FREE THEMES
Trends and multiple causes of death due to chronic renal failure
in a municipality in the Brazilian Amazon
Abstract This study examined the mortality trend due to chronic renal failure (CRF) and ver-ified the underlying and associated causes for this trend in the capital of the state of Acre in the Bra-zilian Amazon. This ecological study used data provided by DATASUS related to mortality due to CRF, which occurred between 1986 and 2012 for male and female residents of the city of Rio Branco, Acre, Brazil. The estimated annual per-centage chance (EAPC) was calculated by using Poisson log-linear regression and utilizing the Joinpoint program. The results showed that the adjusted mortality rates due to CRF, with correc-tion, ranged from 15.4 per 100,000 inhabitants in 1986 to 4.0 per 100,000 inhabitants in 2012. The EAPC was -3.5% from 1986- 2012. Deaths by CRF presented associated causes such as respira-tory diseases, pneumonia and pulmonary edema, septicemias and poorly defined signs and symp-toms. When CRF was analyzed as an associated cause of death, the main primary causes of death were hypertensive diseases and diabetes. Thus, there was a decrease in mortality due to CRF as an underlying cause during the period studied; however, preventive and heath care measures should be maintained.
Key words Chronic renal failure, Mortality,
Cause of death Thatiana Lameira Maciel Amaral 1
Cledir de Araújo Amaral 2
Adalberto Luiz Miranda Filho 3
Gina Torres Rego Monteiro 4
1 Centro de Ciências da
Saúde e do Desporto, Universidade Federal do Acre. Rodovia BR 364 Km 04, Distrito Industrial. 69920-900 Rio Branco AC Brasil. thatianalameira27@ gmail.com
2 Instituto Federal do Acre.
Rio Branco Acre.
3 Section of Cancer
Surveillance, International Agency for Research on Cancer. Lyon France.
4 Escola Nacional de Saúde
A
mar
al TLM
Introduction
The Brazilian population has been experiencing an epidemiological transition in which mortality due to infectious diseases has declined in the last decade, whereas deaths due to chronic non-com-municable diseases have increased; the latter were responsible for 73.9% of deaths in 20101.
Chang-es in morbidity profilChang-es, which are mainly due to unfavorable changes in the diet and level of phys-ical activity of the Brazilian population, have im-portant consequences in the pattern of mortality. These changes have been characterized by an in-crease in the deaths of adults and the elderly due to non-infectious diseases2. Hypertension and
di-abetes mellitus associated with obesity3 are some
of the main chronic diseases that have increased in Brazil and they are considered to be the princi-pal causes of chronic renal failure (CRF)4-6.
Renal failure is a serious public health prob-lem with high incidence and prevalence; it results in high costs and a high mortality rate, and it can be either acute or chronic7.CRF is defined by the
presence of renal damage for a period equal to or greater than three months. It is characterized by structural or functional abnormalities of the kidneys, either with or without changes in the glomerular filtration rate, or if the latter is less than 60 mL/min/1.73/m², independently of the presence of renal damage8. The most frequent
complications associated with CRF include in-fections, bleeding and heart failure9-11.
In addition to the evaluation of mortality due to CRF as an underlying cause of death, it is helpful to analyze CRF as an associated cause of death because the process of death due to chronic disease can coexist with several diseases, includ-ing CRF. Thus, analyzinclud-ing mortality in terms of its underlying and associated causes makes it possi-ble to understand the multiple factors that lead to death, i.e. the diagnoses that are consequences of or complications due to the underlying cause of death, such as cardiac, renal, hepatic and other failures, as well as septicemia12. The chronic
dis-eases that are most likely to be reported as asso-ciated causes of death include CRF, unspecified renal failure, diabetes mellitus, asthma, chronic obstructive pulmonary disease, and Alzheimer’s disease. Thus, when an analysis is performed that only considers the underlying causes of death, this precludes the possibility of the provision of a broader spectrum of information about mor-tality13.
