www.jped.com.br
ORIGINAL
ARTICLE
Serum
TSH
levels
are
associated
with
cardiovascular
risk
factors
in
overweight
and
obese
adolescents
夽
Luciana
Lopes
de
Souza
a,∗,
Erika
Paniago
Guedes
a,
Patrícia
Fátima
dos
Santos
Teixeira
b,
Rodrigo
Oliveira
Moreira
a,
Amelio
Fernando
Godoy-Matos
a,
Mario
Vaisman
baInstitutoEstadualdeDiabeteseEndocrinologia(IEDE),DivisãodeMetabologia,RiodeJaneiro,RJ,Brazil bUniversidadeFederaldoRiodeJaneiro(UFRJ),DivisãodeEndocrinologia,RiodeJaneiro,RJ,Brazil
Received30August2015;accepted14January2016 Availableonline22June2016
KEYWORDS
Subclinical hypothyroidism; Adolescents; Obesity; Overweight; Cardiovascularrisk factors
Abstract
Objective: Toinvestigatetherelationshipbetweenserumthyrotropin(TSH),insulinresistance
(IR),andcardiovascularriskfactors(CRF)inasampleofoverweightandobeseBrazilian
ado-lescents.
Methods: Aretrospective,longitudinalanalysisof199overweightandobesepubescent
ado-lescentswasperformed.TheTSHandfreeT4(fT4)levels,anthropometricmeasurements,and
laboratorytestresultsofthesepatientswereanalyzed.
Results: 27individuals(13.56%)presentedwithTSHlevelsabovethenormallevel
(subclini-calhypothyroidism[SCH]).Theirwaistcircumference(WC)wassignificantlyhigherthanthose
of euthyroidindividuals. Serum TSH was positively correlated with the homeostasis model
assessmentofinsulinresistance(HOMA-IR)index,triglycerides(TG)andhigh-density
lipopro-teincholesterol(HDL-C).UsingTSHandBMIasindependentvariables,TSHlevelswereshown
tobeindependentlyrelatedtoHOMA-IR(p=0.001)andTG(p=0.007).Amongeuthyroid
sub-jects,individualswithTSHvalues<2.5mIU/mLexhibitedstatisticallysignificantdecreasesin
waist-to-hipratio,HDL-Clevels,andHOMA-IRscoresandatendencytowardlowerWCvalues.
Conclusion: SCHinoverweight andobeseadolescentsappears tobeassociated withexcess
weight,especiallyvisceralweight.Ineuthyroidadolescents,thereappearstobeadirect
rela-tionshipbetweenTSHandsome CRF.Inconclusion,inthepresentsampleofoverweightand
obeseadolescents,TSHlevelsappeartobeassociatedwithIRandCRF.
©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen
accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/
4.0/).
夽
Pleasecitethisarticleas:SouzaLL,GuedesEP,TeixeiraPF,MoreiraRO,Godoy-MatosAF,VaismanM.SerumTSHlevelsareassociated withcardiovascularriskfactorsinoverweightandobeseadolescents.JPediatr(RioJ).2016;92:532---8.
∗Correspondingauthor.
E-mail:[email protected](L.L.Souza).
http://dx.doi.org/10.1016/j.jped.2016.01.011
0021-7557/©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND
PALAVRAS-CHAVE
Hipotireoidismo subclínico; Adolescentes; Obesidade; Sobrepeso; Fatoresderisco cardiovascular
NíveisdeTSHséricaassociadosafatoresderiscocardiovascularemadolescentes acimadopesoeobesos
Resumo
Objetivo: Investigararelac¸ãoentretireotrofinasérica(TSH),resistênciaàinsulina(RI)efatores
de riscocardiovascular(FRC) em umaamostrade adolescentesbrasileirosacimadopesoe
obesos.
Métodos: Foirealizada uma análiselongitudinal retrospectivade190 adolescentespúberes
acima do peso e obesos. Foram analisados os níveis de TSH e T4 livre (T4l), as medidas
antropométricaseosresultadosdeexameslaboratoriaisdessespacientes.
Resultados: 27 indivíduos (13,56%) apresentaram níveis de TSH acima do normal
(hipotireoidismosubclínico(HSC)).Elesapresentaramcircunferênciadacintura(CC)
significati-vamentemaiorqueosindivíduoseutireoideos.ATSHséricafoipositivamentecorrelacionadaao
índicedomodelodeavaliac¸ãodahomeostasederesistênciaàinsulina(HOMA-IR),triglicerídeos
(TG) e lipoproteína de alta densidade-colesterol (HDL-C). Usando TSH e IMC como
var-iáveis independentes, os níveis de TSH estavam relacionados ao HOMA-IR (p=0.001) e a
TG (p=0.007)de formaindependente.Entreospacienteseutireoideos, indivíduoscom
val-ores de TSH<2.5mIU/mL apresentaram reduc¸ões estatisticamente significativas na razão
cintura/quadril,nosníveisdeHDL-CenosescoresdeHOMA-IRetendênciaamenoresvalores
deCC.
