JPediatr(RioJ).2016;92(5):436---450
www.jped.com.br
REVIEW
ARTICLE
Impact
of
health
professional
training
in
breastfeeding
on
their
knowledge,
skills,
and
hospital
practices:
a
systematic
review
夽
Patricia
Carvalho
de
Jesus
a,
Maria
Inês
Couto
de
Oliveira
b,∗,
Sandra
Costa
Fonseca
baUniversidadeFederalFluminense(UFF),InstitutodeSaúdeColetiva,ProgramadePós-Graduac¸ãoemSaúdeColetiva,Niterói,
RJ,Brazil
bUniversidadeFederalFluminense(UFF),InstitutodeSaúdeColetiva,DepartamentodeEpidemiologiaeBioestatística,Niterói,
RJ,Brazil
Received18June2015;accepted14September2015 Availableonline15February2016
KEYWORDS Breastfeeding; Healthprofessional; Training;
Knowledge;
Professionalpractice; Baby-Friendly HospitalInitiative
Abstract
Objective: Toidentifytheimpactoftraininginbreastfeedingonknowledge,skills,and profes-sionalandhospitalpractices.
Datasource: ThesystematicreviewsearchwascarriedoutthroughtheMEDLINE,Scopus,and LILACSdatabases.Reviews,studieswithqualitativemethodology,thosewithoutcontrolgroup, thoseconductedinprimarycare,withspecificpopulations,studiesthathadabeliefand/or pro-fessionalattitudeasoutcome,orthosewithfocusonthepost-dischargeperiodwereexcluded. Therewasnolimitationofperiodorlanguage.Thequalityofthestudieswasassessedbythe adaptedcriteriaofDownsandBlack.
Summaryofdata: Theliteraturesearchidentified276articles,ofwhich37wereselectedfor reading,26wereexcluded,andsixwereincludedthroughreferencesearch.Intotal,17 inter-vention articleswere included,threeofthem withgoodinternal validity.The studieswere performedbetween1992and2010incountriesfromfivecontinents;fourofthemwere con-ductedinBrazil.Thetrainingtargetpopulationswerenursingpractitioners,doctors,midwives, andhomevisitors.Manykindsoftrainingcourseswereapplied.Fiveinterventionsemployedthe theoreticalandpracticaltrainingoftheBaby-FriendlyHospitalInitiative.Allkindsoftraining coursesshowedatleastonepositiveresultonknowledge,skills,and/orprofessional/hospital practices,mostofthemwithstatisticalsignificance.
Conclusions: Trainingofhospitalhealthprofessionalshasbeeneffectiveinimproving knowl-edge,skills,andpractices.
©2016SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/ 4.0/).
夽 Pleasecitethisarticleas:deJesusPC,deOliveiraMI,FonsecaSC.Impactofhealthprofessionaltraininginbreastfeedingontheir
knowledge,skills,andhospitalpractices:asystematicreview.JPediatr(RioJ).2016;92:436---50. ∗Correspondingauthor.
E-mail:[email protected](M.I.C.deOliveira). http://dx.doi.org/10.1016/j.jped.2015.09.008
Hospitaltraininginbreastfeeding 437
PALAVRAS-CHAVE Aleitamentomaterno; Profissionaldesaúde; Capacitac¸ão;
Conhecimento; Práticaprofissional; IniciativaHospital AmigodaCrianc¸a
Repercussãodacapacitac¸ãodeprofissionaisdesaúdeemaleitamentomaternosobre
seusconhecimentos,habilidadesepráticashospitalares:umarevisãosistemática
Resumo
Objetivo: Identificararepercussãodacapacitac¸ãoemaleitamentomaternosobre conhecimen-tos,habilidadesepráticasprofissionaisehospitalares.
Fontesdosdados: A busca darevisãosistemáticafoi efetuadanasbases MedLine,Scopuse Lilacs. Foram excluídos artigosde revisão, de metodologia qualitativa, estudos semgrupo controle, conduzidosnaatenc¸ãoprimária,comclientelasespecíficas,cujosdesfechoseram crenc¸ae/ouatitudeprofissionaletrabalhoscomfoconoperíodopós-altahospitalar.Nãohouve limitac¸ão quanto ao anoou idioma,sendorealizada avaliac¸ão daqualidadedos artigospor critérioadaptadodeDowns&Black.
Síntesedosdados: Nabuscadeliteraturaforamencontrados276artigoseselecionados37para leituraintegral,sendoexcluídos26artigoseincluídos6mediantebuscadasreferências.Foram incluídos17artigosdeintervenc¸ãoetrêsapresentaramboavalidadeinterna.Osestudosforam conduzidosentre1992e2010empaísesdecincocontinentes,sendoquatronoBrasil.O prin-cipalpúblico-alvodascapacitac¸õesforamprofissionaisdeenfermagem,médicos,parteirase visitadoresdomiciliares.Oscursosdecapacitac¸ãoforamdiversos,cincointervenc¸ões empre-gandootreinamentoteórico-práticodaIniciativaHospitalAmigodaCrianc¸a.Todasasformasde capacitac¸ãoapresentaramalgumresultadopositivosobreosconhecimentos,habilidadese/ou práticasprofissionaisehospitalares,amaioriacomsignificânciaestatística.
