rev bras hematol hemoter. 2015;37(6):366–368
w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Scientific
Comment
Qualitative
polymerase
chain
reaction
versus
quantitative
polymerase
chain
reaction
for
the
detection
of
minimal
residual
disease
in
children
with
acute
lymphoblastic
leukemia
夽
Carlos
Alberto
Scrideli
∗,
Luiz
Gonzaga
Tone
UniversidadedeSãoPaulo(USP),RibeirãoPreto,SP,Brazil
Inacute lymphoblastic leukemia (ALL),remission is classi-callydefinedasthereestablishmentofnormalhematopoiesis andthepresenceoflessthan5%ofthenucleatedblastcell populationfound byconventional microscopy;this is used inolderprotocolstoassesstreatmentresponse. Morpholog-icalanalysis,althoughuseful and applicableatany center, hasproventobeoflimitedsensitivity,subjectiveand impre-cisetostudyearlyresponsetotreatmentandthistechnique doesnotappeartobesufficienttoidentifypatientsattrue riskofrelapsewhomightbenefitfromtheintensificationof treatment.1,2Forthisreason,cytomorphologicalanalysishas
beenreplacedbyminimalresidualdisease(MRD)monitoring inseveraltreatmentprotocolsandnewdefinitionsof remis-sionandrelapseinchildhoodALLhavebeenproposed.3
TheanalysisofMRDhasprovedtobethestrongest inde-pendentprognosticfactorinallstudiesanalyzinglargeseries ofpatientswithB-lineageandT-cellALL,andspecific molec-ularsubgroupssuchaspatientswiththeBCR-ABLfusiongene andALLpatientswithMLLgenerearrangements.This analy-sisallowsmoreaccurateriskgroupassignmentandtailoring theintensityoftreatment,permittingreductionor intensifi-cationatthedifferenttreatmenttimepointsaccordingtothe MRDlevel.4–9MRDmonitoringcanalsoguidetreatment
deci-sionsinrelapsedpatientsandthosewhoarecandidatesfor bonemarrowtransplantation.4,5,10,11
DOIoforiginalarticle:http://dx.doi.org/10.1016/j.bjhh.2015.08.003. 夽
SeepaperbyPaulaetal.onpages373–80.
∗ Correspondingauthorat:DepartamentodePuericulturaePediatria,FaculdadedeMedicinadeRibeirãoPreto,UniversidadedeSãoPaulo
(USP),AvenidaBandeirantes,3900,14049-900RibeirãoPreto,SP,Brazil. E-mailaddress:[email protected](C.A.Scrideli).
SequentialmonitoringofMRDusingmoresensitiveand specific techniques, such as quantitative real-time poly-merase chainreaction (RQ-PCR) forimmunoglobulin(Ig) and T-cellreceptor(TCR)generearrangementsandflowcytometry analysis,withadetectionpowerofoneblastcellin104–106
normal cells, has substantially refined the assessment of early response to treatment. Unfortunatelythese methods arenotonlyexpensive,buttechnicallycomplexandrequire considerable technologyandhighly-specializedlaboratories toberoutinely usedinriskstratificationprotocols forALL; they are therefore inaccessible to mosttreatment centers, especially in developing countries.4,12 The development
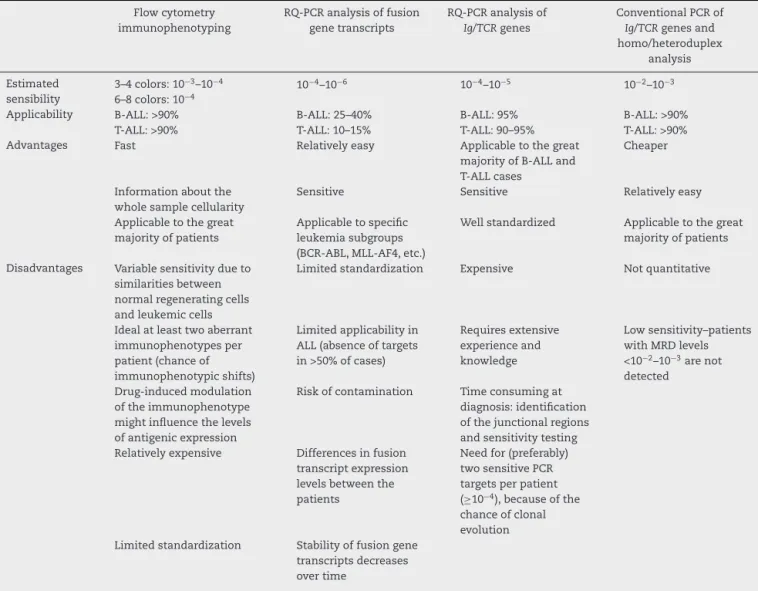
of simplified MRD technologies is essential to allow the potential benefitsofMRDmonitoring tobeextendedtoall childrenwithleukemiaincludingthosetreatedinlow-budget countries. Table 1shows some characteristics ofthe main methodologiesusedtodetectMRDinALL.