Analyzing all the causes of death is a way of generating information about the etiology,
clin-ical evolution and complications of diseases, as well as indirectly influencing the formulation of health actions14,15. Furthermore, knowledge
about the diagnoses mentioned in a death certif-icate provides information that is relevant to the planning of health actions16. The data contained
in the present study is important because it was corrected to take into consideration deaths due to ill-defined and unknown causes. The objective of this study was to evaluate the mortality trend due to CRF and to verify the causes associated with it in the city of Rio Branco, Acre, Brazil.
Methods
This descriptive, ecological study assessed the mortality trend due to CRF from 1986-2012 and the multiple causes of death from 1996-2012. The study included male and female individuals of all ages who were residents of the municipality of Rio Branco in the state of Acre, which is locat-ed in the Western Amazon region of Brazil.
The data regarding deaths from CRF were collected in a disaggregated form from the Mortality Information System (SIM), which is maintained by the Brazilian Ministry of Health (DATASUS/MS)17. The data regarding deaths
from 1986-1995 were based on the codification of the 9th revision of the International Statisti-cal Classification on Diseases and Related Health Problems, Injuries and Causes of Death (ICD-9)18
. The data regarding deaths from 1996-2012
were based on the 10th revision of the Interna-tional Statistical Classification on Diseases and Related Health Problems (ICD-10)19. Thus, CRF
corresponds to code 585 in ICD-9 and N18 in ICD-10. Population data were also obtained for the period under analysis; these were obtained from the population database of the Brazilian In-stitute of Geography and Statistics (IBGE), with populations classified according to age group20.
The proportion of ill-defined and unknown causes of death, and the under-reporting of deaths in Brazil, remains a key issue, especially in the North of the country. For this reason, in order to guarantee the quality of the data the lat-ter were obtained only from the capital of Acre (Rio Branco) and all the analyses were correct-ed for ill-defincorrect-ed and unknown causes of death and for unspecified insufficiencies. The propor-tional redistribution methodology used by the World Health Organization (WHO) was used as a correction factor in the calculation of mortal-ity rates21,22
e C
ole
tiv
a,
23(11):3821-3828,
2018
whose underlying cause was classified as “ ill-de-fined and unknown “ (Codes 780-799 of ICD-9 and R00-R99 of ICD-10); this criterion was rec-ommended by a previous study12. In addition,
the data regarding deaths were also corrected by the redistribution of all deaths classified as due to unspecified renal failure (codes 586 of ICD-9 and N19 of ICD-10), maintaining the same pro-portion of specified deaths19.
For the analysis of the causes of death, all the deaths in which CRF was mentioned in any line of the death certificate (DC) were studied. Com-plications in relation to the underlying cause (part I) and contributing causes (part II) of death were considered together as associated causes of death23
; this information has been available since
1996, and deaths with code N18 were analyzed. The diagnoses mentioned in the death certificate were grouped in accordance with the chapters of ICD-10 in terms of the frequency of diagnoses and the researchers’ interest in the relevance of the causes. All duplications of diagnosis were eliminated.
The causes of death were analyzed by means of the respective frequencies, determining the underlying and associated causes. The crude mortality rates were obtained by the ratio be-tween the number of deaths due to chronic renal failure and the estimated population for each year of the series, which was represented by 100,000 inhabitants. These rates were subsequently stan-dardized by age using the direct method and the world population was used as the standard24,25.
The mortality trend was then analyzed using regression models, utilizing the age-standardized global rate and the age-specific and sex-specific rates of CRF deaths. For the modeling, standard-ized mortality rates (y) were considered as a de-pendent variable, and the studied period of years (x) were considered as an independent variable. Poisson log-linear regression was performed, presenting the Estimated Annual Percentage Chance (EAPC), in which points are identified in which the trend is modified. The chosen model was the one with the highest number of points that maintained statistical significance (p <0.05). Trend analysis was also obtained by age and sex. The statistical analyses were performed using the Joinpoint program, version 3.4 (Statistical Re-search and Applications Branch, National Cancer Institute, USA).