Conclusões: Ascapacitac¸õesdeprofissionaisdesaúdequeatuamemhospitaistêmsidoefetivas emaprimorarconhecimentos,habilidadesepráticas.
©2016SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4. 0/).
Introduction
TheWorldHealthOrganization(WHO)1andtheBrazilian
Min-istryofHealth2recommendexclusivebreastfeedingforsix
monthsand breastfeedingsupplemented withother foods
until2yearsofageormore.
However, health professionals’ lack of knowledge and
skills on breastfeeding and unfavorable attitudes toward
this practice3 can negatively influence the establishment
and maintenance of breastfeeding,4 with lack of
train-ing representing one of the causes for the inefficiency
of professionalpractice.5 The health professional’sroleis
toreinterpret thescientific discourse withtheclientele.6
Therefore, it is essential to have knowledge and clinical
skills inbreastfeedingcounseling,tobeabletoguideand
assistinbreastfeedingmanagement,whennecessary.7,8
Several studies show the need for specific and
peri-odic training in promoting, protecting, and supporting
breastfeeding, aiding in the encouragement and
sup-port of breastfeeding policies and protocols in health
institutions.7---9
Highstaffturnover---aswellaslackofmotivation,
avail-able resources, and time --- are factors that hinder the
trainingofthehealthcareteam.10
A review by Fairbank et al.11 on the effectiveness of
professionaltraining topromote the onset of
breastfeed-ing found increased knowledge of the staff, but did not
identifystatisticallysignificantchangesregardingtheonset
of breastfeeding. Another review12 of interventions with
professionals,withthedurationofbreastfeedingasthe
out-come,concludedthattheevidencewasstillinsufficientand
recommendedthatstudiesreportintermediateoutcomesof
interventions,suchasprofessionalknowledgeandpractices.
The Baby-Friendly Hospital Initiative (BFHI) is a
strat-egythatstartswithawareness,training,andmobilizationof
healthcareprofessionalsworkinginhospitals with
obstet-ricbeds,aimingtoestablishrulesandroutinesfavorableto
thepracticeof breastfeeding.It waslaunchedin1990 by
theWHOandTheUnitedNationsChildren’sFund(UNICEF)
duringa meeting where the Declaration of Innocenti was
signed.13 At this meeting, global goals were proposed
and the ‘‘Ten Steps to Successful Breastfeeding’’ were
established.13
Step2oftheBFHIreferstothetrainingofstafftoacquire
thenecessaryknowledgeandskillstoimplementthe
hospi-talnormsandroutinesinbreastfeedingand,thus,theBFHI
courseisboththeoreticalandpractical.14
No reviews were found that focused on the influence
of health professionals’training in breastfeeding ontheir
knowledge and practices. Considering the importance of
professional training to improve hospital practices
aim-ing toincrease breastfeeding rates, the objective of this
systematic review was to highlight the impact of
train-inginterventions on breastfeeding in health professionals
workinginhospitalsregardingtheirprofessionalknowledge,
skills,andpractices,aswellashospitalpractices.
Methods
438 deJesusPCetal.
SystemOnline(MEDLINE),Scopus,andLatin Americanand CaribbeanHealthSciences(LILACS)databases.Thesearch was carried out in September 2014 and focused on the training of health professionals that worked in hospitals regardingbreastfeedingsupport.Thesearchstrategyusedin theMEDLINEandScopusdatabaseswas:breastfeedingand healthprofessionalsand(capacityortrainingoreducation) and(knowledge or professionalpractice) and(hospital or maternityhospital);andinLILACS:breastfeedingandhealth professionaland(trainingoreducation)and(knowledgeor skillor professionalpractice)andtheequivalentwords in Portuguese.
Thestudyinclusioncriteriawere:originalarticles repor-ting on breastfeeding training and its impact on the professionals’ knowledge, skills, practice, and/or hospi-tal practices. Qualitative methodology articles, studies lacking a comparison control group, review articles, studiescarriedoutintheprimaryhealthcarenetwork, stud-ieswhoseoutcomesexclusivelycomprisedtheprofessional’s belief and/or attitude, studies with specific populations suchaspreterminfants orHIV-positivemothers,and stud-iesfocusing onthe impact of training onthe duration of breastfeedingin the post-dischargeperiodwere excluded fromthesystematicreview.Therewasnolimitationonthe publicationyearorlanguage.
Abstract search was performed independently by two authors of this systematic review. At this phase, articles were excluded according to the study selection criteria. Incaseof discordanceregarding theabstract,theauthors optedtoreadthefulltext.
An additionalsearchwasperformed,based onthe ref-erencelistsofarticlesreadin full,toincreasesensitivity, thusidentifyingarticlesthatwerenotretrievedthroughthe electronicsearch.Afterreadingtheminfull,anew exclu-sionwascarriedoutaccordingtothesamestudyselection criteria. Disagreementswere resolved byconsensus or by consultationwithathirdreviewer.
