www.jped.com.br
ORIGINAL
ARTICLE
Characterization
of
mortality
in
children
with
sickle
cell
disease
diagnosed
through
the
Newborn
Screening
Program
夽
,
夽夽
Alessandra
P.
Sabarense
a,
Gabriella
O.
Lima
a,
Lívia
M.L.
Silva
a,
Marcos
Borato
Viana
b,∗aFaculdadedeMedicina,UniversidadeFederaldeMinasGerais(UFMG),BeloHorizonte,MG,Brazil
bDepartmentofPediatrics,FaculdadedeMedicina,UniversidadeFederaldeMinasGerais(UFMG),BeloHorizonte,MG,Brazil
Received14April2014;accepted6August2014 Availableonline6November2014
KEYWORDS Sicklecellanemia; Deathrate; Infection; Acutesplenic sequestration; Neonatalscreening
Abstract
Objective: Tocharacterizethedeathsof193childrenwithsicklecelldiseasescreenedbya
neonatalprogramfrom1998to2012andcontrasttheinitialyearswiththefinalyears.
Methods: Deathswereidentifiedbyactivesurveillanceofchildrenabsenttoscheduled
appoint-mentsinBloodBankClinicalCenters(Hemominas).Clinicalandepidemiologicaldatacamefrom
deathcertificates,neonatalscreeningdatabase,medicalrecords,andfamilyinterviews.
Results: Between1998and2012,3,617,919childrenwerescreenedand2,591hadsicklecell
disease (1:1,400). Therewere 193 deaths(7.4%): 153with SS/S0-talassemia, 34 SCand6
S+thalassemia; 76.7% were younger thanfive years; 78% died in the hospital and 21% at
homeorintransit.Themaincausesofdeathwereinfection(45%),indeterminate(28%),and
acutesplenicsequestration(14%).In46%ofdeathcertificates,theterm‘‘sicklecell’’wasnot
recorded.Seven-yeardeathrateforchildrenbornbetween1998and2005was5.43%versus
5.12%forthosebornbetween2005and2012(p=0.72).Medicalcarewasprovidedto75%of
children;24%wereunassisted.Medicalcarewasprovidedwithin6hoursofsymptomonsetin
onlyhalfoftheinterviewedcases.In40.5%ofcases,deathoccurredwithinthefirst24hours.
Lowfamilyincomewasrecordedin90%ofcases,andilliteracyin5%.
Conclusions: Althoughcomprehensiveandeffective,neonatalscreeningforsicklecelldisease
wasnotsufficienttosignificantlyreducemortalityinanewbornscreeningprogram.Economic
andsocial developmentandincrease oftheknowledgeon sicklecelldisease among health
professionalsandfamilyareneededtoovercomeexcessivemortality.
©2014SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:SabarenseAP,LimaGO,SilvaLM,VianaMB.Characterizationofmortalityinchildrenwithsicklecelldisease
diagnosedthroughtheNewbornScreeningProgram.JPediatr(RioJ).2015;91:242---7.
夽夽StudyconductedatNúcleodeAc¸õesePesquisaemApoioDiagnóstico(Nupad),FaculdadedeMedicina,UniversidadeFederaldeMinas
Gerais(UFMG),BeloHorizonte,MG,Brazil.
∗Correspondingauthor.
E-mail:vianamb@gmail.com(M.B.Viana). http://dx.doi.org/10.1016/j.jped.2014.08.006
PALAVRAS-CHAVE Anemiafalciforme; Mortalidade; Infecc¸ão;
Sequestroesplênico agudo;
Triagemneonatal
Caracterizac¸ãodoóbitodecrianc¸ascomdoenc¸afalciformediagnosticadaspor ProgramadeTriagemNeonatal
Resumo
Objetivo: Caracterizar os 193óbitosde crianc¸as comdoenc¸afalciforme diagnosticadas por
programadetriagemneonatalentre1998-2012ecompararosprimeiroscomosúltimosanos.
Métodos: Osóbitosforamidentificadospelabuscaativadascrianc¸asausentesnasconsultas
agendadasnoshemocentros.Dadosclínicos eepidemiológicos provieramdosdocumentosde
óbito,bancodedadosdatriagemneonatal,prontuáriosmédicoseentrevistascomfamiliares.