Conclusão: OHSCemadolescentesacimadopesoeobesospareceestarassociadoaoexcesso
de peso,principalmente depeso visceral.Em adolescenteseutireoideos, parecehaveruma
relac¸ãodiretaentreTSHealgunsFRC.Concluindo,emnossaamostradeadolescentesacima
dopesoeobesos,osníveisdeTSHparecemestarassociadosaRIeFRC.
©2016SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo
OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.
0/).
Introduction
The incidence of obesity in childhood andadolescence is increasingindevelopinganddevelopedcountries.1InBrazil, adevelopingcountry,datafromtheHouseholdBudget Sur-vey(PesquisadeOrc¸amentosFamiliares[POF])showedthat thepercentageofoverweightindividualsbetweentheages of 10 and 19 increased from 3.7% (1974---1975) to 21.7% (2008---2009)inmalesandfrom7.6%to19.4%infemalesin thesameperiods.2
The well-established association between obesity and glucose/lipid metabolism disorders, hypertension and increased cardiovascular risk (CVR) is frequently referred toasmetabolicsyndrome(MetS).3Individualsinthe pedi-atric age group may also show increased MetS-related morbidity.3---5
Thyroid hormones (TH) play a key role in regulating metabolismthroughthe modulationof thermogenesis and energyexpenditure.TheputativerelationshipsbetweenTH, bodyweight,andadiposetissuehomeostasishavebeenthe focusofseveralstudiesinrecentyears,butthecausal rela-tionships between these parameters have not been well established.6---12 One review8 included several population-basedstudiesthatrevealedacorrelationbetweenincreased serumthyrotropin(TSH)levelsandincreasedBMI.
Thyroiddiseaseshave beenassociatedwith atheroscle-rotic cardiovasculardisease.13---16 Although thisassociation has been documented conclusively for overt hypothy-roidism,itremains controversialwhetheritisalsopresent insubclinicalhypothyroidism(SCH).17,18 Theassociationof
thyroiddiseaseswithatheroscleroticcardiovasculardisease maybepartiallyexplainedbytheroles ofTHin the regu-lationoflipidmetabolismandbloodpressure(BP).Indeed, severalrecentpopulation-basedstudieshaveobserved pos-itive correlations between TSH and lipid parameters and betweenTSHandBP,evenineuthyroidpopulations.6---18This studyaimedtoinvestigatetherelationshipbetweenthyroid function,obesity,lipids,insulinresistance,andMetS com-ponentsina sampleof overweightadolescents.The study alsoaimedtoassessthemetabolicandanthropometric dif-ferencesofeuthyroidpatientswithTSHintheupperlimit ofnormality(≥2.5IU/mL)incomparisontopatientsinthe lowerlevels.
Patients
and
methods
Subjects
This exclusion criteria included the following: pre-pubertal patients; previous diagnosis of either type 1 or type2diabetes(T2DM); patientswhowerereceiving anti-diabetic and/or anti-obesity medications; those who had an endocrinedisease diagnosis; diagnosed thyroiddisease (theuseoflevothyroxine(LT4)orthionamides);creatinine and urea levels above normal values; aspartate amino-transaminase (AST) and/or aspartate alaninotransferase (ALT)threetimesabovetheupperlimitofnormality;alcohol ordrugabuse;chronicandconstant-doseconcomitantuse ofbeta-blockers,beta-agonists,diuretics,antidepressants, neuroleptics, bromocriptine, ergotamine,andderivatives, atropine,systemicsteroids,appetitesuppressants,ordrugs thatinterferewithamineactivityorareusedtotreat psy-chiatricdisorders withinthe past threemonths;pregnant andlactatingfemales;orahistoryofneoplasiainthepast fiveyears.
Anthropometricexamination
All participants underwent a complete medical history-takingandphysicalexam.Familymembersand/orguardians assistedinprovidinginformationaftersigningtheinformed consent form.The following parameters were evaluated: weight(kg),height(m),bodymassindex(BMI;kg/m2),waist
circumference(WC),waist-to-hipratio(WHR),BP(mmHg), anddemographicfactors(genderandage).Weight measure-mentswereobtainedusingadigitalscaleFilizola®(Filizola®,
SP,Brazil)whileeachpatientwasbarefootandwearinglight clothing. The height of each patientwas measured using aHarpenden® (Harpenden®,United Kingdom)stadiometer
withtheindividualbarefoot.WCwasmeasuredatthe mid-point between the iliac crest and the costal margin. Hip circumference(HC)wasobtainedbymeasuringthelargest diameteroverthegreattrochanters. The WHRwas calcu-latedbydeterminingtheratiobetweenWCandHC.BMIwas calculatedbydividingtheweight(kg)bytheheightsquared (m2).
