Original Article
Influence of Financial Subsidy and venue on Advanced Cardiac Life
Support courses, in the Learning of Cardiovascular Emergency
Heberth C. Miotto
1,2,3, Eugênio M. A. Goulart
1,2, Carlos Faria Santos Amaral
1,2, Maria da Consolação V. Moreira
1,2 School of Medicine, Federal University of Minas Gerais1, Department of Internal Medicine, Federal University of Minas Gerais2, Internal Medicine Postgraduate Program, Medical School,Federal University of Minas Gerais3, Belo Horizonte, MG - BrazilSummary
Background: The success in learning of emergency depends on many factors that can be summarized as: student, instructors and course.
Objective: To evaluate the influence of financial subsidy and venue of course in learning cardiovascular emergency.
Methods: Data were analyzed regarding the courses of Advanced Cardiac Life Support (ACLS) in the period from December 2005 to December 2006. In agreement with the financial subsidy, they were divided in: group 1 - integral
subsidy; group 2 - subsidy of 50%; and group 3 - without subsidy. As for the venue of the course, they were divided
in: locality A - study in city with> 1 million inhabitants; and locality B - study in city with <1 million inhabitants. The practical and theoretical approval and the theoretical average were compared.
Results: 819 students participated in ACL: 199 (24%) in group 1, 122 (15%) in 2 and 498 (61%) in 3. The practical and theoretical approval and the average in the theoretical exam were greater in group 3 than in other groups (p <0.05). Four hundred and eighty two (482) took the course in venue A (59%) and 337 (41%) in venue B. The practical approval was similar for both groups (p = 0.33), however the theoretical approval was greater in venue A (73% vs. 65% - p = 0.021 - OR = 1.44 and IC: 1.05 - 1.97). The theoretical average was greater in venue A (87.1 ± 10.4
and 86 ± 11, respectively p <0.05).
Conclusion: The financial subsidy and venue of the course had influence in the theoretical and practical approval. (Arq
Bras Cardiol 2008; 90(3):172-175)
Key words: Cardiopulmonary resuscitation; education, medical, continuing; heart arrest; health education; emergency; advanced cardiac life support - (ACLS).
Mailing address: Heberth C. Miotto •
Rua Paracatu , 1555/1202 - Santo Agostinho - 30180-091 - Belo Horizonte, MG - Brazil
E-mail: [email protected], [email protected]
Manuscript received August 04, 2007; revised manuscript received October 15, 2007; accepted October 31, 2007.
Introduction
The courses of Advanced Cardiac Life Support - (ACLS) are destined for teaching of cardiovascular emergency1. The training in emergency is associated with the improvement of survival in the pre-hospital and hospital cardio-respiratory arrest, however the retention of knowledge and the pschycomotor ability for accomplishment of the cardiopulmonary resuscitation still remains a problema2-8. The success in learning of cardiovascular emergency depends on several factors, that can be summarized in three: student, instructor and course.
The purpose of the present study is to analyze, in retrospect, the influence of integral or partial financial subsidy and venue of course in the immediate learning of Advanced Cardiac Life Support (ACLS).
Methods
We selected regular ACLS courses between December 2005 and December 2006. Participants in the course were physicians and nurses who sought the training spontaneously or for demand of some institution, and for the latter,some degree of subsidy was supplied.
The courses were classified according to financial aid and venue. In agreement with the financial subsidy, they were organized: group 1 (100% paid for by some institution), group 2 (50% paid for by some institution) and group 3 (integrally paid for by the student). As for the venue, the following classification was determined: venue A (larger urban center with more than a million inhabitants) and venue B (smaller urban center with less than a million inhabitants). The population definition of the urban centers was obtained from the last census of the Brazilian Institute of Geography and Statistics (IBGE).