A clinically useful simplified MRD technique should be economicallyviable,widelyapplicable,specificandsensitive enough topredict thecourseofthe disease.Thedetection of clonal Ig and TCR rearrangements by PCR and homo-heteroduplex analysis has proved to bea rapidand much simplerandcheapermethodthanthe useofclone-specific probes or flow cytometry. In a multicenter retrospective study,thiswasthestrongestindependentprognosticfactor
http://dx.doi.org/10.1016/j.bjhh.2015.08.010
revbrashematolhemoter.2015;37(6):366–368
367
Table1–Characteristicsofthemethodologiesusedforminimalresidualdiseasedetectioninacutelymphoblastic leukemia(ALL)a.
Flowcytometry immunophenotyping
RQ-PCRanalysisoffusion genetranscripts
RQ-PCRanalysisof Ig/TCRgenes
ConventionalPCRof Ig/TCRgenesand homo/heteroduplex
analysis
Estimated sensibility
3–4colors:10−3–10−4 10−4–10−6 10−4–10−5 10−2–10−3
6–8colors:10−4
Applicability B-ALL:>90% B-ALL:25–40% B-ALL:95% B-ALL:>90%
T-ALL:>90% T-ALL:10–15% T-ALL:90–95% T-ALL:>90%
Advantages Fast Relativelyeasy Applicabletothegreat
majorityofB-ALLand T-ALLcases
Cheaper
Informationaboutthe wholesamplecellularity
Sensitive Sensitive Relativelyeasy
Applicabletothegreat majorityofpatients
Applicabletospecific leukemiasubgroups (BCR-ABL,MLL-AF4,etc.)
Wellstandardized Applicabletothegreat majorityofpatients
Disadvantages Variablesensitivitydueto similaritiesbetween normalregeneratingcells andleukemiccells
Limitedstandardization Expensive Notquantitative
Idealatleasttwoaberrant immunophenotypesper patient(chanceof immunophenotypicshifts)
Limitedapplicabilityin ALL(absenceoftargets in>50%ofcases)
Requiresextensive experienceand knowledge
Lowsensitivity–patients withMRDlevels <10−2–10−3arenot
detected Drug-inducedmodulation
oftheimmunophenotype mightinfluencethelevels ofantigenicexpression
Riskofcontamination Timeconsumingat diagnosis:identification ofthejunctionalregions andsensitivitytesting Relativelyexpensive Differencesinfusion
transcriptexpression levelsbetweenthe patients
Needfor(preferably) twosensitivePCR targetsperpatient (≥10−4),becauseofthe
chanceofclonal evolution Limitedstandardization Stabilityoffusiongene
transcriptsdecreases overtime
PCR:polymerasechainreaction;RQ-PCR:quantitativerealtimepolymerasechainreaction;Ig:immunoglobulingene;TCR:T-cellreceptorgene; B-ALL:B-lineageALL;T-All:T-cellALL.
a BasedonvanDongenetal.4,Schrappeetal.12andConteretal.13
inpatientstreatedaccordingtotheGrupoBrasileirode Trata-mentodaLeucemiaInfantil-leucemialinfoideagudaprotocol 1999(GBTLI-99).13 Thismethodrepresentsagoodpredictive
criterionofunfavorablecourseinchildrenwithALLasitisable inidentifypatientswithahighriskofrelapse.Thismethod, however, was not truly quantitative and, due to its lower sensitivity,it should beemployedonlytoidentifypatients withahighresidualtumorload.
ActuallyintheGBTLI-2009protocols,MRDanalysisatDays 14 and 35 ofthe inductionphase has been used to strat-ifypatientsasgoodandpoorresponders,guidingtreatment decisions in all pediatric ALL subtypes.14 Due to the cost
andtechnicalcomplexity,MRDanalysisusingpatientspecific probesbyRQ-PCRhasbeenroutinelyusedinveryfew treat-mentcentersinBrazilandnocomparisonofthismethodwith simplifiedMRDstrategiestodetectIgorTCRclonal rearrange-mentsbyconventionalPCRandhomo-heteroduplexanalysis hasbeenpublisheduntilnow.