Datawereextractedusingastandardizedformandthe final classification regarding inclusion in the review was alsoperformed independently;theresults werecompared anddisagreementsresolvedbyconsensusbetweenthetwo reviewers,withreferraltoathirdreviewerincasesof per-sistentdoubts.
Thearticleswerealsoindependentlyassessedregarding their quality, through a scoring system with a maximum scoreof20points.Theprotocolforassessingthequalitywas adaptedfromDownsandBlack,15 andconsistsof20
ques-tions:(1)Wasthehypothesis/objectiveclearlydescribed?;
(2)Werethestudyoutcomesclearlydescribedinthe
Intro-duction or Methods section?; (3) Were the characteristics
ofthepatientsincludedinthestudyclearlydescribed?;(4)
Werethe interventionsof interest clearly described?; (5)
Wasthe distributionof confoundingfactors ineach group
clearlydescribed?;(6)Werethemainfindingsofthestudy
clearlydescribed?; (7) Didthestudy provide estimates of
randomvariabilityofdataforthemainoutcomes?;(8)Are
thecharacteristicsofthelostpatientsclearlydescribed?;(9)
Werethe95%confidenceintervalsand/orp-valuesreported
for associations with major outcomes, except when the
p-valuewas<0.001?;(10)Werethesubjectsinvitedto
par-ticipateinthestudyrepresentativeofthepopulationfrom
whichtheywererecruited?;(11)Was therean attemptat
blindingsubjectssubmittedtotheintervention?;(12)Were
the statistical tests usedtoassess the significance of the
associations with the main outcome measures adequate?;
(13) Were the comparison groups maintained?; (14) Were
themainoutcomemeasuresaccurate(validandreliable)?;
(15) Were the groups to be compared obtained from the
same population?; (16) Werethe study subjects recruited
inthesameperiodoftime?;(17)Werethesubjectsinthe
intervention group randomized?; (18)Was thereadequate
adjustment for confounding factors in the analysis from
whichthemainfindingswereobtained?;(19)Werethelosses
tofollow-up takeninto account?; (20)Didthe studyhave
enoughpowertodetectasignificantclinicaleffect,inwhich
theprobabilityvalueforthedifferenceduetochanceisless
than5%?
Each question was scored with 0 (negative) or 1
(pos-itive). Considering the score achieved by each study, the
evaluateditemswereclassifiedaspoor(0---9points),
regu-lar(10---14points),orgood(15---20points).Articleswithpoor
qualitywereexcluded fromthereviewbecausetheywere
consideredtohavelowinternalvalidity.
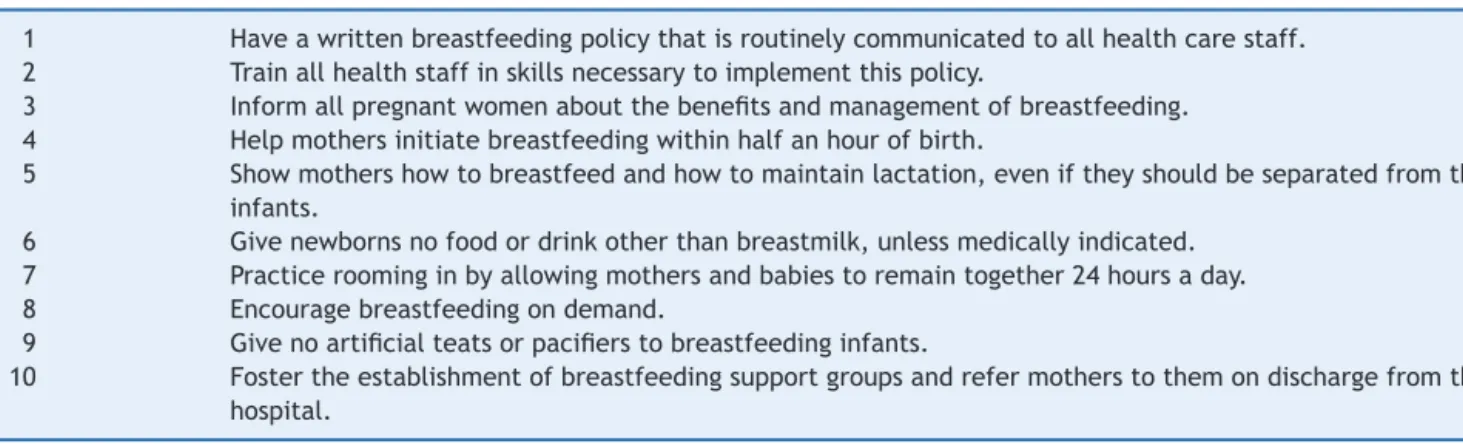
Twotableswereconstructed,accordingtotheoutcome.