Results
Form 1986-2012 there were 205 deaths with CRF as the underlying cause in the municipality of Rio Branco, of which two were excluded due to lack of information regarding age. The age-adjusted CRF mortality rates, with CRF as underlying cause of death, ranged from 10.8 per 100,000 inhabitants in 1986 to 2.6 per 100,000 inhabitants in 2012. With corrections made based on ill-defined and unknown causes of death and those due to un-specified renal failure the mortality rates were 15.4 per 100,000 inhabitants in 1986 and 4.0 per 100,000 inhabitants in 2012 (Figure 1).
The analysis of the variation in the adjusted mortality rates, between 1986-2012, showed that there was no change in behavior in that period, demonstrating a consistent decrease over the studied period, with the EAPC of CRF being -3.5 (95% CI -5.6, -1.3). The decreasing trend was maintained, both in terms of the division by age group for adults and the elderly, with an EAPC of -4.6 and -2.0, respectively, as well as by gender, with an EAPC for men of -3.3 and -2.6 for wom-en (Figure 1).
The number of deaths in the period from 1996-2012 whose underlying cause was renal failure was 110; in these cases there was an av-erage of 1.9 mentions of causes per death cer-tificate. However, when CRF was analyzed as an associated cause of death it was present in 319 deaths during the same period. The majority of deaths where CRF was cited as a primary or asso-ciated cause of death occurred in males aged 60 and over (Table 1). It was also observed that mor-tality due to renal failure as the underlying cause of death was higher among women up to the age of 59 years compared to men (21.1% versus 7.0% in the age group less than 39 years and 28.9% ver-sus 20.8% in the 40-59 age group, between wom-en and mwom-en respectively). However, there was a higher mortality rate for men in all age groups over the age of 60 compared to women (48.6% versus 28.9% between the ages of 60-79, and 23.6% versus 21.1% in the age group of 80 and older, between men and women respectively).
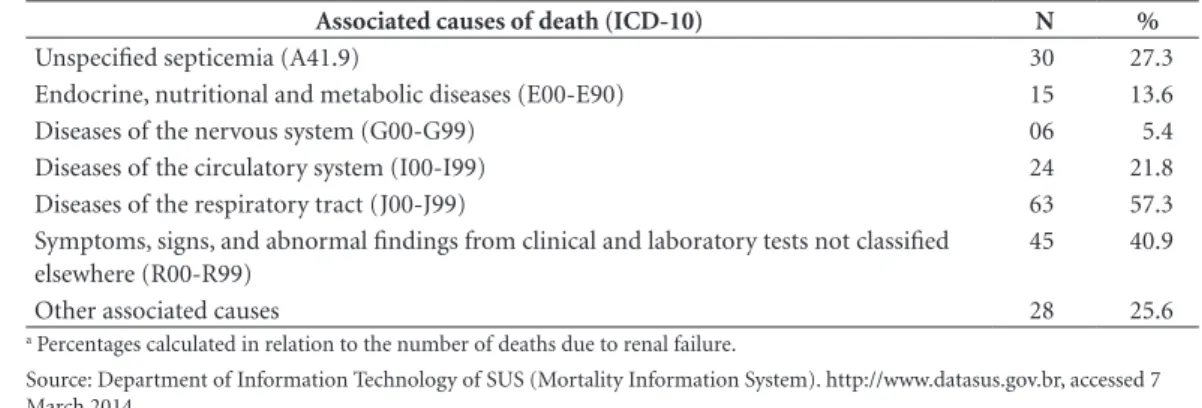
In the analysis of mortality due to CRF as an underlying cause of death, diseases of the respi-ratory tract were the main indications of causes of death, especially pneumonia (39.7%) and pul-monary edema (17.5%), followed by poorly de-fined signs and symptoms, as well as unspecified septicemia (Table 2).
circu-A
mar
al TLM
latory diseases, followed by endocrine, nutrition-al and metabolic diseases, as well as respiratory diseases (Table 3). Of the endocrine, nutritional and metabolic diseases, diabetes mellitus ac-counted for 22.3% of all deaths.