Resultados: Entre1998-2012foramtriadas3.617.919crianc¸as,2.591comdoenc¸afalciforme
(1:1.400).Ocorreram193óbitos(7,4%):153comSS/S0-talassemia,34SCe6S+-talassemia;
76,7%emcrianc¸ascommenosde5anos;78%faleceramemhospitaise21%emdomicílioou
trânsito.Causasprincipaisdoóbito:45%infecc¸ão,28%indeterminada,14%sequestroesplênico
agudo.Em46%dosdocumentosdeóbito,nãohouveregistrodotermo‘‘falciforme’’.Ataxade
mortalidadeatéseteanosdascrianc¸asnascidasentre1998-2005foi5,43%versus5,12%,entre
2005-2012(p=0,72).Receberamassistênciamédica75%dascrianc¸as;24%ficaramdesassistidas.
Pelas entrevistas, atendimentomédicoteria ocorrido nasprimeiras seishoras doiníciodos
sintomasemmetadedoscasos.Oóbitoocorreuem40,5%doscasos,nasprimeiras24horas.
Baixarendafamiliarfoiregistradaem90%doscasoseanalfabetismoem5%.
Conclusões: Atriagemparadoenc¸afalciforme,mesmoabrangenteeeficaz,nãofoisuficiente
parareduzirsignificativamenteamortalidadenoProgramadeTriagemNeonatal.Necessita-se
dedesenvolvimentoeconômicoesocialdoestadoeampliac¸ão,pelaeducac¸ãocontinuada,do
conhecimentosobreadoenc¸afalciformeentreosprofissionaisdesaúdeefamiliares.
©2014SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos
reservados.
Introduction
Sicklecelldisease(SCD)comprisesagroupofhematologic disordersofgeneticorigin,whose mainfeatureisthe pre-dominanceofhemoglobinS(HbS)inredbloodcells.SCDhas greatclinicalandepidemiologicalimportance,being consid-eredapublichealthprobleminBrazil.1---3HbSinhomozygous
form (HbSS), called sickle cell anemia (SCA), is the most
commongenotypeandthemostsevereclinicalpresentation
of the disease. The concept of SCD also includes
dou-bleheterozygosityforHbSwithotherhemoglobinvariants
(HbSC,HbSD-Punjab,andothers)andtheinteractionofHbS
withbetathalassemia(HbS/0andHbS/+thalassemias).4,5
The main determinants of the clinical manifestations of
thediseasearethevaso-occlusivephenomenaandchronic
hemolysis.4
Hemoglobinopathiesareresponsible,worldwide,for3.4%
ofdeathsinchildrenunder5years.6PatientswithSCDhave
highratesofmorbidityandmortality,mainlyindeveloping
countries.7Evenindevelopedcountries,althoughmortality
inchildrenhasdecreased,SCDisstillasignificantcauseof
mortalityinadolescentsandadults.8
A prevalence of 25,000-30,000 individuals with SCD is
estimated in Brazil, withan incidence of 3,500 cases per
year.9 In thestate ofMinas Gerais (MG), theincidenceof
SCDis1:1,400screenednewborns,basedondatafromthe
NeonatalScreeningProgram(NSP-MG).10
AstudyconductedinMG10characterizedthedeathof78
childrenwithSCDscreenedbytheNSP-MGintheperiodof
1998-2005andconcludedthatmostdeathsoccurredin
chil-drenunder2yearsandindividualswithHbSS,mainlydueto
infection(septicemiaandpneumonia).Apredominance of
in-hospitaldeathswasobserved;however,theoccurrenceof
athomeorin-transitdeathswasstillsignificant.An
indeter-minatecauseofdeathonthedeathcertificatewasfrequent,
whichwouldindicatealackofknowledgeamongphysicians
regardingSCD and acuteevents thatare determinants of
death.
Thisstudyaimedtocharacterizethedeathsofchildren
withSCDthathadbeen screenedby theNSP-MGbetween
1998and2012.Wheneverpossible,comparativeanalysisof
deathsofchildrenbornbetweenMarchof1998andFebruary
of2005withthosebornbetweenMarchof2005and
Decem-ber of 2012 was performed to describe possible changes
regardingthequalityofcareprovidedtothesechildren.