In this issue of the Revista Brazileira de Hematology e Hemoterapy,Paulaetal.15comparedMRDmonitoringusingIg
368
revbrashematolhemoter.2015;37(6):366–368ALLusingthesameprotocolisessentialtodefinethereal util-ityofthissimplifiedstrategyinthetreatmentstratification.
Conflicts
of
interest
Theauthorsdeclarenoconflictofinterest.
r
e
f
e
r
e
n
c
e
s
1. CazzanigaG,BiondiA.Molecularmonitoringofchildhood acutelymphoblasticleukemiausingantigenreceptorgene rearrangementsandquantitativepolymerasechainreaction technology.Haematologica.2005;90(3):382–90.
2. StanullaM,SchrauderA.Bridgingthegapbetweenthenorth andsouthoftheworld:thecaseoftreatmentresponsein childhoodacutelymphoblasticleukemia.Haematologica. 2009;94(6):748–52.
3. SchnittgerS.Minimalresidualdiseasemonitoring:anewera forchildhoodALL.LancetOncol.2015;16(4):362–4.
4. vanDongenJJ,vanderVeldenVH,BrüggemannM,OrfaoA. Minimalresidualdiseasediagnosticsinacutelymphoblastic leukemia:needforsensitive,fast,andstandardized technologies.Blood.2015;125(26):3996–4009.
5. VoraA,GouldenN,MitchellC,HancockJ,HoughR,Rowntree C,etal.Augmentedpost-remissiontherapyforaminimal residualdisease-definedhigh-risksubgroupofchildrenand youngpeoplewithclinicalstandard-riskand
intermediate-riskacutelymphoblasticleukaemia(UKALL 2003):arandomisedcontrolledtrial.LancetOncol. 2014;15(8):809–18.
6. PuiCH,PeiD,Coustan-SmithE,JehaS,ChengC,BowmanWP, etal.Clinicalutilityofsequentialminimalresidualdisease measurementsinthecontextofrisk-basedtherapyin childhoodacutelymphoblasticleukaemia:aprospective study.LancetOncol.2015;16(4):465–74.
7. BorowitzMJ,WoodBL,DevidasM,LohML,RaetzEA,Salzer WL,etal.Prognosticsignificanceofminimalresidualdisease
inhighriskB-ALL:areportfromChildren’sOncologyGroup studyAALL0232.Blood.2015;126(8):964–71.
8.SchrappeM,ValsecchiMG,BartramCR,SchrauderA, Panzer-GrümayerR,MörickeA,etal.LateMRDresponse determinesrelapseriskoverallandinsubsetsofchildhood T-cellALL:resultsoftheAIEOP-BFM-ALL2000study.Blood. 2011;118(8):2077–84.
9.ConterV,BartramCR,ValsecchiMG,SchrauderA,
Panzer-GrümayerR,MörickeA,etal.Molecularresponseto treatmentredefinesallprognosticfactorsinchildrenand adolescentswithB-cellprecursoracutelymphoblastic leukemia:resultsin3184patientsoftheAIEOP-BFMALL2000 study.Blood.2010;115(16):3206–14.
10.EckertC,HagedornN,SramkovaL,MannG,Panzer-Grümayer R,PetersC,etal.Monitoringminimalresidualdiseasein childrenwithhigh-riskrelapsesofacutelymphoblastic leukemia:prognosticrelevanceofearlyandlateassessment. Leukemia.2015;29(8):1648–55.
11.ConterV,ValsecchiMG,ParasoleR,PuttiMC,LocatelliF, BarisoneE,etal.Childhoodhigh-riskacutelymphoblastic leukemiainfirstremission:resultsafterchemotherapyor transplantfromtheAIEOPALL2000study.Blood. 2014;123(10):1470–8.
12.Szczepa ´nskiT.Whyandhowtoquantifyminimalresidual diseaseinacutelymphoblasticleukemia?Leukemia. 2007;21(4):622–6.
13.ScrideliCA,Assumpc¸ãoJG,GanazzaMA,AraújoM,ToledoSR, LeeML,etal.Asimplifiedminimalresidualdisease
polymerasechainreactionmethodatearlytreatmentpoints canstratifychildrenwithacutelymphoblasticleukemiainto goodandpooroutcomegroups.Haematologica.
2009;94(6):781–9.
14.GBTLI(GrupoBrasileiroparaoTratamentodeLeucemia Infantil).Protocolodetratamentodaleucemialinfóideaguda emcrianc¸as.SocBrasOncolPediátr.2009.
15.PaulaFD,SantosSM,XavierSG,GanazzaMA,JottaP,YunesJE, etal.Comparisonbetweenqualitativeandreal-time