Analyzing the deaths due to diseases of the circulatory system, with CRF as an associated cause, hypertensive diseases were the main cause of death, followed by cerebrovascular diseases (Table 4).
Discussion
This study found that there was a decrease in mortality due to CRF over the analyzed period
and that this decrease was higher among the el-derly and women. It was also found that among the deaths due to CRF the mentions of causes of death were predominantly related to the respi-ratory system. When diseases of the circulatory system were evaluated as an associated cause of death they were the main underlying causes of death.
Comparatively, the mortality rates observed in Rio Branco in 2009 were higher when com-pared to the rates observed in Brazil as a whole. Brazil was ranked eighth in terms of deaths due to CRF in 2009 among the countries of the Amer-icas, with a mortality rate of 3.8 per 100,000 male inhabitants and 4.8 per 100.000 female in-habitants26. The estimated prevalence of CRF in
Figure 1. General trend, by age and gender, of adjusted mortality rates (with correction) of chronic renal failure
as the underlying cause of death per 100,000 inhabitants in Rio Branco, Acre, Brazil, 1986-2012.
Rate Trend
Year
1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
12
10
8
6
4
2
0
M
o
rtalit
y r
at
e p
er 100.000 inhabitants
Year
1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
12
10
8
6
4
2
0
M
o
rtalit
y r
at
e p
er 100.000 inhabitants
Both genders aged 50-59 Both genders >60
1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
20 18 16 14 12 10 8 6 4 2 0
M
o
rtalit
y r
at
e p
er 100.000 inhabitants
Year
1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
25
20
15
10
5
0
M
o
rtalit
y r
at
e p
er 100.000 inhabitants
Female
Year
e C
ole
tiv
a,
23(11):3821-3828,
2018
Table 1. Underlying and associated causes of death due to chronic renal failure according to gender and age in
Rio Branco, Acre, Brazil, 1996-2012.
Variable Underlying cause Associated cause
N % N %
Gender
Male 72 65.5 214 67.1
Female 38 34.5 105 32.9
Married status a
Single 40 41.2 91 34.5
Married 33 34.0 110 41.7
Widow(er) 19 19.6 45 17.0
Legally separated 05 5.2 18 6.8
Age (years)
< 39 13 11.9 34 10.6
40 - 59 26 23.6 81 25.4
60 - 79 46 41.8 153 48.0
80 and above 25 22.7 51 16.0
Total 110 100.0 319 100.0
a underlying cause N = 97; associated cause N = 264.
Source: Department of Information Technology of SUS (Mortality Information System). http://www.datasus.gov.br, accessed 7 March 2014.
Table 2. Mention of causes referred to as an underlying cause of death in deaths due to chronic renal failure (N
= 110)a in Rio Branco, Acre, Brazil, 1996-2012.
Associated causes of death (ICD-10) N %
Unspecified septicemia (A41.9) 30 27.3
Endocrine, nutritional and metabolic diseases (E00-E90) 15 13.6
Diseases of the nervous system (G00-G99) 06 5.4
Diseases of the circulatory system (I00-I99) 24 21.8
Diseases of the respiratory tract (J00-J99) 63 57.3
Symptoms, signs, and abnormal findings from clinical and laboratory tests not classified elsewhere (R00-R99)
45 40.9
Other associated causes 28 25.6
a Percentages calculated in relation to the number of deaths due to renal failure.
Source: Department of Information Technology of SUS (Mortality Information System). http://www.datasus.gov.br, accessed 7 March 2014.
Table 3. Underlying causes of death when chronic renal failure was referred to as an associated cause in the
death certificate in Rio Branco, Acre, Brazil, 1996-2012.
Underlying causes of death (ICD-10) N %
Infectious and parasitic diseases (A00-B99) 20 6.3
Neoplasms (C00-D48) 32 10
Endocrine, nutritional and metabolic diseases (E00-E90) 88 27.6
Diseases of the circulatory system (I00-I99) 113 35.4
Diseases of the respiratory system (J00-J99) 29 9.1
Diseases of the digestive system (K00-K93) 15 4.7
Diseases of the genitourinary system (N00-N99) a 10 3.1
Other underlying causes 12 3.8
Total 319 100.0
a Excluding diagnosis N18 (ICD-10).