The American charts from the Centers for Dis-ease Control and Prevention National Center for Health Statistics (CDC-NCHS) were used to assess BMI (http://apps.nccd.cdc.gov/dnpabmi/), according to gen-der and age. Individuals with a BMI-for-age between the 85thandthe95thpercentilewereclassifiedasoverweight and those with a BMI-for-age at or above the 95th per-centilewereclassifiedasobeseBPwasobtainedwiththe patient in a supine position after 5min of rest. All BP measurementswereobtained bythesameexaminer using thesameequipment.ForBPmeasurements,astandardized and calibrated mercury-column sphygmomanometer was usedwith the cuffs adjusted tothe body dimensions. All anthropometricmeasurementswereevaluatedbythesame examiner,andthesexualmaturationstagewasdetermined usingtheTannerclassificationofpubertaldevelopment.
Laboratoryevaluations
Bloodsampleswerecollected aftera 12-h fastingperiod, andtheresultsfromthefollowingblood testswere evalu-ated:fastingglucose,2-hglucosefollowingglucoseoverload with75gdextrosol,completebloodcount,urea,creatinine,
sodium,potassium,totalcholesterol,high-density lipopro-teincholesterol(HDL-C),low-densitylipoproteincholesterol (LDL-C), triglycerides, ALT, AST, TSH, free T4 (fT4), and basalinsulin.Usingtheresultsoffastingglucoseandbasal insulin, the homeostasis model assessment-insulin resis-tance(HOMA-IR)indexforeachpatientwascalculatedusing thefollowing formula:HOMA-IR=[Glucose(mMol)×Insulin (U/mL)]/22.5. The Brazilian Metabolic Syndrome Study
(BRAMS) evaluated a population of approximately 2000 patients, including obeseand type 2 diabeticadults, and defined insulin resistance (IR) as a HOMA-IR index value greaterthan2.71inindividualswithnormalBMI.19This cut-offforHOMA-IRislikelytoberepresentativeoftheBrazilian population,giventhenumberofpatientsevaluated.
To evaluate TSH levels, an electrochemiluminescence methodwasemployed.Electrochemiluminescenceconsists ofanimmunoassaythatquantitativelydeterminesTSH lev-els from human serum and plasma samples. The normal range of values that have been reportedusing this kit is 0.5---5.0IU/mL. The fT4 levelsof the patients were also evaluatedbyelectrochemiluminescence,andthereference valuesrangedbetween 0.8and1.9ng/mL.The fT4values wereonlyusedtoexcludepatientsintheeventthatvalues outsideofthenormalrangewereobtained.
ForthediagnosisofSCHinadolescents,itwouldbe nec-essarytousespecificvaluesaccordingtogender,age,and Tannerstage.However,thesedataarenotavailableforthe Brazilian population. Therefore, thediagnosis of SCH was basedontherecommendation14.1oftheClinicalPractice GuidelinesforHypothyroidisminAdults,cosponsoredbythe American Association of Clinical Endocrinologists and the American ThyroidAssociation20: the reference rangeof a given laboratory exam should determine the upper limit ofnormalforathird-generationTSHassay.Therefore,the diagnosisofSCHwasdefinedasnormalfT4associatedwith TSHabove5.0IU/mL.
Euthyroid patients were also divided into two groups according toTSH levels.There has been some discussion aboutloweringtheuppervalueofTSHto2.5IU/mL.This discussionisbasedinsomedatathatindicatedthatpatients withTSH≥2.5mayhavedifferentprofilesthanthosewith TSH<2.5IU/mL.21,22
Statisticalanalysis
Data were analyzed using the GraphPad® InStat 3.00
(GraphPad® Software, USA). The different groups were
compared using Student’s t-tests for parametric varia-blesandMann---Whitneytestsfor nonparametricvariables. For parametric variables, the data are presented as means±standard deviations.Fornonparametricvariables, thedataarepresentedasmedianswithmaximumand min-imumvalues.Correlational analyses wereperformed with Pearson’stestforparametricvariablesandSpearman’stest fornonparametricvariables.Alltestsweretwo-tailed,and thelevelofsignificancewassetatp=0.05forallanalyses.
Results
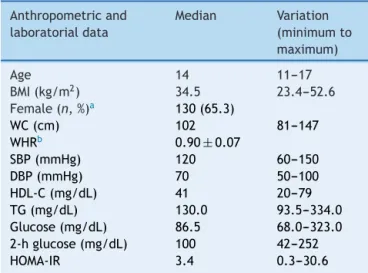
Table1 Anthropometricandmetabolicdataofthestudied sample.