Methods
Thepopulation investigatedin thisstudy consistedof 117 childrendiagnosedwithSCDattheNSP-MG,followed-upin theBloodBanksofFundac¸ãoHemominas,andwhodiedin theperiodfromMarch1,2005toFebruary29,2012.In sev-eralanalyses, 76 deaths that occurred between March of 1998and February of 2005were addedtothe sample (of the78deathsreported,twochildrenwereexcluded,whose birthwaspriortoMarch1,1998),10totaling193deathsand
thuscomplementingthe14yearsofthestudy.
The NSP-MGperformsscreening forSCDsinceMarchof
1998.All853 state municipalities areregistered. In2010,
91.44%oftheinfantsborninthestateofMinasGeraiswere
Research(NúcleodeAc¸õesePesquisaemApoioDiagnóstico
[NUPAD]), and free medicaltreatment and follow-up was
offeredtothosebornwithSCD.
The informationondeathresultsfroman investigation
conducted by the Control and Treatment Department of
NUPADduetonon-attendanceatscheduledconsultationat
theBloodBank.Theactivesearchesperformedencompass
allscreenedpatientswithSCDfollowed-upattheoutpatient
clinicofFundac¸ãoHemominasthroughoutthestate.
There-fore,itcanbestatedthatalldeathsthatoccurredduring
thestudyperiodwererecorded.
The data for this research came from the NUPAD
database, death certificates, the Brazilian UnifiedHealth
Systemdatabase(DATASUS),theBrazilianInstituteof
Geog-raphy and Statistics (Instituto Brasileiro de Geografia e
Estatística[IBGE]), medicalrecords of Fundac¸ão
Hemom-inas, and from interviews with the children’s family
members.
TheinformationintheNUPADdatabasewasusedto
per-formanactivesearchofthe117familieswhosechildrenhad
diedbetween2005and2012.Theinterviewwasperformed
withthechild’sguardian,usingasemistructuredformused
byFernandesetal.10Atotalof81familieswereinterviewed
bytheresearcher andthreefamilieswereinterviewedby
nursesfromthereferralBasicHealthUnits.
Fivefamiliesrefusedtobeinterviewed,onewasunable
totalk about the subject, and 27 were not located. The
interview coveredfive aspects: (1) death-related
circum-stances;(2)follow-up ofSCDandtheoccurrenceof other
acuteevents;(3)family’ssocioeconomicandcultural
con-ditions, which considered per capita income, education,
parents’occupation,andhousing conditions;(4)
consider-ationsabout their experiencewiththe child;(5) applying
thescaleofknowledgeonSCDtothefamilies,consistingof
20questionswithansweroptions:‘‘right’’,‘‘wrong’’,or‘‘I
don’tknow.’’The interviewwasperformed onlyafterthe
informedconsentformwassigned,whichencompassedthe
objectives,purpose,andbenefitsoftheresearch.
Regarding the causes of death, they were considered
asindeterminatewhenthephysiciansshowedambiguityin
themedicalrecordsofthedeathcertificate,regardlessof
wherethedeathoccurredandwhetherthechildreceived
assistance, thus making it impossible for researchers to
determineitscause.
Forthe statisticalanalysis, comparisonsof frequencies
betweennominalvariablesweremadeusingthechi-squared
testwithoutcontinuitycorrection.Testswithaprobability
ofalphaerror≤ 0.05wereconsideredsignificant.
ThestudywasapprovedbytheEthicsCommitteeof
Uni-versidade Federal de Minas Gerais (UFMG) and Fundac¸ão
Hemominas.
Results
Marchof1998toFebruaryof2012(193deaths)
A total of 3,617,919 children were screened through the NSP-MG. Of these, 2,591 children had a hemoglobin pro-filecompatiblewith SCDand193 of them died (7.4%),of whom97(50.3%)weremales.Regardinggenotypes,153had
SS/S0thalassemia(79.3%),34hadSC-(17.6%),andsixhad S+-thalassemia(3.1%).
Mostchildrenwhodied150(77.7%)livedinurbanareas ofthemunicipalities.Whenthemunicipalitiesinthestate ofMinasGeraisthatrecordeddeathsareconsidered,98of 378children diagnosedwithSCD(25.9%) diedinthesmall municipalities, i.e., towns withup to50,000 inhabitants. Thisisincontrastwiththe93deathsamong1,228children (7.6%)frommediumorlarge-sizedmunicipalities,plusthe large cities (p < 0.000001). Two children died out of the state.