A
mar
al TLM
Brazil is approximately 503 patients per million inhabitants and the mortality rate tended to fall in 201227.
This study found that there was a decreasing trend in CRF mortality rates in the city of Rio Branco. There is a worldwide variation in the mortality behavior of this disease. For example, in the city of Michigan in the USA the mortality rate due to CRF increased from 14.8 per 100,000 inhabitants in 1999 to 15.4 per 100,000 inhabi-tants in 2005; it was highest among elderly peo-ple, reaching 173.6 per 100.000 inhabitants for those aged over 7528. In the present study, the
highest mortality rates were also found among the elderly.
In a cohort study conducted in the USA (NHANES II) over 16 years of follow-up, it was observed that individuals with CRF had a high-er risk of death from all causes of death, with a predominance of cardiovascular diseases29. In a
study carried out in the Brazilian state of Paraná other causes of death included septicemia, neo-plasias and malnutrition30.
A Brazilian study, which included nationwide data from patients who started renal replacement therapy in 2002 and 2003, and was followed up until 2004, revealed that 42% of patients on peri-toneal dialysis and 33% of those on hemodialy-sis died; these deaths were particularly related to diabetes mellitus and cardiovascular diseases31. A
further study of mortality due to CRF, which was performed from 2000-2004, found that diabetes and cardiovascular diseases were the main un-derlying causes of death due to CRF; in the anal-ysis of associated causes of death it was found that 48% of deaths resulted from complications related to treatment, especially infections32.
In the present study, the main causes of death due to CRF listed in death certificates were dis-eases of the respiratory tract, followed by poor-ly defined signs and symptoms, and septicemia.
The predisposition of patients with CRF to in-fections is associated with age, comorbidities, hypoalbuminemia, immunosuppressive ther-apy, nephrotic syndrome, uremia, anemia and malnutrition. Many of these conditions may be present even before the start of dialysis. Added to these factors are vascular access and the dialysis procedure itself33.
The main underlying causes of death with CRF as an associated cause were circulatory, en-docrine, nutritional and metabolic diseases, with an emphasis on hypertensive diseases and dia-betes, which corroborates the findings of other studies34-39. In data from 2011, which related to
mortality in Australia, CRF accounted for 10% of the multiple causes of death, 39% of which were associated with cardiovascular diseases40.
CRF promotes the progression of cardiovas-cular disease through volume expansion, disor-ders of the calcium-phosphate metabolism, dys-lipidemia, and hypertension. On the other hand, cardiovascular disease can promote the decline of renal function due to heart failure and ath-erosclerosis41. In this context, studies on multiple
causes of mortality foreground the understand-ing of CRF, with a view to preventunderstand-ing factors re-lated to death13. It should be mentioned that the
data presented in the present study refers to indi-viduals with CRF who were, therefore, at a higher risk of death.
The limitations of the present study were the use of a secondary database, which is subject to inaccuracies. To minimize this issue, the rates were calculated to take into account correction for ill-defined and unknown causes of death and for unspecified renal failure. Another possible limitation of this study was the quality of the information that was used, because this depends on the complete and correct completion of death certificates42. However, the positive aspects of
this study are that it includes an analysis of the
Table 4. Deaths related to renal failure as an associated cause according to the underlying cause of death due to
diseases of the circulatory system in Rio Branco, Acre, Brazil, 1996-2012.
Diseases of the circulatory system (I00-I99) N %
Hypertensive diseases (I10-I15) 66 58.4
Ischemic heart diseases (I20-I25) 10 8.9
Other forms of heart disease (I30-I52) 17 15.0
Cerebrovascular diseases (I60-I69) 18 15.9
Other diseases of the circulatory system 02 1.8
Total 113 100.0
e C
ole
tiv
a,
23(11):3821-3828,
2018
causes of death due to CRF (as an underlying and associated cause), and the possibility of suggest-ing designs for actions to minimize related com-plications that result in death in the city of Rio Branco. This contributes to the accumulation of knowledge that supports the adoption of more comprehensive measures that are appropriate to local conditions.