All courses had identical methodology and format, according to the ACLS (American Heart Association - AHA) instructor’s manual and they were administered by the same team of instructors, all accredited by AHA, after instructor’s
Original Article
Miotto et al Factors that influence learning of emergency
Arq Bras Cardiol 2008; 90(3) : 172-175 Ethics
This study was approved by the Institutional Review Board of the Federal University of Minas Gerais.
Statistical analysis
The theoretical score and the approval in the evaluations theoretical-practical were compared in retrospect at the groups venue A and venue B and groups 1, 2 and 3, according to available data in database.
Initially, the data were analyzed through techniques of descriptive statistics, in which continuous variables were transformed in binary variables, for greater analysis clarity; then these data were contained synthetically in table. Later, the continuous variables were analyzed by the Test of T of Student, ANOVA, and, when necessary, by the non-parametric test of Kruskall-Wallis. As criteria of statistical significance P was used <0.05 for all the variables.
Results
In the period of December 2005 to December 2006, 819 students were trained in emergency by the ACLS course. From this total, 437 were male (53.4%) and 382 female (46.6%). According to the subsidy, the students were distributed like this: group 1 - 199 students (24.3%), group 2 - 122 (14.9%) and group 3 - 498 (60.8%). In group 1 there was small male predominance (60.3%), fact not observed in other groups, and without statistical significance.
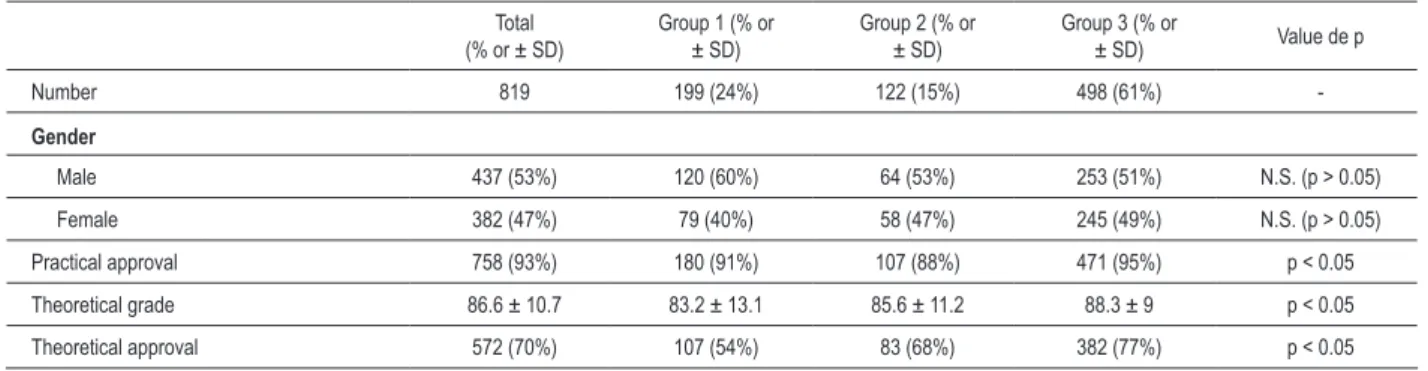
The group 3 presented greater approval in the practical evaluation, followed by 1 and finally by 2 (p <0.05). The theoretical approval was also greater in group 3 than in other groups, and the group 1 presented the lesser approval index. The average of the score in the theoretical evaluation was greater in group 3 than in other groups and group 2 presented better score than group 1 (p <0.05) (tab. 2).
In agreement with the venue of the course, the total of enrolled students, 482 (59%) finished the course in venue A (urban center with more than a million inhabitants) and 337 (41%) in venue B (smaller urban center (tab.3).
The approval in the practical evaluation was similar for venues A and B (p = 0.33), however the theoretical approval was greater in venue A than in B (73% vs. 65% - p = 0.021 - OR = 1.44 and IC: 1.05 - 1.97). The average in the theoretical evaluation was of 87.1 ± 10.4 for venue A and 86 ± 11 for venue B, resulting in significant statistical difference (p <0.05).
