaCasa
deMisericórdiadeBeloHorizonte(n=8).Bonemarrow
sam-ples were collected from January 2010 to December 2012.
Most patients (n=45) were treated according to the Grupo
BrasileirodeTratamentodaLeucemiaInfantil-leucemia
lin-foideaguda(GBTLI-LLA-99)protocolalthough21patientswere
treatedaccordingtoGBTLI-LLA-2009,andeightpatientsusing
theAssociazioneItalianaEmatologiaedOncologiaPediatrica
(AIEOP-95)protocol.AccordingtotheGBTLI-LLA-99and2009
protocols,patientsolderthannineyearsatdiagnosisand/or
with awhite blood cell (WBC) countabove50×109/L were
assignedtothegroupwithhighriskofrelapseandtheothers
wereassignedtothelow-riskgroupandreceivedlessintensive
treatment.ApprovalwasobtainedfromtheEthicsCommittee
ofthethreeparticipatinginstitutionsandallguardiansand/or
patientsgavetheirinformedwrittenconsenttoparticipatein
thestudyaccordingtotheDeclarationofHelsinki.Nofamily
orpatientrefusedtosigntheinformedconsentform.
Diagnosticstudies
DiagnosisofALLwasmadebystandardmorphological
anal-ysisandbyflowcytometryimmunophenotyping.Karyotype
analysisandreversetranscriptionPCR(RT-PCR)werealso
per-formedatdiagnosisfortheBCR-ABL,TCF3/PBX1,ETV6/RUNX1
andMLL-AF4fusiongenes.
CellsamplesandDNAisolation
Bone marrow sampleswere obtained from the patientsat
diagnosis(Day0)andattheendoftheinductionperiod(Day
28forthosetreatedaccordingtoGBTLI-LLA-99protocol;Day
33forAIEOP-95;andDay35forGBTLI-LLA-2009).
Mononuclear cells were separated using Histopaque®
(Sigma–Aldrich, Saint Louis, USA) centrifugation gradient
and DNA was extracted with the NucleoSpin® Tissue Kit
(Macherey-Nagel, Düren, Germany) according to
manufac-turer’sinstructions.TheextractedDNAwasquantifiedusing
theNanoDrop2000TMSpectrophotometer.ThequalityofDNA
wasconfirmedthroughamplificationoftheFms-liketyrosine
kinase3(FLT3)gene,accordingtoMeshinchietal.10
Identificationofimmunoglobulin/Tcellreceptorminimal residualdiseasetargetsatdiagnosis
DNAfromdiagnosticsampleswasscreenedusing19primer
mixes according to the ALL subtype. For precursor B-cell
for the complete and incomplete IgH (VH-(DH)-JH, DH-JH),
IgK (Vk-Kde, Intron-Kde), TCRG (Vg-Jg1.3/2.3+Jg1.1/2.1) and
incompleteTCRDgene rearrangements(Vd2-Dd3,Dd2-Dd3)
wereused.11ForT-ALL,BIOMED2primersetsfortheIgH
(DH-JH),TCRG(Vg-Jg1.3/2.3+Jg1.1/2.1),TCRD(Vd-(Dd)-Jd1,Dd2-Jd1,
Vd2-Dd3,Dd2-Dd3)generearrangementsand forthe Sil-Tal
(Sil-Tal1,Sil-Tal2)microdeletionwereused.11,12
PCRwascarriedoutin25Lreactionscontaining25ngof
DNA,1U ofTthDNA polymerase(Biotools,Madrid, Spain),
10pmolofeachprimer,2mMofMgCl2,and100Mofeach
dNTP. The PCR amplification cycles have been previously
described.11,12TwonegativecontrolswereusedineachPCR
assay:onewithout DNAand the other containingpools of
polyclonalDNAobtainedfromperipheralbloodmononuclear
cells(PBL)fromtenhealthydonors.PCRproductswere
ana-lyzedbyhomo-heteroduplexanalysison12%acrylamidegels
stained withSybr Safe DNA gel stain (Invitrogen, USA), as
previouslydescribed.13Amplifiedgenerearrangementswere
characterizedasclonalwhenabandoftheexpectedsizewas
visible,11andnotpresentinthePBLcontrol.Theband
contain-ingtheclonalamplicon,accordingtotheexpectedmolecular
size,wascutfrom thegel,dissolvedinwaterandstoredat
−20◦Cforsubsequentsequencing.
Qualitativeminimalresidualdiseaseanalysis
ForMRDmonitoringbythequalitativemethod,atleasttwo
clonalmarkersidentifiedatdiagnosisweretested,whenever
possible. PCRs and homo-heteroduplex analyses were
car-riedoutasdescribedabove,exceptthat500ngofDNAwere
used.Day28–35samples,diagnosticDNAsamples,aswellas
thepolyclonalPBLDNAandthenon-templatecontrolswere
runinparallel.Follow-upsampleswereconsideredpositive
whentheyshowedthesamemigrationpatternandmolecular
weightasthesamplesatdiagnosis.