Anthropometricand
laboratorialdata
Median Variation
(minimumto
maximum)
Age 14 11---17
BMI(kg/m2) 34.5 23.4---52.6
Female(n,%)a 130(65.3)
WC(cm) 102 81---147
WHRb 0.90±0.07
SBP(mmHg) 120 60---150
DBP(mmHg) 70 50---100
HDL-C(mg/dL) 41 20---79
TG(mg/dL) 130.0 93.5---334.0
Glucose(mg/dL) 86.5 68.0---323.0 2-hglucose(mg/dL) 100 42---252
HOMA-IR 3.4 0.3---30.6
BMI,bodymassindex;WC,waistcircumference;WHR, waist-to-hipratio;SBP, systolicbloodpressure;DBP,diastolicblood pressure; HDL-C, high-density lipoprotein cholesterol; TG, triglycerides; HOMA-IR, homeostasismodel assessment-insulin resistance.
a Dataforfemalegenderispresentedasthenumberof
indi-vidualsandpercentage.
b DataforWHRareexpressedasthemean±standarddeviation
becausethesamplehasaparametricdistribution.
AllpatientswereaboveTannerstageIIforpubertal devel-opment.Thefrequencyofoverweightwas6.97%according totheCDC-NCHSchart,andobesitywaspresentin93.03%of patients.Table1showstheanthropometricandmetabolic dataofthestudiedpopulation.
Regarding glucose metabolism, 13.56% of the sample (27 outof 199) had abnormalfasting glucoselevels (i.e., between 100 and 125mg/dL). In addition, 6.03% (12 out of199) hada2-hglucoselevel followingachallengewith
75gdextrosol between140 and 200mg/dL andwere thus classifiedashavingimpairedglucosetolerance.Finally,four patients (2.02%) received a diagnosis of T2DM. Using the cutoff point for IR that was obtained in the aforemen-tionedBrazilianstudy(aHOMA-IRvalueabove2.7),61.19% (122outof199) ofthepatients presentedIR.Nochanges in fasting glucose or OGTT were observed in overweight patients.
Thyroidfunction was evaluatedby measuringTSH lev-els(normalrange:0.5---5.0IU/mL).Two(1.0%)individuals exhibited TSH levels below the normal range (subclinical hyperthyroidism), and 27 individuals (13.56%) presented with TSH levels above the normal level (SCH). All these patients had fT4 within normal limits. No patient was diagnosed with overt hypothyroidism (low fT4 and TSH above 5.0IU/mL). Patients with subclinical hyperthy-roidism(n=2)werenotincludedintheanalysis.
Table2shows a comparisonof theanthropometricand metabolic parameters of adolescents diagnosed with SCH andeuthyroid adolescents.Patients withSCH exhibited a significantlyhigherWCthanthosewithnormalthyroid func-tion.Nosignificantdifferenceswereobservedbetweenthe groupsinanyofthemetabolicparametersexamined.
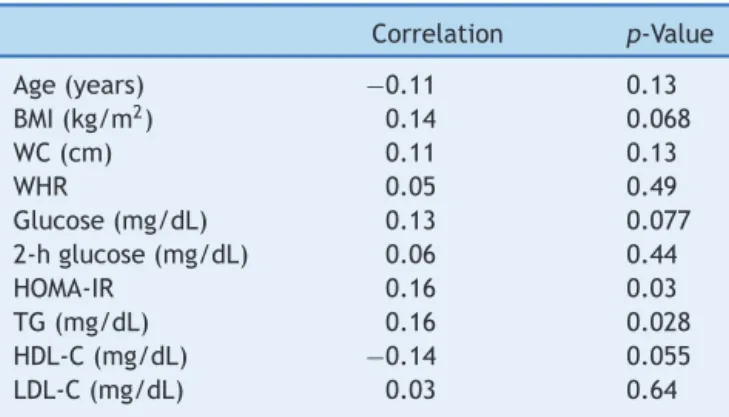
After excluding patients with SCH, the 170 remaining patients(TSHlevelswithinthenormalrange)wereanalyzed separately.Table3showsthecorrelationsbetweenTSH lev-elsandvariousanthropometricandmetabolicparametersin individualswithnormalthyroidfunction.
Multiple linear regression analysis was used to assess the relationship between TSH and metabolic parameters. Inthisfirstmodel,TSHandBMIwereusedasindependent variablesandeachmetabolicparameterasthedependent variable. After regression, TSH levels remained indepen-dentlyassociatedwithHOMA-IR(p=0.001),HDL(p=0.046), andTGlevels(p=0.007).Thesameanalysiswasalsousedto assesswhethertherelationshipbetweenTSHandmetabolic parameterswouldremain statisticallysignificant indepen-dentofageandgender.Inthissecondmodel,age,gender,
Table2 Acomparisonofmetabolicandanthropometricparametersbetweenadolescentswithsubclinicalhypothyroidism(SCH)
andthosewithnormalthyroidfunction.