Discussion
The participants’ performance was influenced by several factors related to the course, as student, instructor and the course itself7,9,10. The motivated student presented better theoretical and practical performance, however the financial subsidy, many times associated to the compulsory nature of the accomplishment of the ACLS course, could be interpreted as negative factor for the learning (lesser motivation). The data presented demonstrated that the subsidized students (100% or 50%) presented worse performance than those that did not have any subsidy, what resulted in lesser approval and lesser course, and with two-yearly re-certification1. The students
received the material (“ACLS - Manual for providers of health”) with thirty days of antecedence and they were previously instructed by letter to study the manual.
All the mannequins used in the courses complied to the recommendations of AHA and they allowed defibrillation, invasive procedures as intubation and simulation of heart rhythms (Ambu®). The scenario and simulations in the practical classes and in the evaluations followed examples of scenario in the student’s and instrutor’s manual1.
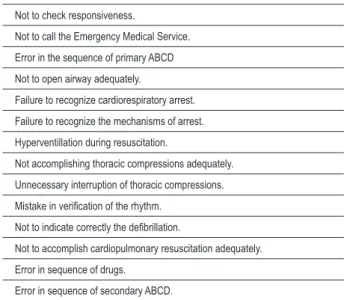
For the certification, all students were submitted to the theoretical and practical evaluation at the end of the course, in agreement with model proposed by the instructor’s of ACLS1 manual. The theoretical test consisted of multiple choice questionnaire with thirty three subjects, elaborated for the courses of ACLS by AHA, and who obtained 84% or more of correct answers was approved. The practical exam evaluated the correct assistance to the cardiac arrest, per AHA algorithm, and the student that accomplished an assistance to a cardiac arrest according to the AHA algorithms and did not make any serious mistake , such as lack of recognition of the rhythm, no call for Emergency Medical Services (EMS) and incorrect indication of defibrillation (tab. 1). was approved.The student that committed some serious mistakes was given a second chance and was evaluated again in another cardiac arrest scenario. If again some serious mistake was made, then the student was reproved.
We compared the approval in the theoretical and practical evaluations and the average in the theoretical evaluation in venue A and B and in the groups with financial subsidy 1, 2 and 3.
All the data were extracted of the database of the training center in emergencies of the Minas Society of Intensive Therapy, which is accredited by AHA.
Table 1 - Serious mistakes in the practical evaluation Not to check responsiveness.
Not to call the Emergency Medical Service. Error in the sequence of primary ABCD Not to open airway adequately.
Failure to recognize cardiorespiratory arrest. Failure to recognize the mechanisms of arrest. Hyperventillation during resuscitation.
Not accomplishing thoracic compressions adequately. Unnecessary interruption of thoracic compressions. Mistake in veriication of the rhythm.
Not to indicate correctly the deibrillation.
Not to accomplish cardiopulmonary resuscitation adequately. Error in sequence of drugs.
Error in sequence of secondary ABCD.
Original Article
Miotto et al
Factors that influence learning of emergency
Arq Bras Cardiol 2008; 90(3) : 172-175
medium score in the theoretical evaluation. Such data suggest that the spontaneous search is derived of greater interest and motivation for the learning of emergency and, consequently, better performance in the theoretical and practical evaluations. As for the work place and the student’s residence, when the course took place in smaller city, with less than a million inhabitants (place B), the performance in the theoretical evaluation was worse, characterizing possibly lesser theoretical knowledge or lesser commitment for the accomplishment of the course. It can also mean lesser previous study of the theoretical material or lesser experience in attendance of emergencies. The fact of, in the practical evaluation, not to have had significant difference can characterize learning capacity of the students or appropriate didactic methodology of the course (factor related to this), but it can also be related to the instructor.
There are other factors involved in the benefit of the training, but the venue of course and the financial subsidy, what depends on the student, have participation in the approval and probably in the retention of the theoretical and practical knowledge.