Sequencinganddesignofpatient-specificprimers
Clonal PCR products from Day 0 that had been dissolved
inwaterwere re-amplifiedin a volumeof 50Lusing the
sameprimersets(butwithT7orM13extensions)and
reac-tion conditions as described above. Sequencing reactions
werecarriedoutusingtheBigDyeTerminatorCycle
Sequenc-ing Reaction Kit (PE Applied Biosystems) and T7and M13
primers.SequenceswererunusingtheABIPrism3130Genetic
Analyzer (PE Applied Biosystems) and analyzed using the
ChromasLite2.4software(TechnelysiumPty Ltd.).
Patient-specificjunctionalregionsequenceswereidentifiedwiththe
Blasttool(http://blast.ncbi.nlm.nih.gov/Blast.cgi)and
IMGT/V-QUEST(http://www.imgt.org/IMGTvquest/share/textes/).
ThePrimer3Biotoolssoftware(http://biotools.umassmed.
edu/bioapps/primer3www.cgi)was used todesign
patient-specific primers complementary to the junctional region
sequence and compatible with primers and probes
previ-ouslydescribedforIgH,14IgK,15TCRG,16TCRD,17andSil-Tal.18
Twopatient-specificprimersweredesignedforeachIg/TCR
region. GCrich(>80%)junctional regionswere notused as
targets.
Patient-specificprimersweretestedforspecificityand
sen-sitivity.RQ-PCRanalysiswasperformedinduplicate,inafinal
volume of25Lcontaining100ngofDNA, 5M
sequence-specific TaqMan probes (Applied Biosystems), 7.5pmol of
eachprimer,andTaqManUniversalMastermix(2×)(Applied
Biosystems),ontheStepOnePlusTM RQ-PCRSystem(Applied
Biosystems).Resultswere analyzed withthe StepOne
soft-warev2.3andthesensitivitywasdefinedasthepointwith
thegreatestdilutioninwhichthecyclethreshold(Ct)reached
atleastoneCt belowthe lowestCt forpolyclonalPBL.The
primerwasconsideredmorespecificthegreaterthedifference
betweenthesensitivityofCtandthatofPBLCt.
Minimalresidualdiseaseusingreal-timepolymerase chainreaction
RQ-PCR MRDanalysisofDay28–35sampleswasperformed
andinterpretedaccordingtotheguidelinesofvanderVelden
etal.19RQ-PCRswerecarriedoutasdescribedabovefor
sen-sitivity tests,exceptthat500ngofDNAwere used.Results
werenormalizedusingN-RASasacontrolgene.18MRD
cut-offpointsweredefinedaccordingtotheGBTLI-2009protocol,
inwhichpatientswithresultsabove1×10−3forpB-ALLand
1×10−2 forT-ALLare considered positiveand classified as
poorrespondersattheendoftheinductiontherapy.
Statisticalanalysis
Overallsurvival(OS),event-freesurvival(EFS)and
leukemia-free survival (LFS) curves were plotted employing the
Kaplan–Meiermethod.TheOSwascalculatedfromthedateof
diagnosistothedateofdeathorlastfollow-up.TheEFSwas
calculatedfromthedateofdiagnosistothedateofrelapse
ordeath.TheLFSwascalculatedfromthedateofleukemia
remissiontothedateofrelapse(patientswhodiedin
remis-sionwascensoredonthedateofdeath).Thecut-offdatefor
censoringnon-relapsedpatientswas22October2014.Curves
fordifferentMRDgroupswerecomparedbythelog-ranktest
according to age, WBC countat diagnosis,
immunopheno-type,riskgroup,gender,institutionoforiginandtreatment
protocol. All statistical analyses were performed using the
StatisticalProgramfortheSocialSciences(SPSS)software
(ver-sion20.0)withthelevelofsignificancesetforp-values≤0.05.
The association between LFS, qualitative MRD and
RQ-PCR MRD results were adjusted for the effect of clinical
and biological categorical variables in a multivariate Cox
model.
Results
Themainclinicalandbiologicalcharacteristicsofpatientsat
diagnosisandintheinductionphasearedepictedinTable1.
Fourteenoutofthe74patientswerenottestedforgene
rearrangementsbecausetherewasnotenoughbonemarrow
materialformolecularbiologystudiesatdiagnosis,andtwo
patientsdiedduringtheinductionperiod.Thus,58patients
werescreenedforIg/TCRrearrangements.Atleastoneclonal
markerwasdetectedin57children(98.3%):47outof47(100%)
forpB-ALLand10out of11 (90.9%)forT-ALL.Twoormore
clonalmarkersweredetectedin46children(79.3%):41outof
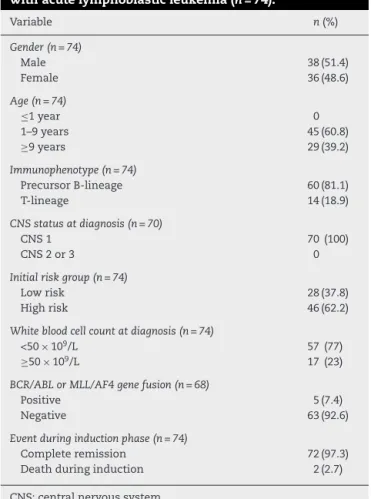
Table1–Clinicalandbiologicalvariablesofchildren withacutelymphoblasticleukemia(n=74).