Normal(n=170) SCH(n=29) p
Age(years) 14.0(11---17) 14.0(12---18) 0.33
BMI(kg/m2) 34.2(23.4---52.6) 37.2(25.8---51.9) 0.046
WC(cm) 102(72---148) 111(81---134) 0.0027
WHR 0.91±0.08 0.93±0.05 0.22
SBP(mmHg) 120(80---160) 120(90---160) 0.48
DBP(mmHg) 70(50---100) 80(50---100) 0.34
Glucose(mg/dL) 87.0(68---323) 91.0(75---268) 0.087
2-hglucose(mg/dL) 102.0(42---252) 107.0(72---200) 0.38
HOMA-IR 3.4(0.2---50.7) 3.7(1.0---30.5) 0.19
AST(mg/dL) 19(7---67) 21(13---39) 0.18
ALT(mg/dL) 16(6---80) 20(9---54) 0.09
TG(mg/dL) 95.0(30---356) 100.0(30---210) 0.26
HDL-C(mg/dL) 41.5(20---74) 40.0(26---79) 0.11
LDL-C(mg/dL) 94.1±25.3 99.8±24.8 0.26
BMI,bodymassindex;WC,waistcircumference;WHR,waist-to-hipratio;SBP,systolicbloodpressure;DBP,diastolicbloodpressure; HOMA-IR,homeostasismodelassessment-insulinresistance;TG,triglyceride;AST,aspartateaminotransferase;ALT,aspartatealanine transferase;HDL-C,high-densitylipoproteincholesterol;LDL-C,low-densitylipoproteincholesterol.
Table3 Correlationsbetweenserumthyrotropin(TSH)
lev-elsandvariousanthropometricandmetabolicparametersin
170adolescentswithnormalthyroidfunction.
Correlation p-Value
Age(years) −0.11 0.13
BMI(kg/m2) 0.14 0.068
WC(cm) 0.11 0.13
WHR 0.05 0.49
Glucose(mg/dL) 0.13 0.077
2-hglucose(mg/dL) 0.06 0.44
HOMA-IR 0.16 0.03
TG(mg/dL) 0.16 0.028
HDL-C(mg/dL) −0.14 0.055
LDL-C(mg/dL) 0.03 0.64
BMI,bodymassindex;WC,waistcircumference;WHR, waist-to-hip ratio; HOMA-IR, homeostasis model assessment-insulin resistance;TG, triglycerides; HDL-C, high-density lipoprotein cholesterol;LDL-C,low-densitylipoproteincholesterol.
and TSH levels were used as independent variables and eachmetabolicparametersasthedependentvariable.After regression,TSHremainedindependentlyrelatedto HOMA-IR(p=0.0015)andtriglycerides(p=0.0092).Atrendtoward significancewasstillfoundforHDLcholesterol(p=0.0508) andfastingglucose(p=0.0706).
Table 4 shows a comparison of anthropometric and metabolic parameters of individuals with normal thyroid functionbasedonaTSH cutoffvalueof 2.5IU/mL. Indi-vidualswithTSHlevels>2.5hadhigherWHR andHOMA-IR andatrendtowardhigherWC.
Discussion
In this sample of obese and overweight adolescents, 85% of patients exhibited normal thyroid function and 13.63% exhibitedSCH.ThefrequencyofSCHobservedinthissample washigherthanthatreportedintheliterature,evenusing a cutoffvalue of 5.0IU/mL. In the pediatric population
ingeneral,theprevalence ofSCHislessthan2%,butitis
importanttonote thatepidemiological studiesinthis age grouparescarce.
Several studies have indicated a positive correlation between weight and TSH levels in children. These stud-ieshavealsodemonstratedthat10---23%of obesechildren have moderatelyhigh levelsof TSH(4---10IU/mL), which
areassociatedwithnormallevelsoffT4orslightlyelevated fT4and/orfT3levels.ThelevelsofTSH inobesechildren andadultshavebeenconsistentlyreportedtobeelevated when compared with normal weight individuals.8,9,12,23,24 Prior researchhasrevealed notonlyapositivecorrelation between BMI andTSH, but also between five-yearweight gainandagradualincreaseinserumTSHlevels.8Thisisthe firststudytoevaluateTSHlevelsinaSouthAmerican popu-lationofobesechildren.ConsideringthatRiodeJaneiroisat anurbanareainBrazil,withnoiodinedeficiency,no reason-ableexplanationfortheelevatedprevalenceofSCHfound inthepresentstudycouldbeidentified.Furtherstudiesare necessary toinvestigate whetherthe prevalenceofSCH is higherinBraziland/orotherSouthAmericancountries.