Themedianageatbloodcollectionforscreeningwas6 days; 75% of the children were screened at up to8 days oflife.ThemedianageatthefirstvisittotheBloodBank ClinicalCenterwas1.4months.Twelvechildren(6.2%)died prior tothe first consultation; nine died before reaching 60 days, the maximum period of waiting until the first consultation in Blood Banks, mostly due to prematurity and itscomplications, according to thedeath certificates assessed by the researchers. Three children died at 105, 122,and131daysofage,twoofthemwithsevere congeni-talcardiomyopathy.Theotherchilddiedwithacutesplenic sequestrationinthecityofVitória(ES),withoutundergoing theconsultationat theBloodBankinValadares (MG);two familieswereinterviewedbytheresearchers.
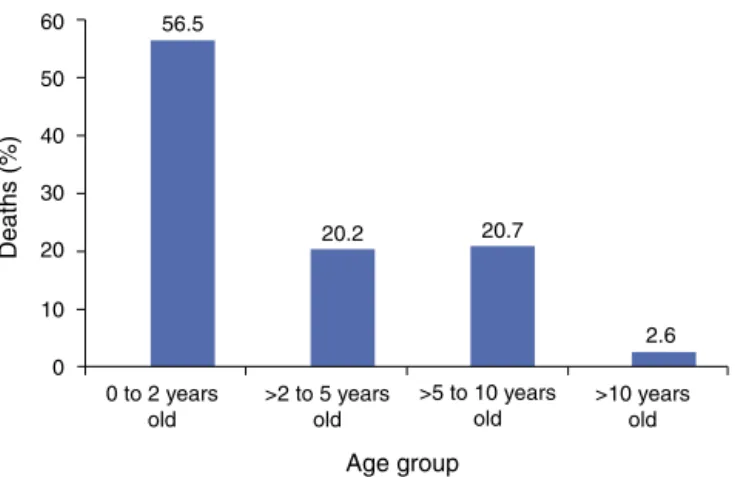
Itwas observed that56.5% of deaths occurred in chil-dren younger than 2 years of age and 76.7% occurred in childrenyoungerthan5years.Themedianageatdeathwas 1.7years.Fig.1showsthedistributionbyagerange.
Accordingtoinformationobtainedfromthe death
cer-tificatesandinterviewswithfamilymembers,therewasa
prevalenceofin-hospitaldeaths(78%),buttheoccurrence
of21home(11%) and19in-transit(10%)deathsshouldbe
emphasized.
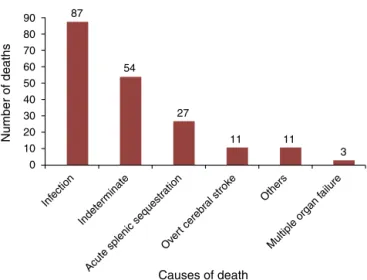
Infection,includingsepticemia,pneumonia/acutechest,
andgastroenteritis,wastheleadingcauseofdeathsinthis
group(45%),followedbyindeterminatecauses(28%).Acute
splenic sequestration (ASS) was the third cause of death
(14%),asshowninFig.2.AmongthechildrenwithSS/S0
-thalassemia,ASSwasthecauseofdeathin17.6%.
Mostchildren(75%)receivedmedicalcarebeforedeath;
however,thenumberofchildrenthatwentunassisted(24%)
56.5
20.2 20.7
2.6
0 to 2 years old 60
50
40
Deaths (%)
30
20
10
0
>2 to 5 years old
>5 to 10 years old
>10 years old
Age group
Figure1 Distribution,byagegroup,ofthedeathsof193
chil-drenwithsicklecelldiseasewhodiedbetweenMarchof1998
90 87
54
27
11 11
3 80
70 60 50 40 30 20
Infection
Indeter minate
Acute splenic sequestr ation
Over t cerebr
al strok e
Others
Multiple organ f ailure
10 0
Number of deaths
Causes of death
Figure2 Causesofdeathof193childrenwithsicklecell
dis-easewhodiedbetween Marchof1998andFebruary of2012,
accordingtoinformationextractedfromdeathcertificates,the
databaseoftheNúcleodeAc¸õesePesquisaemApoio
Diagnós-tico(Nupad,UFMG),andinterviews.
wassignificant.Therewasnorecordingoftheterms‘‘SCD’’ or‘‘SCA’’ascauseofdeathinasignificantnumberofdeath certificates(46%).