Variable n(%)
Gender(n=74)
Male 38(51.4)
Female 36(48.6)
Age(n=74)
≤1year 0
1–9years 45(60.8)
≥9years 29(39.2)
Immunophenotype(n=74)
PrecursorB-lineage 60(81.1)
T-lineage 14(18.9)
CNSstatusatdiagnosis(n=70)
CNS1 70(100)
CNS2or3 0
Initialriskgroup(n=74)
Lowrisk 28(37.8)
Highrisk 46(62.2)
Whitebloodcellcountatdiagnosis(n=74)
<50×109/L 57(77)
≥50×109/L 17(23)
BCR/ABLorMLL/AF4genefusion(n=68)
Positive 5(7.4)
Negative 63(92.6)
Eventduringinductionphase(n=74)
Completeremission 72(97.3)
Deathduringinduction 2(2.7)
CNS:centralnervoussystem.
rearrangementswerenotbedetectedinonepatientwith T-ALL.
The most frequent rearrangement for pB-ALL was IgH (74.5%),followedbyTCRD(59.6%),IgK(53.2%)andTCRG(38.3%). ForT-ALL,themostfrequentrearrangementwasTCRG(90.9%), followedbySil-Tal1(18.2%).
Of the 57 patients with at least one clonal marker, 51 (89.5%)hadsuitabletargetsforthedesignofspecificprimers. Atotalof173primers(75forIgH,43forTCRD,33forTCRG and22forIgK)weredesignedandtestedforsensitivityand
specificity. PrimersfortheSil-Tal1 rearrangementwerealso testedintwopatients.IgH,IgKandSil-Tal1primersachieved highersensitivity(1×10−4)thanprimersforTCRGandTCRD.
AhighproportionofTCRGandTCRDprimerswereunspecific (66.7%and55.8%,respectively).Aftertestingthe175primers, 44patientshadatleastoneprimerthatwassuitablefor RQ-PCRmonitoringofMRD.
MRDevaluation
Attheendoftheinductiontherapy,9/57patients(15.8%)had positiveMRDbythequalitativeassay,12.8%(6/47)forpB-ALL and30%(3/10)forT-ALL.EightoutofthenineMRD-positive patientshadbeenassignedtothehigh-riskgroupatdiagnosis; oneofthemwasBCR-ABL-positiveandanotherwasMLL-AF4 -positive.Sensitivityoftheassaywiththequalitativeprimers was10−2to10−3.13
MRD analysis by RQ-PCR was performed in 14/44 (32%)
patients usingtwo markersandin 30(68%)using justone
marker.Twenty-sevenIgH,12IgK,fiveTCRGand11TCRD
rear-rangements were used.Eleven out ofthe44 patients(25%)
hadpositiveMRDatthecut-offlevelof10−3(pB-ALL)or10−2
(T-ALL); 10/39 (25.6%) pB-ALL patients and 1/5 (20%)T-ALL
patients.Eightoutofthe11hadbeenassignedtothe
high-riskgroupatdiagnosis;twoofthemwereBCR-ABL-positive
andanotherwasMLL-AF4-positive.Theobservedsensitivity
oftheassaywiththespecificprimersvariedfrom10−3to10−5.
AccordingtoMRDRQ-PCRcut-offpointsestablishedbythe
GBTLI-2009protocol,theagreementbetweenthetwomethods
using Kappastatistics was40%forpB-ALLand 100%for
T-ALL.Whenacut-offpointof1×10−2wasusedforpB-ALL,the
Kappacoefficientwas75%,andconsideringacut-offpointof
1×10−3forT-ALL,itwas50%(Table2).Mostdivergentresults
betweenassayswerepatientswithMRDloadsbetween10−2
and10−3,whichwerepositiveinRQ-PCRbutnegativein
con-ventionalPCR.
Analysisofoutcome
Theestimated3.5-yearprobabilitiesofOSandEFSwere73.6%
and68.2%,respectively,whiletheestimated3.5-year
probabil-ityofLFSwas72.3%(Figure1).
Table2–Comparativeanalysisofminimalresidualdiseasebyconventionalpolymerasechainreaction(PCR)and real-timequantitativepolymerasechainreaction(RQ-PCR).