Thefirstshowsarticleswhoseassessedoutcomewere
pro-fessionalknowledge,skills,and/orpractice,andthesecond
showsarticleswhoseoutcomewerehospitalpractices.Both
professionaland hospitalpracticesin generalwere
evalu-atedusingtheTenStepstoSuccessfulBreastfeedingasthe
parameter(Table1).Thearticlesinvestigatingthetwo
out-comesareshowninTables2and3.
Thecolumnsofthetablesshow:thearticle’sfirstauthor,
year of publication, the place and year the study was
performed;qualityscoreobtained;thestudysetting,
pop-ulation, and sample size (or the number of participants
when the article does not specify the sample size); the
study design (studies in which therewasa randomization
processwereconsideredrandomizedcontrolledtrials;
stud-ieswithexternal controlgroupbutwithoutrandomization
wereconsideredquasi-experimentalstudies,andthosewith
internalcontrolgroupwereconsidered‘‘beforeandafter’’
interventions);theexposure;theassessedoutcomeandthe
evaluationmethod;and,finally,theobservedresults.Each
lineshowsanarticle,whichareshownbyyearofthestudy
(Tables2and3).
Theeffectof trainingwiththe TenStepstoSuccessful
Breastfeeding14 onthe hospitalpracticeswassummarized
inthelastparagraphoftheresults,consideringtheeffect
aspositivewhenthechangesweresignificantorwhen100%
ofcompliancewiththeStepwasachieved.
Results
Hospitaltraininginbreastfeeding 439
Table1 Tenstepstosuccessfulbreastfeeding.
1 Haveawrittenbreastfeedingpolicythatisroutinelycommunicatedtoallhealthcarestaff. 2 Trainallhealthstaffinskillsnecessarytoimplementthispolicy.
3 Informallpregnantwomenaboutthebenefitsandmanagementofbreastfeeding. 4 Helpmothersinitiatebreastfeedingwithinhalfanhourofbirth.
5 Showmothershowtobreastfeedandhowtomaintainlactation,eveniftheyshouldbeseparatedfromtheir infants.
6 Givenewbornsnofoodordrinkotherthanbreastmilk,unlessmedicallyindicated. 7 Practiceroominginbyallowingmothersandbabiestoremaintogether24hoursaday. 8 Encouragebreastfeedingondemand.
9 Givenoartificialteatsorpacifierstobreastfeedinginfants.
10 Fostertheestablishmentofbreastfeedingsupportgroupsandrefermotherstothemondischargefromthe hospital.
thestudiesreadinfull,totaling17articlesincludedinthe review(Fig.1).
Of the 17 articles, nine addressed professional
knowledge,7,16---23 two professional skills,7,24 three
profes-sionalpractices,9,20,21andninehospitalpractices.9,16,19,25---30
Thestudiesaddressedinterventionsthatwereclassified
asrandomizedcontrolledtrials(3),7,16,26quasi-experimental
studies (5),9,19,20,23,24 and the ‘‘before and after’’ type,
which used an internal control group (9)17,18,21,22,25,27---30
(Tables2and3).Resultsrelatedtobreastfeedingduration
afterhospitaldischargewerenotincludedinthisreview.
Thestudieswerecarriedoutbetween1992and2010in
several countries: four in Brazil,7,16,26,29 one in Mexico,18
one in the United States,23 one in Canada,9 two in the
UnitedKingdom,22,24 twoinFrance,27,28 onein Italy,19 two
inCroatia,21,30 oneinNigeria,20 onein India,25 andonein
Australia.17 The setting of thesestudies wasvaried: large
andsmallhospitals,of lowand highrisk, publicand
phil-anthropicinstitutions,in urban andruralareas. The main
target audience of these courses was nursing
profession-als/staff,physicians,andhomevisitors.
Thetrainingcourseswerediverse:theoreticaland
prac-ticalBFHI training14 lasting 18---24h was employedin five
studies,19---21,29,30 while two22,24 used a breastfeeding
man-agementcourse,31andtheWHOcounseling32courselasting
40hwasusedinonestudy.7
Two studies used a Wellstart-SLC (Santos Lactation
Center)33courselasting133h,16,26twoapplied3daycourses
onthebenefitsandmanagementofbreastfeeding,27,28one
appliedan 18-h theoretical---practical course on maternal
Medline 116 results
Lilacs 43 results Scopus
117 results
276 articles
203 articles
73 articles duplicated among the data bases
166 articles excluded after reading the title/abstract, as they did not meet the selection criteria
37 abstracts selected for full text reading
Excluded articles:
- Score <10 at quality assessment (1) - Qualitative studies (2)
- Other outcomes, such as start and duration of BF and EBF (7) - Studies without coupled intervention (9)
- Case report/editorial (4)
- Study population: students/primary care professionals (3)
Articles included through reference search (6)
17 articles included in the review
440
de
Jesus
PC
et
al.