Marchof2005toFebruaryof2012(117deaths)
Theinterviews(n=84)showedthat46.4%ofchildrenwere treatedwithinthefirst6hoursaftersymptomonsetduring the event that caused the death; 64.3%, within 24hours; and26.2%diedwithoutmedicalattention.Deathoccurred within12hoursof symptom onsetin 30% of cases and,in 40.5%,withinthefirst24hours.Fever,pain,pallor,and vomi-ting were the most common initial symptoms related to death, asreported by family members. The hospital was thefirsthealthcareservicesoughtbyapproximately60%of families,followedbyBasicHealthUnits(12%).
After the firstconsultation, 30 children were referred toothercareunits,24byambulance.Ofthese,threedied duringtransferandonediedbeforetransportarrived.Only 13.8%ofthechildrenweretransportedwhileonmedication. Regularuseofprophylacticantibioticsandfolicacidwas reportedby90%ofthefamilies.Approximately 74%ofthe childrenreceivedspecialimmunobiologicagents.Regarding theclinicalevolutionpriortodeath,58.3%ofthechildren hadbeenadmittedtothehospitalatleastonceand23.8%, morethanthreetimes.Painfulcrisishadoccurredinalmost 60%ofthechildrenbeforetheeventwhichresultedinthe death,and46.4%hadreceivedtransfusions.ASShadalready occurredin27.4%ofthechildren.
Regarding the socioeconomic status of families, 91.6% hadamonthlypercapitaincomeequaltoorsmaller than oneminimum wageand 50%received federal benefits.As foreducation,5%ofthefamilieswereilliterate.
Only54.8%ofthefamiliesreceivedregularvisitsofthe Family Health Program (FHP) agents while the child was alive.The cognitivequestionnaire applied tothe families (n = 41) showed that 85.4% obtained over 60% of correct answers.
Consideringthetotalof1,733appointmentsscheduledin bloodcentersforthe117children whodied,359 appoint-ments(20.7%)werenotattendedbecausethefamiliesfailed tocome.Allappointmentswererescheduled,butthe con-trolsystemdoesnotinformthesuccessofsuchprocedure.
Comparisonsbetweenthestudyperiods
In the first seven years, a total of 1,399 children were screenedand76deaths occurreduntilFebruary 28,2005, withamortalityrateof5.43%.Inthelastsevenyears,1,192 childrenwerescreenedand61died,withamortalityrate of5.12%(p=0.72).Inthefirstperiod,55/76deaths(72.4%) occurredbeforetheageof 2years;in thesecond period, 47/61(77.0%,p=0.53).Theremaining56deaths,totaling 193,occurredinchildrenborninthefirstsevenyears,but diedinthesecondperiodandthus,werenotincludedinthe statisticalcalculations.
In the first seven-year period, 25.3% of the deaths occurredathomeorintransit;inthesecond,themortality ratedecreasedto18.1%(p=0.28).Thelackofmedicalcare atthetimeofdeathalsodecreasedfrom28.0%to21.6%(p =0.39).Thementioningoftheterm‘‘sicklecell’’indeath certificateswassignificantlymorefrequent (60.5%) inthe lastseven-year period,whencomparedtothe firstperiod (42.1%,p=0.017).
Discussion
The sample reflects the overall health reality of children withSCDscreenedduringthe14yearsoftheNSP-MG,asall deathsof childrenfollowedatBloodBankClinicalCenters wereinformed.Thisrepresentsthetotalnumberofdeaths, whichconfiguresapopulation-basedstudy.
Thepresentstudy,asothers,11,12observednosignificant
differencebetweengenders in theincidence ofdeaths in
theassessedagerange.
Thisandseveralotherstudies11,13---17havedemonstrated
thatthe highest frequencyof deaths occurredin patients
withHbSS (79.3%), the most common and most clinically
severegenotype.Therelativelyhighfrequencyofdeathsin
childrenwithS+thalassemia(6.5%)doesnotcorrespondto
reality,asonlyfrom2010onwardsallsuspectedcasesofSCD
inNSP-MGwereconfirmedbymolecularbiologytechniques.
ThediagnosisofthissubtypeofSCDmaybeoverestimatedin
theneonatalperiodduetobloodtransfusionsnotreported
byfamilymembersorerrorsintheinterpretation ofsmall
concentrationsofHbA.
Threequartersofthechildrendiagnosedbetween2005
and2012underwentneonatalscreeningfor SCDinupto8
daysoflife,lesstimethanthe18daysintheinitialperiod
between1998and2005,10whichshowsimprovementofthe
NSP-MG.