RQ-PCR ConventionalPCR Concordance(%)
Negative Positive
pB-ALL(n=39)
>1×10−2 4 1 3 75.0
>1×10−3and≤1×10−2 6 5 1 16.7
<1×10−3a 29 29 0 100.0
T-ALL(n=5)
>1× 10−2a 1 0 1 100.0
>1× 10−3and≤1× 10−2 1 1 0 0
<1× 10−3 3 3 0 0
pB-ALL:precursor-Bcellacutelymphoblasticleukemia;T-ALL:T-cellacutelymphoblasticleukemia.
20
0.0 40 60 80 100
20
0.0 40 60 80 100
20
0.0 40 60 80 100
1.00
.00 2.00
Probability of overall survival, %
Probability of event-free survival, %
Probability of leukemia-free survival, %
n=74
A
B
C
n=74 n=72
Time (years)
3.00 4.00 5.00 .00 1.00 2.00 Time (years)
3.00 4.00 5.00 .00 1.00 2.00 Time (years)
3.00 4.00 5.00
Figure1–Kaplan–Meiersurvivalcurveestimatesfor(A)overallsurvivaland(B)event-freesurvivalofallpatients(n=74); and(C)leukemia-freesurvivalin72patients.
.00 0.0
20 40 60 80 100
1.00 2.00
MRD-positive (n=9) MRD-negative (n=48)
Cumulative survival,
%
Leukemia-free survival (years) 3.00
P=0.004
4.00 5.00
Figure2–Leukemia-freesurvivalof57childrenwithacute lymphoblasticleukemiaaccordingtominimalresidual diseasebasedonqualitativepolymerasechainreaction.
ThemediantimeofLFSforchildrenwithoutrelapsewas
3.0years(1.1–4.5years)fromthedateofmorphologicalbone
marrowremission.Themediantimefromremissiontorelapse
was1.2years(0.5–2.5years).The3.5-yearLFSwassignificantly
higher in qualitatively MRD-negative children (84.1±5.6%)
when compared to MRD-positive children (41.7±17.3%; p
-value=0.004)(Figure2).Therewasnosignificantassociation
betweenanyotheranalyzedclinicalorbiologicalvariablesand
LFS.Evendifferentprotocolshadnoimpactonsurvival(data
notshown).
LFSdataanalysisforqualitativeMRDresultswasrepeated
considering only patients evaluated by both techniques,
qualitative PCR and RQ-PCR (n=44). Again, qualitative
MRD-negativepatientshadsignificantlyhigherLFSthan
MRD-positivechildren(p-value=0.032;Supplementalfigure1).
.00 0.0
20 40 60 80 100
1.00 2.00
MRD-positive (n=11) MRD-negative (n=33)
Cumulative survival, %
Leukemia-free survival (years) 3.00
P=0.274
4.00 5.00
Figure3–Leukemia-freesurvivalaccordingtominimal residualdiseasebasedonreal-timequantitative polymerasechainreactionattheendofinductionin44 childrenwithacutelymphoblasticleukemia.
Cox’s regression model was used toassess the
progno-sticimpactofqualitativeMRDonLFS onDays28–35.After
adjustingfortheeffectofgender,institutionoforigin,
treat-mentprotocol,riskgroup,immunophenotype,WBCcountat
diagnosis and agein amultivariateanalysis, MRDwas the
onlyvariablesignificantlyassociatedwithLFS(p-value=0.015)
(Table3).
Afterexcludingnon-significantvariables,positiveMRDby
qualitative PCRon Days 28–35was significantlyassociated
withalowerLFS(p-value=0.009).Therelapseriskfor
posi-tiveMRDpatientsonDays28–35was4.6higherthanforthose
withnegativeMRD(95%confidenceinterval:1.5–14.6).
TherewasnosignificantassociationbetweenRQ-PCRMRD
and LFS (Figure 3).Analyzingthe individual data,onlyone
Table3–CoxmodelfortheprognosticinfluenceofminimalresidualdiseaseconsensusprimersonDays28–35onthe leukemia-freesurvivalof57childrenwithacutelymphoblasticleukemia.
Variable Degreesoffreedom Coefficient SE p-Value EstimatedRR(95%CI)
Institutionoforigin 2 0.642
Protocol 2 0.621
Gender 1 −0.375 0.694 0.589 0.687(0.176–2.678)
Riskgroup 1 0.550 1.090 0.614 1.733(0.205–14.689)
Agegroup 1 −1.392 1.294 0.282 0.249(0.020–3.138)
Immunophenotype 1 0.150 0.967 0.877 1.161(0.175–7.725)
WBCatdiagnosis 1 0.679 1.057 0.521 1.971(0.248–15.643)
QualitativeMRDD28–35 1 2.762 1.138 0.015 15.827(1.702–147.182)
SE:standarderror;RR:relativerisk;CI:confidenceinterval;WBC:whitebloodcellcount;MRDD28–35:minimalresidualdiseaseonDays28–35.