The focus on underlying causes of death, as well as associated causes of death, makes it pos-sible to identify the diseases that participate in the morbid process of death due to CRF. Con-sequently, understanding the temporal evolu-tion and the causes involved in the death process makes it possible to assess the public health prob-lem constituted by chronic renal failure.
It was concluded that there was a reduction in mortality due to CRF in Rio Branco in the stud-ied period, with the greatest decrease found to be
among those aged over 50 and among women. The deaths caused by the CRF presented respi-ratory diseases, including pneumonia and pul-monary edema, as well as abnormal findings and septicemia as causes of death. When CRF was analyzed as an associated cause of death the most frequent main causes of death were hypertensive diseases and diabetes.
Collaborations
TLM Amaral, CA Amaral and AL Miranda Filho contributed to the design of the research project, collecting, processing, analyzing, interpreting data and writing the manuscript; GTR Monteiro, participated in the analysis and interpretation of the data, critical review and approval of the final version of the manuscript.
References
1. Duarte EC, Barreto SM. Transição demográfica e epi-demiológica: a Epidemiologia e Serviços de Saúde revi-sita e atualiza o tema. Epidemiol Serv Saúde [Internet]; 2012 [cited 2016 Out 23]; 21(4):529-532. Available from: http://scielo.iec.pa.gov.br/scielo.php?script=s-ci_arttext&pid=S167949742012000400001&lng=pt. http://dx.doi.org/10.5123/S1679-49742012000400001 2. Schmidt MI, Duncan BB, Silva GA, Menezes AM,
Mon-teiro CA, Barreto SM, Chor D, Menezes PR. Chronic non-communicable diseases in Brazil: burden and cur-rent challenges. Lancet 2011; 377(9781):1949-1961. 3. Schmidt MI, Duncan BB, Hoffmann JF, Moura L, Malta
DC, Carvalho RMSV. Prevalência de diabetes e hiper-tensão no Brasil baseada em inquérito de morbidade auto-referida, Brasil, 2006. Rev Saude Publica 2009; 43(Supl. 2):74-82.
4. Balbi AL, Gabriel DP, Barsante RC, Caramori JT, Mar-tin LC, Barreti P. Mortalidade e prognóstico específico em pacientes com insuficiência renal aguda. Rev Assoc Medica Bras 2005; 51(6):318-322.
5. Bortolotto LA. Hipertensão arterial e insuficiência re-nal crônica. Rev Bras Hipertens 2008; 15(3):152-155. 6. Tsioufis C, Tatsis I, Thomopoulos C, Wilcox C, Palm
F, Kordalis A, Katsiki N, Papademetriou V, Stefanadis C. Effects of hypertension, diabetes mellitus, obesity and other factors on kidney haemodynamics. Curr Vasc Pharmacol 2014; 12(3):537-548.
7. Levey AS, Eckardt KU, Tsukamoto Y, Levin A, Coresh J, Rossert J, De Zeeuw D, Hostetter TH, Lameire N, Ek-noyan G. Definition and classification of chronic kid-ney disease: a position statement from Kidkid-ney Disease: Improving Global Outcomes (KDIGO). Kidney Int 2005; 67(6):2089-2100.
8. National Kidney Foundation. K/DOQI clinical prac-tice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis 2002; 39(2 Supl. 1):S1-266.
9. Costa JAC, Vieira-Neto OM, Moysés Neto M. Insufici-ência renal aguda. Medicina 2003; 36(2/4):307-324. 10. Naqvi SB, Collins AJ. Infectious complications in
chronic kidney disease. Adv Chronic Kidney Dis 2006; 13(3):199-204.
11. Thomas R, Kanso A, Sedor JR. Chronic kidney disease and its complications. Prim Care 2008; 35(2):329-vii. 12. Jorge MHPM, Gotlieb SLD, Laurenti R. The national
mortality information system: problems and proposals for solving them I - Deaths by natural causes. Rev Bras Epidemiol 2002; 5(2):197-211.