When patients with SCH were compared with euthy-roid individuals, it was observed that patients with SCH hadhigherWC.This findingisextremelyimportant,asWC provides information regarding the fat distribution. The prevalence of acentraldistribution offat correlateswith increased CVR,and WCappears tobe thebest anthropo-metricmethod for evaluatingthisdistribution in pubertal adolescents and children, although this remains open to debate.6,25Centralorabdominalobesity,whichis character-izedbyincreasedWC,hasbeenshowntobecorrelatedwith SBP,DBP,totalcholesterol,TGs,LDL-C,andHDL-C.4---8Inan articlepublishedbyBlüheretal.,BMIandWCwerereported tobethebestanthropometricpredictorsof comorbidities in obese pubertal adolescents.25 Thus, the correlation of TSH with WCcontributes toits possible relationship with IRandincreasedCVR.Severalstudiesinchildrenand ado-lescentshave demonstratedtherelationshipbetween TSH andBMI,butfewofthesehavereportedastatistically sig-nificant relationship with WC.26---28 Interestingly, although severalanthropometricparametersofadolescentswithSCH werealtered,nolaboratory abnormalities wereobserved. Perhapsthesedatasuggestthat,atthisearlytimeoflife,
Table4 Comparisonofanthropometricandmetabolicparametersinadolescentsaccordingtotheserumthyrotropin (TSH)
cutofflevel.
TSH<2.5(n=60) TSH≥2.5(n=110) p
Age(years) 14.0(12---17) 14.0(11---17) 0.024
BMI(kg/m2) 34.1(23.4---50.2) 34.5(23.9---52.6) 0.11
Waist(cm) 100.9±13.6 105.3±14.3 0.054
WHR 0.89±0.08 0.92±0.07 0.04
Glucose(mg/dL) 87.0(72---323) 87.0(68---133) 0.55
2-hglucose(mg/dL) 101.0(43---166) 102.5(42---252) 0.53
HOMA-IR 2.71(0.37---17.22) 3.51(0.20---50.70) 0.028
TG(mg/dL) 93.0(36---214) 95.0(30---356) 0.25
HDL-C(mg/dL) 45.0(27---74) 40.0(20---68) 0.023
LDL-C(mg/dL) 92.1±25.2 95.1±25.4 0.46
Dataarepresentedasmedian(minimum---maximum),exceptforwaist,WHR,andLDL---C,whicharepresentedasmean±SD.
excessweightandvisceralfatmaynotbesufficientto trig-ger metabolic changes. However,it is possible that these changeswillbeidentifiedinthefuture.Prospectivestudies areneededtoevaluatethishypothesis.
In the euthyroid individuals, a weak, but statistically significant, correlation was observed between TSH and HOMA-IR, HDL, and TG. Using TSH and BMI as indepen-dentvariables,TSHwasfoundtobeindependentlyrelated to HOMA-IR and TG.An Italian study that also made this comparison in overweight children showed that patients withhighTSHlevelshadsignificantlyhigher levelsof ALT, gamma-glutamyl transferase(GGT),totalcholesterol, TG, insulin, and HOMA-IR.26 Likewise, in a Turkish study, TSH was positively correlated with total cholesterol, TG, and SBP.27Anotherstudyofeuthyroidobeseadolescentsand chil-dren whounderwentrapid weightloss concludedthat the decreaseinTSHresultedinareductionofover 50%inthe levelsoffastinginsulinandHOMA-IRregardlessofchanges inweightor bodycomposition.This improvementwasnot associatedwithweightloss,butwithareductioninserum TSH levels.Thesedata suggest thatalterations of thyroid functioninobesityarenotsimplyadaptivemechanisms.28
Evenwhenexaminingonlyeuthyroidpatients,individuals withhigher TSH levels(>2.5IU/mL) hadhigher HOMA-IR and WHR, lower levels of HDL-C, and a tendency toward lowerWC.There havebeen relativelyfew studies investi-gatingeuthyroidobeseadolescents,butthecorrelationof HOMA-IRwithTSHhasbeenreportedinseveralstudies.26---28 Ruhlaetal.13 foundthateuthyroidindividualswithTSHin theuppernormalrange(2.5---4.5)havehigherTGlevelsand anincreasedincidenceofMetS.Roosetal.alsoreportedan associationbetweenMetScomponentsandthyroidfunction inindividualswithSCHandineuthyroidindividuals.Inthis study,euthyroidpatientswithTSHintheupperportionof thenormalrangedisplayedhigherlevelsoftotalcholesterol, glucose,insulin,andHOMA-IR.29
Theaforementionedevidence,inadditiontothepresent results, reinforcesthe relationship between thyroid func-tion, especially TSH levels, and IR. In patients with hypothyroidism, IR has been well documented in muscle and fat tissue, and it results in impaired glucose absorp-tion and decreased gluconeogenesis in skeletal muscle.25 Thesemetabolicchanges havebeen showntobereversed with LT4 replacement therapy. Several studies have also reportedthepresenceofIRinSCH.6,15When assessingthe lipidprofiles of patientswith SCH, most studies have not foundsignificant differencesinthemeantotalcholesterol levelsofSCHpatientswhencomparedwitheuthyroid indi-viduals,althoughsomestudieshavenoteddifferencesinthe frequencyofdyslipidemiabetweenthesegroups.30
Thepresentstudyhasseverallimitations.First,thefact that it was a cross-sectional study prevented the estab-lishment of temporal relationships between the variables under investigation. In addition, because this study was performedretrospectively,theauthorswereunableto ana-lyze other parameters, including the levels of fT3, tT3, andleptin.Moreimportantly,thyroidantibodieswerealso notevaluated.Therefore,itwasnotpossibletodetermine whether this increased frequency of SCH was related to Hashimoto’sthyroiditis or anotheretiology. Alongitudinal studythatfollowseachgroupoveragivenperiodandmakes repeatedevaluationsandobservationsmayleadtodifferent
conclusions; future studies aretherefore needed. Finally, the diagnosis of SCH should have been based on specific valuesofTSH accordingtogender, age,andTannerstage. Unfortunately,thesedataarenotavailablefortheBrazilian population.Therefore,thediagnosiswasbasedsolelyinthe cutoffvalueofthekit.