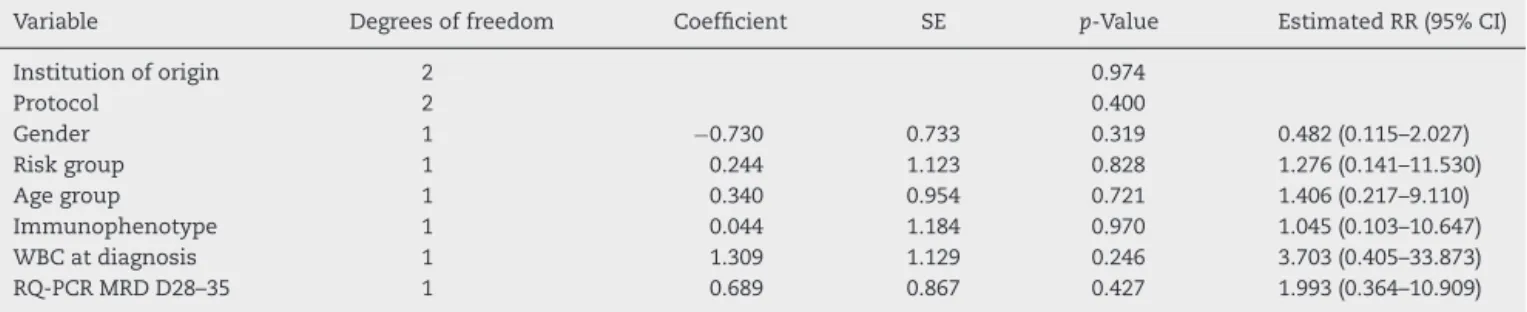
Table4–Coxmodelfortheprognosticinfluenceofminimalresidualdiseasebasedonreal-timequantitativepolymerase chainreaction(RQ-PCR)onDays28–35ontheleukemia-freesurvivalof44childrenwithacutelymphoblasticleukemia.
Variable Degreesoffreedom Coefficient SE p-Value EstimatedRR(95%CI)
Institutionoforigin 2 0.974
Protocol 2 0.400
Gender 1 −0.730 0.733 0.319 0.482(0.115–2.027)
Riskgroup 1 0.244 1.123 0.828 1.276(0.141–11.530)
Agegroup 1 0.340 0.954 0.721 1.406(0.217–9.110)
Immunophenotype 1 0.044 1.184 0.970 1.045(0.103–10.647)
WBCatdiagnosis 1 1.309 1.129 0.246 3.703(0.405–33.873)
RQ-PCRMRDD28–35 1 0.689 0.867 0.427 1.993(0.364–10.909)
SE:standarderror;RR:relativerisk;CI:confidenceinterval;WBC:whitebloodcellcount;MRDD28–35:minimalresidualdiseaseonDays28–35.
andnegativequalitativeMRDrelapsedsofar,afteroneyearof remission.Theremainingfivearealiveandwithoutrelapsing for3.2–4.0yearssincetheinitialremission.
Cox’sregression model was usedto determinethe pro-gnosticimpactofRQ-PCRMRDonDays 28–35onLFS.After adjustingfortheeffectofgender,institutionoforigin, treat-mentprotocol,riskgroup,WBCcountatdiagnosis,ageand immunophenotypeinamultivariateanalysis,novariablewas statisticallyassociatedwithLFS, includingRQ-PCR MRD(p -value=0.427;Table4).
Discussion
Riskstratificationisstillachallengingissueinthetreatmentof
childrenwithALL.ThestratificationofpatientsbasedonMRD
definedbyIg/TCRmarkersusingPCRattheendofinduction
therapywasincludedintheBrazilianprotocolsforthefirst
timein2009andisstillunderevaluation.20Thepresentstudy
aimedtocomparealow-costPCR-basedtechniqueof
detec-tion and monitoring MRD withthe gold standard method,
RQ-PCR.
Thedetectionofatleastoneclonalrearrangementin98.3%
ofpatients tested byPCR supports the applicability ofthe
GBTLI-2009strategyforthescreeningofrearrangementsin
thevastmajorityofchildrenwithALL.
For pB-ALL patients, the prevalence of rearrangements
was similar to that found by van der Velden et al., Flohr
et al., and two other Brazilian studies using the same
methodology.9,13,21,22Themostcommonofthe19clonal
rear-rangements screened was IgH, followed by TCRD and IgK,
as observedby Thorn et al.23 In T-ALL, the most frequent
rearrangement was TCRG, in line with other studies.9,13,24
Frequency oftheSIL-TAL1 rearrangement (18.2%)isalsoin
agreementwithfindingsfromotherBraziliangroups.25
Inthepresentstudy,twoormoreclonalrearrangements
weredetectedin87%ofthepB-ALLandin45%oftheT-ALL
patients.SincemostresearchersproposetwotargetsforMRD
monitoring,5thereisaneedtoincreaseT-ALLtargets.