13. Australian Institute of Health and Welfare (AIHW). Multiple causes of death in Australia: an analysis of all natural and selected chronic disease causes of death 1997-2007 [Internet]. Canberra: AIHW; 2012 [cited 2014 May 16]. (AIHW bulletin no. 105. Cat. no. AUS 159). Available from: http://www.aihw.gov.au/WorkArea/ DownloadAsset.aspx?id=10737422598
14. Israel RA, Rosenberg HM, Curtin LR. Analytical poten-tial for multiple cause-of-death data. Am J Epidemiol 1986; 124(2):161-179.
15. Redelings MD, Sorvillo F, Simon P. A comparison of underlying cause and multiple causes of death: US vital statistics, 2000-2001. Epidemiology 2006; 17(1):100-103.
A
mar
al TLM
17. Brasil. Ministério da Saúde (MS). Sistema de Informa-ção de mortalidade/DATASUS [Internet]. 2012 [cited 2014 Aug 16]. Available from: http://www2.datasus. gov.br/DATASUS/index.php?area=0205
18. Organização Mundial da Saúde (OMS). Classificação estatística internacional de doenças: manual de lesões e causas de óbito - CID-9. 9ª ed. São Paulo: Centro Brasi-leiro Classificação Doenças em Português; 1979. (Ma-nual de instrução).
19. Organização Mundial da Saúde (OMS). Classificação estatística internacional de doenças e problemas relacio-nados à saúde - CID -10 [Internet]. 10ª ed. São Paulo: Centro Colaborador da OMS para a Classificação de Doenças em Português/Edusp; 1993. (Manual de ins-trução; vol. 2). Available from: http://www.datasus.gov. br/cid10/V2008/cid10.htm
20. Instituto Brasileiro de Geografia e Estatística (IBGE). Sistema IBGE de Recuperação Automática - SIDRA [In-ternet]. 2013 [cited 2014 May 4]. Available from: http:// www.sidra.ibge.gov.br/cd/cd2010RgaAdAgsn.asp 21. França E, Teixeira R, Ishitani L, Duncan BB,
Cortez-Es-calante JJ, Morais OL, Szwarcwald CL. Ill-defined caus-es of death in Brazil: a redistribution method based on the investigation of such causes. Rev Saude Publica 2014; 48(4):671-681.
22. Mathers CD, Bernard C, Iburg KM, Inoue M, Fat DM, Shibuya K, Stein C, Tomijima N, Xu H. Global burden of disease in 2002: data sources, methods and results. Ge-neva: World Health Organization; 2003.
23. Santo AH. Causas múltiplas de morte: formas de apre-sentação e métodos de análise [Tese]. São Paulo: Univer-sidade de São Paulo, Faculdade de Saúde Pública; 1988. 24. Doll R, Payne P, Waterhouse JAH. Cancer incidence in
five continents. Geneva: Union Internationale Contre le Cancer; 1966. Vol. I
25. Segi M. Cancer mortality for selected sites in 24 countries (1950-57). Sendai: Department of Public Health, To-hoku University of Medicine Japan; 1960.
26. Pan American Health Organization (PAHO). Visual-izing renal failure and chronic kidney diseases age-stan-dardized mortality rate in countries of the Americas, 2000-2009 [Internet]. Washington: PAHO; 2014. [cit-ed 2015 May 16]. (Non-communicable Diseases and Mental Health). Available from: http://www.paho. org/hq/index.php?option=com_content&view=arti- cle&id=9381:renal-failure-chronic-kidney-disease-ck-d&Itemid=41166&lang=en
27. Sesso RC, Lopes AA, Thome FS, Lugon JR, Watanabe Y, Santos DR. Report of the Brazilian Chronic Dialysis Census 2012. J Bras Nefrol 2014; 36(1):48-53. 28. Centers for Disease Control and Prevention. Kidney
disease mortality - Michigan, 1989-2005. MMWR Morb Mortal Wkly Rep 2007; 56(10):225-227. 29. Muntner P, He J, Hamm L, Loria C, Whelton PK.