The distribution of childrenper age range at the time
of death shows increased occurrence of deaths in those
younger than 5 years, similar to that observed by other
authors.11,18---22 Nonetheless, some authors4,8,12,16,23,24 have
reportedthatinfantmortalityrateduetoSCDisdecreasing
andthemedian ageofdeathis increasing.Inthe present
explainedbythehigherincidenceofpotentiallyfatalevents
inthisagegroup,suchasinfectionsandASS.
Althoughin-hospitaldeathswerethemostprevalent,it
isnoteworthy thatone-fifth ofthem occurred athome or
in-transit.This can be explainedby several factors,such
as family residence located far from the health service,
difficulty getting to the service, low socioeconomic and
educational levels, in addition to the family’s incapacity
to identify risk situations for the child. The statistically
non-significantincreaseof11%inthenumberofin-hospital
deathsshowsimprovement,albeitsmall,inthehealthcare
ofchildrenwithSCDinthelastsixyears.Astudyconducted
inAngola25concludedthatpatientswithSCDwholivedinthe
countrysideorinruralcommunitieswerethreetimesmore
likelytodie during hospitalization,due tosocioeconomic
factorsandlackofimmediateaccesstomedicalcare.
In the present study, as in many others,11,14,15,18,25---27
infectionappearsasthemain causeofdeath, considering
theagegroupsstudied.Thehighnumberofindeterminate
causessuggests adifficulty forphysicians andhealth care
professionalstorecognizeSCDanditssevereacuteevents
determinantsofdeath,asinthestudybyAlves,28giventhat
mostoftherecordscamefromin-hospitaldeaths.ASSwas
thethirdmostcommoncause,whichreflectsthedifficulty
byhealthteamsandfamiliestoidentifythiscomplication.
TheproportionofdeathscausedbyASSinSSchildrenwas
similartothatreportedinapreviousstudy,restrictedtoSS
children.29 Other authors13,15,19 indicated ASS asthe main
causeofdeathinchildrenyoungerthan3years.
Asignificantnumber(46%)ofdeathcertificatesdidnot
mentiontheterm‘‘sicklecell’’asthecauseofdeath.
How-ever,thenumberofcertificatesthatmentionthistermhas
increasedsignificantlyoverthepastsevenyears,indicating
greatervisibilityandawarenessofthediseasebyphysicians.
Mostchildren receivedmedicalcare beforedeath, but
25% of them were unassisted. An increase, albeit
non-significant,of13%inthefrequencyofmedicalcareprovided
tochildrenwithSCDbeforedeathwasobserved,whichonce
againindicatesaprobableincreaseoftheknowledgeabout
SCDbyphysicians.
Medicalcareoccurredwithinthefirst6hoursinalmost
halfthecasesandtwo-thirdsintheperiodofupto24hours.
Deathoccurredwithinthefirst24hoursofsymptom onset
inapproximately40%ofcases.Mancietal.15demonstrated
thatthe first 24hours afterthe onset of thepathological
processrepresent theperiodof greatestrisk of deathfor
patients with SCD. This emphasizes how fast the clinical
conditionworsens,culminatingindeath.
Highadherencetoantibioticprophylaxisandfolicacid,
in addition to the regular use of special immunobiologic
agents indicates that these data may be overestimated,
astheywereobtainedaposterioriandinthepresenceof
an ‘‘authorityfigure’’, i.e., the interviewer.Astudy
con-ducted at the Blood Bank Clinical Center of MG showed
lowerlevelsof adherencetoantibiotic prophylaxis.30 The
incorporationof‘‘specialvaccines’’tothebasicvaccination
scheduleoccurredonlyrecently,andmayhavecontributed
tothelow adherence of families.This is probablydue to
thelackofawarenessbyhealthprofessionalsregardingthe
specialimmunizationscheduleandthelackofprioritywhen
requestingspecialimmunobiologicagentsbythe
municipal-ities.
Atthetimeofthechild’sdeath,onlylittlemorethanhalf
ofthefamiliesregularlyreceivedvisitsfromtheFHPteam.
ConsideringthatSCDisachronicdiseasewiththepossibility
ofsevereacuteevents,inadditiontothefactthatitaffects
low-incomefamilies,bettermonitoringbytheFHPthrough
homevisitswasexpected,inordertoensuretheinclusion
ofthesepatientsinthehealthcaresystem.