According to vander Velden, the sensitivity ofthe
RQ-PCRassaydependsonseveralfactors,includingthetypeof
rearrangement.26Inthis study,primerssynthesizedforIgH
andIgKrearrangementswerethemostsensitiveandspecific
asinpreviousreports,27andshouldbethefirstchoiceforMRD
monitoringinpB-ALL.ThelowspecificityofTCRG
rearrange-ments(onlytwoofthenineprimerstestedwereapprovedin
thesensitivityandspecificitytests)couldbeduetothesizeof
theNregion,16althoughthisaspectwasnotevaluatedinthe
presentstudy.
MRD by qualitative PCR was positive on Days 28–35 in
15.8%ofthepatientsinthisstudy,afigurewithintherange
describedpreviouslybyScridelietal.usingasimilar
method-ology (13.2%).9 MRDby RQ-PCR was positivein 25% ofthe
patientsattheendofinduction.
Comparing the qualitative and quantitative techniques,
this study found a 40% agreement for pB-ALL and 100%
for T-ALL. All negative cases in the quantitative test were
also negativeinthe qualitative test. TheGBTLI-2009
refer-encelaboratoryfromCentroInfantilBoldrini(Campinas,SP,
Brazil)reporteda68%agreementbetweenthetwomethods
forpB-ALL(n=121)and100%forT-ALL(n=9)inanongoing
prospectivestudy(personalcommunication).Thediscordance
ratebetweenthetwoassaysforpB-ALLisnotsurprisingsince
thereforethequalitativetestmaymisspB-ALLpatients
char-acterizedaspositivebythequantitativeassaywithacut-off
pointof10−3.
SeveralclinicaltrialsthatstratifypatientsbasedonRQ-PCR
MRDhaveshownthat molecularresponseishighly
predic-tiveforrelapseinchildhoodALL.28–30 Inthis studyMRDby
qualitativePCR wasthe single variable that showeda
sta-tistically significant association with the LFS. Surprisingly,
RQ-PCRMRDshowednoassociation,incontrasttowhathas
beenobservedinotherstudies.22,30 Itisimportanttopoint
outthatthefollow-uptimeofthepresentstudyisrelatively
shortand patients who had beenMRD-positive byRQ-PCR
mayrelapselateron.Moreover,thenumberofpatients
eval-uatedwasratherlow.Itispossiblethattheeffectoflow-level
MRDonoutcomedetectedbyRQ-PCRwouldbeevidenthad
a larger group of patients been studied. In addition, MRD
wasstudiedatjustonetimepointwhileotherstudies
eval-uated the kinetics of MRD from the end of induction to
maintenanceattwotimepoints.6,28 Thelackofassociation
betweenRQ-PCRdataandLFSinthisstudyisintriguingand
needstobefurtherexaminedinalargercohortwithalonger
follow-up.
ItisinterestingtohighlightthatsixpB-ALLpatientswith
aMRDloadcloseto10−3 wereidentifiedaspositiveby
RQ-PCRbutnegativebyqualitativePCR.Asalreadystated,only
onepatienthasrelapsedsofar.Perhapsthesensitivityofthe
qualitativeassaymaybeenoughtoidentifypatientswitha
relativelyhigh-levelMRDwhoareatahigherriskofrelapse
andneedintensificationoftherapyoralternative protocols
thatcouldavoidrelapse.
Conclusions
TheRQ-PCRmethodishighlysensitiveandspecificasreported
bymanyinstitutionsallovertheworld.TheGBTLI-2009
proto-colalsorecommendsthismethodforMRDanalysisinchildren
withALL.Thepresentstudy,however,suggeststhat
primer-basedMRDattheendofinductionseemstobeaneffective
alternativetoassignrisktochildrenwithALL.Undoubtedly,
itisasimpleandcost-effectivestrategyforinstitutionsand
countrieswithlimitedtechnicalandfinancialresources.
Conflicts
of
interest
Theauthorsdeclarenoconflictofinterest.
Acknowledgments
Wewould like tothank all patients and their families for
takingpart inthis research. Wewould like to thanksome
medicaldoctors,especiallyJoaquimCaetanodeAguirreNeto
andAlvaroPimentaDutra(SantaCasadeMisericórdia,BH),
EduardoRibeiroLima(HospitaldaBaleia,Fundac¸ãoBernardo
Guimarães,BH),BenignaMariadeOliveira,CybeledeAndrade
Paes and Mitiko Murao (Hospital das Clínicas da
Univer-sidade Federal de Minas Gerais). We also thank Valéria
CristinaCâmaraforthetechnicalsupport.Thisworkwas
sup-portedbyConselhoNacionaldeDesenvolvimentoCientíficoe
Tecnológico(CNPq)andFundac¸ãodeAmparoàPesquisade
MinasGerais(FAPEMIG).
MBV and JAY have research grants from CNPq
(Brazil-ian ResearchCouncil), Brazil. Thiswork was supportedby
grantsfromFundac¸ãodeAmparoàPesquisadeMinasGerais
(FAPEMIG)toMBVandRonaldMcDonaldInstitute(79/2011)to
JAY.
Appendix
A.