Insummary,thefrequencyofSCHisapproximately15% inasampleofoverweightandobeseBrazilianadolescents. Theseindividuals,despiteexhibitingametaboliccondition similartothatofpatientswithnormalthyroidfunction,have ahigherWC, suggesting that SCH maybeassociated with excessbody weight,especiallyvisceral weight.In adoles-centswithnormal thyroidfunction, therealsoappears to beadirectrelationshipbetweenTSHandsomeofthe pri-marymarkersofIRandMetS.Thesecorrelations,although statisticallysignificant,wereweakandshouldbecarefully interpreted. Inparticular, patients with TSH inthe upper normal limit appear to have a worse metabolic profile, suggestingthatthyroid functionmaybeoneofthe deter-minantsofIRandMetSinthissample.However,theclinical significance of these findings needs to be determined in prospectivestudies.Itwillbeespeciallyimportantto per-formlarge studies examining the potential advantages of treatingobesechildrenandadolescents,targetingaTSHof approximately2.5toattenuatemetabolicrepercussions.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.OgdenCL,CarrollMD,KitBK,FlegalKM.Prevalenceofobesity andtrendsinbodymassindexamongUSchildrenand adoles-cents,1999---2010.JAMA.2012;307:483---90.
2.FloresLS,GayaAR,PetersenRD,GayaA.Trendsofunderweight, overweight,andobesityinBrazilianchildrenandadolescents. JPediatr(RioJ).2013;89:456---61.
3.WeissR,DziuraJ,BurgertTS,TamborlaneWV,TaksaliSE,Yeckel CW,etal.Obesityandthemetabolicsyndromeinchildrenand adolescents.NEnglJMed.2004;350:2362---74.
4.Godoy-MatosA,CarraroL,VieiraA,OliveiraJ,GuedesEP, Mat-tosL,etal.Treatmentofobeseadolescentswithsibutramine: arandomized,double-blind,controlledstudy.JClinEndocrinol Metab.2005;90:1460---5.
5.CookS,WeitzmanM,AuingerP,NguyenM,DietzWH.Prevalence of a metabolic syndrome phenotype inadolescents: findings fromthethirdNationalHealthandNutritionExamination Sur-vey,1988---1994.ArchPediatrAdolescMed.2003;157:821---7.
6.BrentaG.Whycaninsulinresistancebeanaturalconsequence ofthyroiddysfunction?JThyroidRes.2011;2011:152850.
7.IacobellisG,RibaudoMC,ZappaterrenoA,IannucciCV,Leonetti F.Relationshipofthyroidfunctionwithbodymassindex,leptin, insulinsensitivityandadiponectinineuthyroidobesewomen. ClinEndocrinol(Oxf).2005;62:487---91.
8.KnudsenN,LaurbergP,RasmussenLB,BülowI,PerrildH,Ovesen L,etal.Smalldifferences inthyroidfunction maybe impor-tantforbodymassindexandtheoccurrenceofobesityinthe population.JClinEndocrinolMetab.2005;90:4019---24.
10.ReinehrT, IsaA, deSousaG, DieffenbachR, AndlerW. Thy-roidhormonesand theirrelationtoweightstatus. HormRes. 2008;70:51---7.
11.ReinehrT,AndlerW.Thyroidhormonesbeforeandafterweight lossinobesity.ArchDisChild.2002;87:320---3.