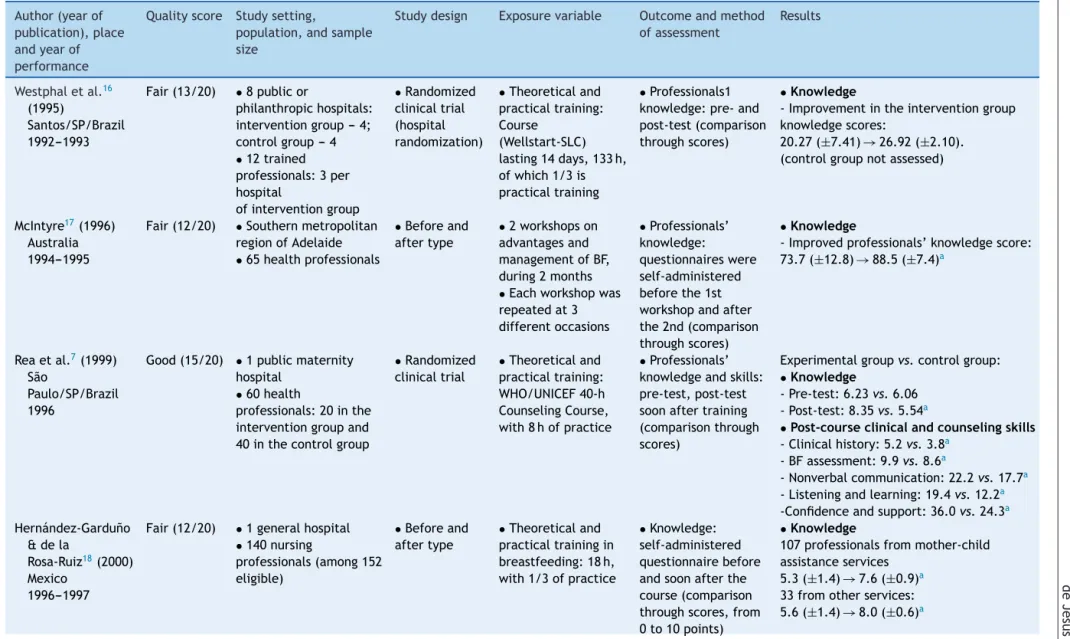
Table2 Studiesontheimpactoftrainingofhealthprofessionalsontheirknowledge,skills,andpractices. Author(yearof
publication),place andyearof performance
Qualityscore Studysetting,
population,andsample size
Studydesign Exposurevariable Outcomeandmethod ofassessment
Results
Westphaletal.16
(1995)
Santos/SP/Brazil 1992---1993
Fair(13/20) •8publicor
philanthropichospitals: interventiongroup---4; controlgroup---4
•12trained professionals:3per hospital
ofinterventiongroup
•Randomized clinicaltrial (hospital randomization)
•Theoreticaland practicaltraining: Course
(Wellstart-SLC) lasting14days,133h, ofwhich1/3is practicaltraining
•Professionals1 knowledge:pre-and post-test(comparison throughscores)
•Knowledge
-Improvementintheinterventiongroup knowledgescores:
20.27(±7.41)→26.92(±2.10). (controlgroupnotassessed)
McIntyre17(1996)
Australia 1994---1995
Fair(12/20) •Southernmetropolitan regionofAdelaide
•65healthprofessionals
•Beforeand aftertype
•2workshopson advantagesand managementofBF, during2months
•Eachworkshopwas repeatedat3 differentoccasions
•Professionals’ knowledge: questionnaireswere self-administered beforethe1st workshopandafter the2nd(comparison throughscores)
•Knowledge
-Improvedprofessionals’knowledgescore: 73.7(±12.8)→88.5(±7.4)a
Reaetal.7(1999)
São
Paulo/SP/Brazil 1996
Good(15/20) •1publicmaternity hospital
•60health
professionals:20inthe interventiongroupand 40inthecontrolgroup
•Randomized clinicaltrial
•Theoreticaland practicaltraining: WHO/UNICEF40-h CounselingCourse, with8hofpractice
•Professionals’ knowledgeandskills: pre-test,post-test soonaftertraining (comparisonthrough scores)
Experimentalgroupvs.controlgroup:
•Knowledge
-Pre-test:6.23vs.6.06 -Post-test:8.35vs.5.54a
•Post-courseclinicalandcounselingskills
-Clinicalhistory:5.2vs.3.8a
-BFassessment:9.9vs.8.6a
-Nonverbalcommunication:22.2vs.17.7a
-Listeningandlearning:19.4vs.12.2a
-Confidenceandsupport:36.0vs.24.3a
Hernández-Gardu˜no &dela
Rosa-Ruiz18(2000)
Mexico 1996---1997
Fair(12/20) •1generalhospital
•140nursing
professionals(among152 eligible)
•Beforeand aftertype
•Theoreticaland practicaltrainingin breastfeeding:18h, with1/3ofpractice
•Knowledge: self-administered questionnairebefore andsoonafterthe course(comparison throughscores,from 0to10points)
•Knowledge
107professionalsfrommother-child assistanceservices
5.3(±1.4)→7.6(±0.9)a
Hospital
training
in
breastfeeding
441
Table2 (Continued) Author(yearof publication),place andyearof performance
Qualityscore Studysetting,
population,andsample size
Studydesign Exposurevariable Outcomeandmethod ofassessment
Results
Cattaneo& Buzzetti19(2001)
Italy 1996---1998
Good(16/20) •8eligiblehospitals Group1:4hospitalswith 377trainedprofessionals (of536eligible):from 10/1996to
02/1997
Group2:3hospitals(1 loss)with194trained professionals(of237 eligible)from10/1997to 02/1998
•2669mother-child binomials(with L>2000g,withno admissionattheICU)
• Quasi-experimental (withbefore andafter component)
•Multipliertraining in24-hcourses (18h+2h
counseling+4clinical practice)thattrained groups1and2 throughthe18-hBFHI course
•Professionals’ knowledge: self-administered questionnaireat baseline(06/1996) andaftereach trainingcourse (comparisonthrough scores)
•Knowledge
Baseline→post-trainingofgroup 1→post-trainingofgroup2: -Group1:0.41→0.66→0.72 -Group2:0.53→0.53→0.75 (p-valuenotmentioned)
Owoajeetal.20
(2002) Nigeria 1997