Supplementary
data
Supplementarydataassociatedwiththisarticlecanbefound,
intheonlineversion,atdoi:10.1016/j.bjhh.2015.08.003.
r
e
f
e
r
e
n
c
e
s
1.vanderVeldenVH,JoostenSA,WillemseMJ,vanWeringER, LankesterAW,vanDongenJJ,etal.Real-timequantitativePCR fordetectionofminimalresidualdiseasebeforeallogeneic stemcelltransplantationpredictsoutcomeinchildrenwith acutelymphoblasticleukemia.Leukemia.2001;15(9):1485–7. 2.vanDongenJJ,SeriuT,Panzer-GrumayerER,BiondiA,
Pongers-WillemseMJ,CorralL,etal.Prognosticvalueof minimalresidualdiseaseinchildhoodacutelymphoblastic leukemia:aprospectivestudyoftheInternationalBFMStudy Group.Lancet.1998;352(9142):1731–8.
3.CavéH,vanderWerfftenBoschJ,SuciuS,GuidalC, WaterkeynC,OttenJ,etal.Clinicalsignificanceofminimal residualdiseaseinchildhoodacutelymphoblasticleukemia. EuropeanOrganizationforResearchandTreatmentofCancer ChildhoodLeukemiaCooperativeGroup.NEnglJMed. 1998;339(9):591–8.
4.DworzakMN,FröschlG,PrintzD,MannG,PötschgerU, MühleggerN,etal.Prognosticsignificanceandmodalitiesof flowcytometricminimalresidualdiseasedetectionin childhoodacutelymphoblasticleukemia.Blood. 2002;99(6):1952–8.
5.CazzanigaG,BiondiA.Molecularmonitoringofchildhood acutelymphoblasticleukemiausingantigenreceptorgene rearrangementsandquantitativepolymerasechainreaction technology.Haematologica.2005;90(3):382–90.
6.SchrappeM.Minimalresidualdisease:optimalmethods, timing,andclinicalrelevanceforanindividualpatient. HematolAmSocHematolEducProgram.2012;2012:137–42. 7.KroftSH.Roleofflowcytometryinpediatric
hematopathology.AmJClinPathol.2004;122Suppl1:S19–32. 8.Szczepa ´nskiT,BeishuizenA,Pongers-WillemseMJ,HählenK,
VanWeringER,WijkhuijsAJ,etal.Cross-lineageTcell receptorgenerearrangementsoccurinmorethanninety percentofchildhoodprecursor-Bacutelymphoblastic leukemias:alternativePCRtargetsfordetectionofminimal residualdisease.Leukemia.1999;13(2):196–205.
9.ScrideliCA,Assumpc¸ãoJG,GanazzaMA,AraújoM,ToledoSR, LeeML,etal.AsimplifiedMinimalResidualDisease(MDR) PCRmethodatearlytreatmentpointsstratifieschildrenwith acutelymphoblasticleukemiaintogoodandpooroutcome groups.Haematologica.2009;94(6):781–9.
10.MeshinchiS,WoodsWG,StirewaltDL,SweetserDA,Buckley JD,TjoaTK,etal.Prevalenceandprognosticsignificanceof Flt3internaltandemduplicationinpediatricacutemyeloid leukemia.Blood.2001;97(1):89–94.
11.vanDongenJJ,LangerakAW,BrüggemannM,EvansPA, HummelM,LavenderFL,etal.Designandstandardizationof PCRprimersandprotocolsfordetectionofclonal
suspectlymphoproliferations:reportoftheBIOMED-2 ConcertedActionBMH4-CT98-3936.Leukemia. 2003;17(12):2257–317.
12.Pongers-WillemseMJ,SeriuT,StolzF,d’AnielloE,GameiroP, PisaP,etal.Primersandprotocolsforstandardizeddetection ofminimalresidualdiseaseinacutelymphoblasticleukemia usingimmunoglobulinandTcellreceptorgene
rearrangementsandTAL1deletionsasPCRtargets:reportof theBIOMED-1CONCERTEDACTION:investigationofminimal residualdiseaseinacuteleukemia.Leukemia.
1999;13(1):110–8.
13.Assumpc¸ãoJG,GanazzaMA,deAraújoM,SilvaAS,Scrideli CA,BrandaliseSR,etal.Detectionofclonalimmunoglobulin andT-cellreceptorgenerearrangementsinchildhoodacute lymphoblasticleukemiausingalow-costPCRstrategy.Pediatr BloodCancer.2010;55(7):1278–86.
14.VerhagenOJ,WillemseMJ,BreunisWB,WijkhuijsAJ,Jacobs DC,JoostenSA,etal.ApplicationofgermlineIGHprobesin real-timequantitativePCRforthedetectionofminimal residualdiseaseinacutelymphoblasticleukemia.Leukemia. 2000;14(8):1426–35.