12.MarrasV,CasiniMR,PiliaS,CartaD,CivolaniP,PorcuM,etal. Thyroidfunctioninobesechildrenandadolescents.HormRes Paediatr.2010;73:193---7.
13.RuhlaS,WeickertMO,ArafatAM,OsterhoffM,IskenF,Spranger J,et al.Ahighnormal TSHis associatedwiththemetabolic syndrome.ClinEndocrinol(Oxf).2010;72:696---701.
14.Taylor PN,Razvi S, PearceSH, DayanCM. Clinicalreview: a review of the clinical consequences of variation in thyroid functionwithinthereferencerange.JClinEndocrinolMetab. 2013;98:3562---71.
15.RazviS,IngoeL,KeekaG,OatesC,McMillanC,WeaverJU.The beneficialeffectofl-thyroxineoncardiovascularriskfactors, endothelialfunction,andqualityoflifeinsubclinical hypothy-roidism:randomized,crossovertrial.JClinEndocrinolMetab. 2007;92:1715---23.
16.Boggio A, Muzio F, Fiscella M, Sommariva D, Branchi A. Is thyroid-stimulatinghormonewithinthenormalreferencerange ariskfactorforatherosclerosisinwomen?InternEmergMed. 2014;9:51---7.
17.Asvold BO, Bjøro T, Vatten LJ. Associations of TSH levels withinthereferencerangewithfuturebloodpressureandlipid concentrations: 11-year follow-up of the HUNT study. Eur J Endocrinol.2013;169:73---82.
18.Ittermann T,ThammM,WallaschofskiH, RettigR, VölzkeH. Serumthyroid-stimulatinghormonelevelsareassociatedwith bloodpressureinchildrenand adolescents.JClinEndocrinol Metab.2012;97:828---34.
19.GelonezeB,RepettoEM,GelonezeSR,TambasciaMA,Ermetice MN.Thethresholdvalueforinsulinresistance(HOMA-IR)inan admixturedpopulationIRintheBrazilianMetabolicSyndrome Study.DiabetesResClinPract.2006;72:219---20.
20.GarberJR,CobinRH,GharibH,HennesseyJV,KleinI, Mechan-ick JI, et al. Clinical practice guidelines for hypothyroidism inadults:cosponsoredbytheAmericanAssociationofClinical Endocrinologists and theAmerican Thyroid Association. Thy-roid.2012;22:1200---35.
21.LaurbergP,AndersenS,CarléA,KarmisholtJ,KnudsenN, Peder-senIB.TheTSHupperreferencelimit:whereareweat?NatRev Endocrinol.2011;7:232---9.
22.Wartofsky L, Dickey RA. The evidence for a narrower thy-rotropinreferencerangeiscompelling.JClinEndocrinolMetab. 2005;90:5483---8.
23.MonzaniA,ProdamF,RapaA,MoiaS,AgarlaV,BelloneS,etal. Endocrinedisordersinchildhoodandadolescence.Natural his-toryofsubclinicalhypothyroidisminchildrenandadolescents andpotentialeffectsofreplacementtherapy:areview.EurJ Endocrinol.2012;168:R1---11.
24.ReinehrT,deSousaG,AndlerW.Hyperthyrotropinemiainobese childrenis reversibleafterweight lossand isnotrelated to lipids.JClinEndocrinolMetab.2006;91:3088---91.
25.BlüherS,MolzE, WiegandS, OttoKP,SergeyevE,Tuschy S, et al. Body mass index, waist circumference, and waist-to-heightratioaspredictorsofcardiometabolicriskinchildhood obesitydependingonpubertaldevelopment.JClinEndocrinol Metab.2013;98:3384---93.
26.AeberliI,JungA,MurerSB,WildhaberJ,Wildhaber-BrooksJ, KnöpfliBH,etal.During rapidweightlossinobesechildren, reductionsinTSHpredictimprovementsin insulinsensitivity independentofchangesinbodyweightorfat.JClinEndocrinol Metab.2010;95:5412---8.
27.Aypak C, Türedi O, Yüce A, Görpelio˘glu S. Thyroid-stimulatinghormone(TSH)levelinnutritionallyobesechildren and metabolic co-morbidity. J Pediatr Endocrinol Metab. 2013;26:703---8.
28.Radhakishun NN, van Vliet M, von Rosenstiel IA, Weijer O, BeijnenJH,BrandjesDP,etal.Increasingthyroid-stimulating hormone is associated with impaired glucosemetabolism in euthyroidobesechildrenandadolescents.JPediatrEndocrinol Metab.2013;26:531---7.
29.RoosA,BakkerSJ,LinksTP,GansRO,WolffenbuttelBH. Thy-roidfunctionisassociatedwithcomponentsofthemetabolic syndrome in euthyroid subjects. J Clin Endocrinol Metab. 2007;92:491---6.