Fair(13/20) •1tertiaryhospital,2 secondaryhospitals,and 13basicunitswith obstetriccare)
•298nurses(of305 eligibleprofessionals) workingforatleast6 months:113trainedand 185inthecontrolgroup
• Quasi-experimental (withprevious intervention)
•Theoreticaland practicaltraining: WHO/UNICEFBFHI 18-hcourse
•Knowledgeand professional practices: self-administered questionnaire (comparisonof knowledgeonEBF throughproportions andscores(0---20 points);about problemsand managementof problemsin breastfeeding throughproportions
•Knowledge
Experimentalvs.control:Onthe advantagesofEBF
-knowledgescoresof(11items):11.9 (±1.84)vs.10.7(±2.4)
-differenceonlyfordiarrheareduction: 97.3%vs.87.0%a
2.OncausesandmanagementofBF problems.
-effectofpre-dairy,asorenipples,a
insufficientmilk,abreastengorgement,a
mastitis,amanagementofneonatal
jaundice
•Professionalpractices
Experimentalvs.control -Step4(BFstart): 91.2%vs.81.6%a
-Step5(expressionbyhand):75.2%vs. 65.4%
-Step6(notusingpre-dairy):73.5%vs. 54.6%a
442
de
Jesus
PC
et
al.
Table2 (Continued) Author(yearof publication),place andyearof performance
Qualityscore Studysetting,
population,andsample size
Studydesign Exposurevariable Outcomeandmethod ofassessment
Results
Martens9(2000)
Canada 1998
Fair(13/20) •2smallhospitalsin ruralareas.
•InterventionGroup:1 hospital,15of24eligible nursingprofessionals
•ControlGroup:1 hospital,16of19eligible nursingprofessionals
•Breastfedbabies:26in theinterventionhospital and23inthecontrol hospital
• Quasi-experimental
•Traininglasting 1.5hwithnurses duringworkhours andoptionaltutorial
•Focusonknowledge ofthemanagement ofBFandBFHIpolicy
•AdherencetoBFHI principles:
Self-administered questionnairebefore theinterventionand after8months (comparisonof proportions)
•Professionalpractices
Interventionhospital:
-Step1:Informationonnorms:15%→87%a
-Step3:discussbenefitsofBF:60%→73% -Step4:offerhelptostartBFwithinthe 1sthour:75%→87%
-Step5:recordlatching/position: 45%→67%
-Step5:guideexpressionbyhand: 40%→73%a
-Step6:doesnotencourageuseof supplements:30%→67%a
-Step8:doesnotlimitBFondemand: 5%→7%
-Step9:doesnotrecommenduseof bottle:30%→67%a
-Step10:guidespost-dischargeBFsupport: 5%→67%a
Moranetal.24
(2000)
UnitedKingdom 1999
Fair(10/20) •4hospitals: 3experimentaland1 control
•13obstetricnurses evaluatedbeforethe courseand15afterthe course
• Quasi-experimental
•Trainingof WHO/UNICEF managementin maternalBF:20h
•Professionals’skills: analyzedthrough pre-validatedBeSST (Breastfeeding SupportSkillsTool) toolusingvideoclips. Questionnaireswere self-administered (comparisonof scores)
•Skills
Experimentalvs.control:
-SkillscoresinthemanagementofBF support:
Hospital
training
in
breastfeeding
443
Table2 (Continued) Author(yearof publication),place andyearof performance
Qualityscore Studysetting,
population,andsample size
Studydesign Exposurevariable Outcomeandmethod ofassessment
Results
Zakarija-Grkovi´c& Burmaz21(2010)
Croatia 2007---2009
Fair(12/20) •5largehospitals.
•308professionals trainedof424eligible (72.6%)
•Beforeand aftertype
•Theoreticaland practicaltraining: WHO/UNICEFBFHI course:20h
•Professional knowledgeand practices:
Questionnaireswere self-administered beforethetraining (n=223)andafter 3months(n=213) (comparisonofhit ratios)
•Knowledge
DefinitionofEBF,atimeoffirstBF,aroleof
prolactin,asignsofinadequatepositioning
forBF,ahospitalsupportpractices,asignsof
inadequatelatching,barrierstoBF.