Lackofpriorityand/ordelayintreatment,lackof
knowl-edge by the team and poor health service infrastructure
weredifficultiesreportedbythefamiliesthatmayhave
con-tributedtodeath.Lowparentaleducationallevelandlow
incomeconstituteadditionalbarriers.Astudyconductedin
Gabon,Africa,21alsoreportedthatthevastmajority(91.3%)
of children withSCD whodied were fromfamilies of low
socioeconomicstatus.Inadequatetransportconditionswere
alsoreportedbysomefamilies,suchasoxygencylinderwith
insufficientorabsentvolumefortheentiretransfer,
inade-quateoxygenmasksizeforthechild,amongothers.
Thecognitivequestionnaireadministeredto41families
indicatesthatknowledgeaboutSCDisstillprecarious,even
aftertheoccurrenceofsuchanimportanteventasthedeath
ofachild.
The main limitation of the study was itsretrospective
design,aslocatingthefamiliesbecomesmoredifficultover
theyears,aswell astheir incapacitytoaccurately report
some of the data.The interviews added a moreaccurate
qualitative character to the study, rather than a simple
assessment of deathcertificates. In the authors’ opinion,
the absence of 33 interviews, in 117, did not impair the
desiredgoals.
It can be concludedthat low socioeconomic and
edu-cational levels of families,difficulties in accesstohealth
services, lack of transportation, lack of priorityin health
care, and lack of knowledge about SCD by health
profes-sionals were aggravating factors for the clinical status of
thechild.
ScreeningforSCD,evenwhenperformedina
comprehen-siveandeffective way,wasstillnotenoughtoreduce the
mortalityrateobservedattheNSP-MG.Socialandeconomic
developmentinthestatearenecessarytochangethis
sce-nario.Careofacuteevents,consultationswithspecialists,
adequatetransportationofpatients,andcontinuing
educa-tionforfamiliesandhealthcareteamsshouldberecognized
asapriorityinthecareofpatientswithSCD.
Funding
Conselho Nacional de Desenvolvimento Científico e Tec-nológico(CNPq) andNúcleodeAc¸õesePesquisaemApoio Diagnóstico(Nupad).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
financialsupportatthedifferentstagesoftheresearch.To CNPq,whichusedpartoftheproceedsfromtheUniversal Demand Project No. 471019/2011-9 to allow the perfor-manceofsomevisits for datacollection.To Dr.AnaPaula FernandesPinheiroChagasforsuggestingthetopic,aswell asher assistance and encouragement at all stages of the research.
References
1.LoboCL,BallasSK,DomingosAC,MouraPG,doNascimentoEM, CardosoGP, et al.Newborn screening programfor hemoglo-binopathies in Rio de Janeiro. Brazil Pediatr Blood Cancer. 2014;61:34---9.
2.PereiraSA,BrenerS,CardosoCS,ProiettiAB.Sicklecelldisease: qualityoflifeinpatientswithhemoglobinSSandSCdisorders. RevBrasHematolHemoter.2013;35:325---31.
3.Felix AA, Souza HM, Ribeiro SB. Aspectos epidemiológicos esociais da doenc¸a falciforme.Rev Bras Hematol Hemoter. 2010;32:203---8.
4.Quinn CT. Sickle cell disease in childhood: from newborn screeningthroughtransitiontoadultmedicalcare.PediatrClin NorthAm.2013;60:1363---81.
5.SerjeantGR. The naturalhistory ofsickle cell disease. Cold SpringHarbPerspectMed.2013;3:a011783.
6.HankinsJ.Towardhighqualitymedicalcareforsicklecell dis-ease:arewethereyet?JPediatr(RioJ).2010;86:256---8.
7.McGannPT.Sicklecellanemia:anunderappreciatedand unad-dressedcontributorto global childhood mortality. JPediatr. 2014;165:18---22.
8.Hamideh D, Alvarez O. Sickle cell disease related mortal-ity in the United States (1999-2009). Pediatr Blood Cancer. 2013;60:1482---6.
9.Canc¸adoRD,JesusJA.Adoenc¸afalciformenoBrasil.RevBras HematolHemoter.2007;29:204---6.
10.FernandesAP,JanuárioJN,CangussuCB,MacedoDL,VianaMB. Mortalityofchildrenwithsicklecelldisease:apopulationstudy. JPediatr(RioJ).2010;86:279---84.