15.vanderVeldenVH,WillemseMJ,vanderSchootCE,Hahlen K,vanWeringER,vanDongenJJ.Immunoglobulinkappa deletingelementrearrangementsinprecursor-Bacute lymphoblasticleukemiaarestabletargetsfordetectionof minimalresidualdiseasebyreal-timequantitativePCR. Leukemia.2002;16(5):928–36.
16.vanderVeldenVH,WijkhuijsJM,JacobsDC,vanWeringER, vanDongenJJ.Tcellreceptorgammagenerearrangements astargetsfordetectionofminimalresidualdiseaseinacute lymphoblasticleukemiabyreal-timequantitativePCR analysis.Leukemia.2002;16(7):1372–80.
17.SzczepanskiT,vanderVeldenVH,HoogeveenPG,deBrieM, JacobsDC,vanWeringER,etal.Vdelta2-Jalpha
rearrangementsarefrequentinprecursor-B-acute lymphoblasticleukemiabutarerareinnormallymphoid cells.Blood.2004;103(10):3788–804.
18.ChenX,PanQ,StowP,BehmFG,GoorhaR,PuiC-H,etal. QuantificationofminimalresidualdiseaseinT-lineageacute lymphoblasticleukemiawiththeTAL-1deletionusinga standardizedreal-timePCRassay.Leukemia.
2001;15(1):166–70.
19.vanderVeldenVH,Panzer-GrümayerER,CazzanigaG,Flohr T,SuttonR,SchrauderA,etal.OptimizationofPCR-based minimalresidualdiseasediagnosticsforchildhoodacute lymphoblasticleukemiainamulti-centersetting.Leukemia. 2007;21(4):706–13.
20.GBTLI.GrupoBrasileiroparaoTratamentodeLeucemia Infantil.Protocolodetratamentodaleucemialinfoideaguda emcrianc¸as.SociedadeBrasileiradeOncologiaPediátrica; 2009.
21.vanderVeldenVH,SzczepanskiT,WijkhuijsJM,HartPG, HoogeveenPG,HopWC,etal.Age-relatedpatternsof immunoglobulinandT-cellreceptorgenerearrangementsin precursor-B-ALL:implicationsfordetectionofminimal residualdisease.Leukemia.2003;17(9):1834–44.
22.FlohrT,SchurauderA,CazzanigaG,Panzer-GrümayerR,van derVeldenV,FischerS,etal.Minimalresidual
disease-directedriskstratificationusingreal-time quantitativePCRanalysisofimmunoglobulinandT-cell receptorgenerearrangementsintheinternational multicentertrialAIEOP-BFMALL2000forchildhoodacute lymphoblasticleukemia.Leukemia.2008;22(4):771–82. 23.ThornI,ForestierE,ThuressonB,WasslavikC,MalecM,LiA,
etal.ApplicabilityofIG/TCRgenerearrangementsastargets forminimalresidualdiseaseassessmentina
population-basedcohortofSwedishchildhoodacute lymphoblasticleukaemiadiagnosed2002–2006.EurJ Haematol.2009;84(2):117–27.
24.GanazzaMA,Assumpc¸ãoJG,deAraújoM,ScrideliCA,Tone LG,BrandaliseSR,etal.TCRGgenerearrangementpatternsin BrazilianchildrenwithALL:anupdate.LeukRes.
2009;33(12):228–9.
25.MansurMB,EmerencianoM,BrewerL,Sant’AnaM, Mendonc¸aN,ThulerLC,etal.SIL-TAL1fusiongenenegative impactinT-cellacutelymphoblasticleukemiaoutcome.Leuk Lymphoma.2009;50(8):1318–25.
26.VanderVeldenVH,WillemseMJ,VanderSchootCE,Hählen K,VanWeringER,VanDongenJ.Immunoglobulinkappa deletingelementrearrangementsinprecursor-Bacute lymphoblasticleukemiaarestabletargetsfordetectionof minimalresidualdiseasebyreal-timequantitativePCR. Leukemia.2002;16(5):928–36.
27.SalariF,ShahjahaniM,ShahrabiS,SakiN.Minimalresidual diseaseinacutelymphoblasticleukemia:optimalmethods andclinicalrelevance,pitfallsandrecentapproaches.Med Oncol.2014;31(11):266.
28.ConterV,BartramCR,ValsecchiMG,SchrauderA,
Panzer-GrumayerR,MörickeA,etal.Molecularresponseto treatmentredefinesallprognosticfactorsinchildrenand adolescentswithB-cellprecursoracutelymphoblastic leukemia:resultsin3184patientsoftheAIEOP-BFMALL2000 study.Blood.2010;115(16):3206–14.
29.KarsaM,DallaPozzaL,VennNC,LawT,ShiR,GilesJE,etal. ImprovingtheidentificationofhighriskprecursorBacute lymphoblasticleukemiapatientswithearlierquantification ofminimalresidualdisease.PLoSOne.2013;8(10):e76455. 30.PaganinM,FabbriG,ConterV,BarisoneE,PolatoK,Cazzaniga