•Professionalpractices
-RecommendationondurationofEBFaand
BF,amanagementofinsufficientmilk
productionaandmastitis,aadherenceto
ICMBMS,aBFrecommendationafter
C-section,BFmanagementwhenthebaby refusestosuck
Wissettetal.22
(2000)
UnitedKingdom Yearnot mentioned
Fair(12/20) •1hospital
•22professionals: nursesandhomevisitors (pre-test:22and post-test:18)
•Beforeand aftertype
•Trainingin WHO/UNICEF Maternal Breastfeeding management:20h
•Knowledge: self-administered questionnairebefore and8weeksafterthe course(comparison throughmedian scores,maximum:30)
•Knowledge
-Medianoverallscore: 17→24a
Bernaixetal.23
(2010) UnitedStates Yearnot mentioned
Fair(13/20) •12hospitals
•InterventionGroup:9 hospitals,203nurses(of 297eligibleones)
•ControlGroup:4 hospitals(with1loss), 34nurses(of64eligible)
• Quasi-experimental
•Tenmodulesof self-teaching materialtobe studiedfor4---6weeks beforethepost-test
•Knowledge: Self-administered questionnairewith 50items(comparison ofproportionsand meanscores)
•Knowledge
Experimentalvs.control: 64%→78%avs.61%→62%
31.9→39.2avs.30.5→31.7
BF,breastfeeding;EBF,exclusivebreastfeeding;BFHI,BabyFriendlyHospitalInitiative;WHO/UNICEF,WorldHealthOrganization/TheUnitedNationsChildren’sFund;ARF,acuterespiratory failure;ICMBMS,TheInternationalCodeofMarketingofBreastmilkSubstitutes.
444
de
Jesus
PC
et
al.
Table3 Studiesontheimpactoftrainingofhealthprofessionalsonhospitalpractices.
Author(yearof publication),place andyearof
performance,quality score
Qualityscore Studysetting,population, andsamplesize
Study design
Exposure variable
Outcomeandmethod ofassessment
Resultsonhospitalpractices
Westphaletal.16
(1995)
Santos/SP/Brazil 1992---1993
Fair(13/20) •8publicand
philanthropichospitals: interventiongroup---4; controlgroup---4
•12professionalstrained: 3perhospitalintervention
•Randomized clinicaltrial (hospital randomization)
•Theoreticaland practicaltraining: Course
(Wellstart-SLC) lasting14 days,133h,with 1/3practical training
•AdherencetoBFHISteps 1---10:interviewswith managers,health professionals,pregnant women,andmothers beforeandsixmonths aftertraining
•Differencesininstitutionalscoresby hospitalpairs(experimentalorcontrol): Pair1:0.6vs.0.9;Pair2:1.6vs.−0.7 Pair3:1.9vs.0.2;Pair4:0.5vs.0.2
•Institutionalchanges:significant advanceinSteps1,2,10(p-valuenot stated)
Prasad&Costello25
(1995) India 1992---1993
Fair(13/20) •1publichospitalinthe countryside
•HospitalAdministrators, 8physicians,1wardsister, 9nurses
•Mother-childbinomials withnormaldeliveryand healthybabies(172at baseline,195soonafter theintervention,and101 sixmonthslater)
•Beforeand aftertype(with comparison between exposedand non-exposedsix months post-intervention)
•≥5individualor groupsessionswith healtheducation doctorsonSteps4 and6
•Changesinhospital practicesrelatedtoSteps 4and6:Mothers interviewedathometwo weeksafterdelivery(at baseline,soonafterthe interventionandsix monthspost-intervention)
Baseline→soonafterthe intervention→6months post-intervention
Mothersexposedtohealtheducation: 0%→100%→36%
-Step4:BFwithinthe1sthouroflife: 3%→60%→14%
-Step6:useofsupplements: 96%→43%→77%
(bothsignificantadvances,butp-value isnotmentioned)
Sixmonthspost-intervention: -Step6:useofsupplements: 42%(ofexposed,n=36)vs.97%(of non-exposed,n=65)a
Taddeietal.26(2000)
Santos/SP 1992---1993
Fair(14/20) •8publicorphilanthropic hospitals:intervention group---4;controlgroup ---4
•12trainedprofessionals: 3perinterventionhospital
•Mother-childbinomials: 494of609eligible (pre-training)and469of 555eligible(post-training)
•Randomized clinicaltrial (hospital randomization)
•Theoreticaland practicaltraining: 14-day,133-h course (Wellstart-SLC course),with1/3 practice
•Changesinhospital practicesregardingSteps 4,5,and7:interviewto mothersduringhome visits(oneandsixmonths afterdelivery)
•Before/after,exposedvs.