Re-nal insufficiency and subsequent death resulting from cardiovascular disease in the United States. J Am Soc Nephrol 2002; 13(3):745-753.
30. Peres LA, Biela R, Herrmann M, Matsuo T, Ann HK, Camargo MT, Rohde NR, Uscocovich VS. Epidemi-ological study of end-stage kidney disease in western Paraná: an experience of 878 cases in 25 years. J Bras Nefrol 2010; 32(1):51-56.
31. Szuster DAC, Caiaffa WT, Andrade EIG, Acurcio FA, Cherchiglia ML. Survival analysis of dialysis patients in the Brazilian Unified National Health System. Cad Saude Publica 2012; 28(3):415-424.
32. Siviero PCL, Machado CJ, Cherchiglia ML. Chronic kidney failure by means of multiple causes of death in Brazil. Cad Saude Colet 2014; 22(1):75-85.
33. Dalrymple LS, Go AS. Epidemiology of acute infec-tions among patients with chronic kidney disease. Clin J Am Soc Nephrol 2008; 3(5):1487-1493.
34. Global Burden of Metabolic Risk Factors for Chronic Diseases Collaboration. Cardiovascular disease, chron-ic kidney disease, and diabetes mortality burden of car-diometabolic risk factors from 1980 to 2010: a compar-ative risk assessment. Lancet Diabetes Endocrinol 2014; 2(8):634-647.
35. Perazella MA, Khan S. Increased mortality in chron-ic kidney disease: a call to action. Am J Med Sci 2006; 331(3):150-153.
36. Tonelli M, Wiebe N, Culleton B, House A, Rabbat C, Fok M, McAlister F, Garg AX. Chronic kidney dis-ease and mortality risk: a systematic review. J Am Soc Nephrol 2006; 17(7):2034-2047.
37. Chronic Kidney Disease Prognosis Consortium, Mat-sushita K, van der Velde M, Astor BC, Woodward M, Levey AS, de Jong PE, Coresh J, Gansevoort RT. Associ-ation of estimated glomerular filtrAssoci-ation rate and albu-minuria with all-cause and cardiovascular mortality in general population cohorts: a collaborative meta-anal-ysis. Lancet 2010; 375(9731):2073-2081.
38. Rao MV, Qiu Y, Wang C, Bakris G. Hypertension and CKD: Kidney Early Evaluation Program (KEEP) and National Health and Nutrition Examination Survey (NHANES), 1999-2004. Am J Kidney Dis 2008; 51(4 Supl. 2):S30-S37.
39. Rashidi A, Sehgal AR, Rahman M, O’Connor AS. The case for chronic kidney disease, diabetes mellitus, and myocardial infarction being equivalent risk factors for cardiovascular mortality in patients older than 65 years. Am J Cardiol 2008; 102(12):1668-1673. 40. Australian Institute of Health and Welfare (AIHW).
Cardiovascular disease, diabetes and chronic kidney disease: Australian facts: mortality [Internet]. Canber-ra: AIHW; 2014 [cited 2014 Oct 11]. (Cardiovascular, diabetes and chronic kidney disease series no. 1. Cat. no. CDK 1). Available from: http://www.aihw.gov.au/ WorkArea/DownloadAsset.aspx?id=60129549107 41. Weiner DE, Sarnak MJ. Chronic kidney disease and
cardiovascular disease: A bi-directional relationship? Dial Transplant 2007; 36(3):113-120.
42. Conselho Federal de Medicina. Resolução CFM n° 1.779, de 11 de novembro de 2005. Regulamenta a res-ponsabilidade médica no fornecimento da Declaração de Óbito. Diário Oficialda União 2005; 5 dez.
Article submitted 23/08/2016 Approved 08/11/2016
Final version submitted 10/11/2016
This is an Open Access article distributed under the terms of the Creative Commons Attribution License BY