11.Leikin SL, Gallagher D, Kinney TR, Sloane D, Klug P, Rida W.Mortality inchildrenandadolescentswithsickle cell dis-ease. Cooperative Study of Sickle Cell Disease. Pediatrics. 1989;84:500---8.
12.Shankar SM, Arbogast PG, Mitchel E, Cooper WO, Wang WC, Griffin MR. Medical care utilization and mortality in sicklecell disease:a population-basedstudy.AmJHematol. 2005;80:262---70.
13.Rogers DW, Clarke JM, Cupidore L, Ramlal AM, Sparke BR, SerjeantGR.EarlydeathsinJamaicanchildrenwithsicklecell disease.BrMedJ.1978;1:1515---6.
14.GillFM,SleeperLA,WeinerSJ,BrownAK,BellevueR,Grover R,etal.Clinicaleventsinthefirstdecadeinacohortofinfants
withsickle celldisease.CooperativeStudyofSickleCell Dis-ease.Blood.1995;86:776---83.
15.ManciEA,CulbersonDE,YangYM,GardnerTM,PowellR,Haynes JJr,et al.Causesofdeathinsicklecelldisease:anautopsy study.BrJHaematol.2003;123:359---65.
16.QuinnCT, RogersZR,BuchananGR. Survivalofchildrenwith sicklecelldisease.Blood.2004;103:4023---7.
17.Houston-YuP,RanaSR,BeyerB,CastroO.Frequentand pro-longedhospitalizations:ariskfactorforearlymortalityinsickle celldiseasepatients.AmJHematol.2003;72:201---3.
18.SeelerRA.Deathsinchildrenwithsicklecellanemia.Aclinical analysisof19fatal instancesinChicago.ClinPediatr(Phila). 1972;11:634---7.
19.ThomasAN,PattisonC,SerjeantGR.Causesofdeathin sickle-cell disease in Jamaica. Br Med J (Clin Res Ed). 1982;285: 633---5.
20.PlattOS,BrambillaDJ, RosseWF,MilnerPF,CastroO, Stein-bergMH,etal.Mortalityinsicklecelldisease.Lifeexpectancy and risk factors for early death. N Engl J Med. 1994;330: 1639---44.
21.KokoJ,DufillotD,M’Ba-MeyoJ,GahoumaD,KaniF.Mortality ofchildrenwithsicklecelldiseaseinapediatricdepartmentin CentralAfrica.ArchPediatr.1998;5:965---9.
22.MakaniJ,CoxSE,Soka D,KombaAN, OruoJ, MwamtemiH, etal. Mortalityinsicklecell anemiainAfrica: aprospective cohortstudyinTanzania.PLoSOne.2011;6:e14699.
23.Loureiro MM. Epidemiologia das internac¸ões hospitalares e tratamentofarmacológicodoseventosagudosemdoenc¸as fal-ciformes [thesis]. Rio de Janeiro: Escola Nacional de Saúde Pública,Fundac¸ãoOswaldoCruz;2006.
24.YanniE,GrosseSD,YangQ,OlneyRS.Trendsinpediatricsickle celldisease-relatedmortalityintheUnitedStates,1983-2002. JPediatr.2009;154:541---5.
25.Van-DunemJC,AlvesJG,BernardinoL,FigueiroaJN,BragaC, doNascimento M,deL,et al.Factorsassociatedwithsickle celldiseasemortalityamonghospitalizedAngolanchildrenand adolescents.WestAfrJMed.2007;26:269---73.
26.GillFM,BrownA,GallagherD,DiamondS,GoinsE,GroverR, etal.NewbornexperienceintheCooperativeStudyofSickle CellDisease.Pediatrics.1989;83:827---9.
27.MillerST,SleeperLA,PegelowCH,EnosLE,WangWC,Weiner SJ,etal.Predictionofadverseoutcomesinchildrenwithsickle celldisease.NEnglJMed.2000;342:83---9.
28.AlvesAL.Estudodamortalidadeporanemiafalciforme.Informe EpidemiológicodoSUS.1996;5:45---53.
29.RezendePV,VianaMB,MuraoM,ChavesAC,RibeiroAC.Acute splenic sequestrationina cohortofchildrenwithsickle cell anemia.JPediatr(RioJ).2009;85:163---9.