Conclusion
The influence of financial subsidy and venue of ACLS course in theoretical and practical approval and in average of theoretical evaluation was well recognized. Therefore, strategies should be developed to solve or to ease the problem.
Potential Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Sources of Funding
There were no external funding sources for this study.
Study Association
This article is part of the thesis of master submitted by Heberth C. Miotto, Eugênio M. Goulart e Carlos F. S. Amaral, from Universidade Federal de Minas Gerais.
Table 2 - Characteristics of the groups with and without subsidy and results Total
(% or ± SD) Group 1 (% or ± SD)
Group 2 (% or
± SD)
Group 3 (% or
± SD) Value de p
Number 819 199 (24%) 122 (15%) 498 (61%)
-Gender
Male 437 (53%) 120 (60%) 64 (53%) 253 (51%) N.S. (p > 0.05)
Female 382 (47%) 79 (40%) 58 (47%) 245 (49%) N.S. (p > 0.05)
Practical approval 758 (93%) 180 (91%) 107 (88%) 471 (95%) p < 0.05
Theoretical grade 86.6 ± 10.7 83.2 ± 13.1 85.6 ± 11.2 88.3 ± 9 p < 0.05
Theoretical approval 572 (70%) 107 (54%) 83 (68%) 382 (77%) p < 0.05
Financial subsidy: group 1 - 100% subsídy; group 2 - 50% subsidy; group 3 - without subsidy; ± SD - standard deviation.
Table 3 - Characteristics of the students’ group, according to venue of the course and results of the evaluation
Total (% or ± DP) Venue A (% or ± DP) Venue B (% or ± DP) Value of p
Number 819 482 (59%) 337 (41%)
-Gender
Male 437 (53%) 259 (54%) 178 (53%) p > 0.05
Female 382 (47%) 223 (46%) 159 (47%) p > 0.05
Practical approval 758 (93%) 442 (92%) 316 (94%) p > 0.05
Theorical grade 86.6 ± 10.7 87.1 ± 10.4 86 ± 11 p < 0.05
Theorical approval 572 (70%) 352 (73%) 220 (65%) P < 0.05
Venue of course: venue A - urban centers with more than one million inhabitants; venue B - urban centers with less than one million inhabitants. ± SD - standard deviation
Original Article
Miotto et al Factors that influence learning of emergency
Arq Bras Cardiol 2008; 90(3) : 172-175
References
1. American Heart Association. Advanced cardiac life support: instructor manual. New York: American Heart Association; 2002.
2. Nadel FM, Lavelle JM, Fein JA, Giardino AP, Decker JM, Durbin DR. Teaching resuscitation to pediatric residents: the effects of an intervention. Pediatrics. 2000; 154 (10): 1049-54.
3. Holmberg M, Holmberg S, Herlitz J. Effect of bystander cardiopulmonary resuscitation in out-of-hospital cardiac arrest patients in Sweden. Resuscitation. 2000; 47:59-70.
4. Woollard M, Whitfeild R, Smith A, Colquhoun M, Newcombe RG, Vetter N, et al. Skill acquisition and retention in automated external defibrillator (AED) use and CPR by lay responders: a prospective study. Resuscitation. 2004; 60: 17-28.
5. Seraj MA, Naguib M. Cardiopulmonary resuscitation skills of medical professionals. Resuscitation. 1990; 20: 31-9.
6. Quiney NF, Gardner J, Brampton W. Resuscitation skills amongst anaesthetists. Resuscitation. 1995; 29: 215-8.
7. Stross JK. Maintaining competency in advanced cardiac life support skills. JAMA. 1983; 249: 3339-41.
8. Semeraro F, Signore L, Cerchiari EL. Retention of CPR performance in anaesthetists. Resuscitation. 2006; 68: 101-8.
9. Bullock I. Skills acquisition in resuscitation. Resuscitation. 2000; 45: 139-43.
10. Moser DK, Coleman S. Recommendations for improving cardiopulmonary resuscitation skills retention. Heart Lung. 1992; 21: 372-80.