non-exposed:
-Step4:BFinthedeliveryroom: 2%→23%a×2%→8%a
-BFwithinthefirst6h: 41%→53%a ×48%→50%
-Step5:BFsupportatthehospital: 48%→64%avs.58%→61%
-Step5:BFsupportatthehospital: 29%→49%avs.35%→36%
Hospital
training
in
breastfeeding
445
Table3 (Continued)
Author(yearof publication),place andyearof
performance,quality score
Qualityscore Studysetting,population, andsamplesize
Study design
Exposure variable
Outcomeandmethod ofassessment
Resultsonhospitalpractices
Cattaneo&Buzzetti19
(2001) Italy 1996---1998
Good(16/20) •8eligiblehospitals Group1:4hospitalswith 377trainedprofessionals (of536eligible)from 10/1996to02/1997 Group2:3hospitals(1 loss)with194trained professionals(of237 eligible)from10/1997to 02/1998
•2669Mother-child binomialswith
BW>2000g,withoutICU admission
• Quasi-experimental (withbeforeand after
component)
•Multipliertraining in24-hcourses (18h+2h counseling+4 clinicalpractice) thattrainedgroups 1and2usingthe BFHI18-hcourse
•AdherenceBFHITen Steps:Self-administered questionnaireby professionals(steps1and 2),interviewtomothers preandpost-evaluation (Steps4---10)
Baseline→post-training
•Before/after--- overallresult: -MeanadherencetotheSteps: 2.4→7.7steps(p-valuenotmentioned)
•Before/after--- group1andgroup2: -EBFatdischarge:41%→77%and 23%→72%(p-valuenotmentioned) -Step4:BFwithinthe1sthour: 12%→22%aand37%→60%a
-Step5:latching/positioning: 67%→88%aand77%→93%a
-Step5:expressionbyhand: 60%→75%aand43%→72%a
-Step6:useofsupplements: 35%→17%aand8%→8%
-Step7:roomingin: 72%→89%aand36%→77%a
-Step8:BFondemand: 83%→97%aand97%→99%
-Step9:useofbottle: 58%→14%aand70%→26%a
-Step9:useofpacifier: 56%→19%aand63%→52%a
•LessadvancementinSteps1,2,and 10(p-valuenotmentioned)
Durandetal.27(2003)
France 1997---2000
Fair(11/20) •1tertiarymaternity hospital
•All73professionalsfrom thestaff
•Mother-childbinomials withoutICUadmission:50 beforethetraining programand50after (with71.4%ofresponse rate)
•Beforeand aftertype
•Three-day theoreticaland practicaltraining onthebenefitsand managementof breastfeeding (10professionals perclass)from 1998to2000
•Changesinhospital practicesrelatedtoSteps 4---7,9,10:assessmentof newborns’recordsand self-administered questionnaire,givento mothersatthetimeof hospitaldischarge
•Accordingtomedicalrecord: -Step4:BFwithinthe1sthour: 7.9%→21%
-Step6:useofsupplements: 82%→63%
-Step7:mother-childseparation>4h: 52%→13%a
-Step9:formulaonlyincup: 0%→13.1%a
-Step9:useofbottle: 82%→26%a
-EBFatdischarge:14%→28%
•Accordingtothequestionnaire: -Step5:teachpositioningfor breastfeeding:41.7%→69.2%a
-Step10:post-dischargesupport resources:
446
de
Jesus
PC
et
al.
Table3 (Continued)
Author(yearof publication),place andyearof
performance,quality score
Qualityscore Studysetting,population, andsamplesize
Study design
Exposure variable
Outcomeandmethod ofassessment
Resultsonhospitalpractices
Labarereetal.28
(2003) France 1997---2000
Fair(14/20) •1tertiarymaternity
•All73professionalsof thestaff
•Mother-childbinomials withoutICUadmission: 323(pre-training)and324 (post-training)
•Beforeand aftertype
•Three-day theoreticaland practicaltraining onbenefitsand managementof breastfeeding (10professionals perclass) from1998to2000
•Changesinhospital practicesregardingSteps 4---7,and9:assessmentof maternalmedicalrecords beforeandaftertraining retrospectivelybynurse notinvolvedinassistance
EBFatdischarge:15.8%→35.2%a
-Step4:BFwithinthe1sthouroflife: 9.2%→16.9%a
-Step6:useofsupplements: 77.6%→54.0%a
-Step7:roomingin: 56.6%→72.6%a
-Step9:
formulainthecup:0.4%→23.8%a
useofbottle:77.2%→14.1%a
Martens9(2000)
Canada 1998
Fair(13/20) 2smallhospitalsinrural areas
•InterventionGroup:1 hospital,15of24eligible nursingprofessionals
•ControlGroup:1 hospital,16of19eligible nursingprofessionals
•Breastfedbabies:26in theinterventionhospital and23inthecontrol
• Quasi-experimental
•1.5-htraining withnursesduring working
hours+optional tutorial
•Focuson knowledgeofBF managementand BFHIpolicy
•AdherencetoBFHIand Steps1,2,6,7,9,and10 bythehospital:
Self-administered questionnaireby professionalsbeforethe interventionand8months after.
•EBFduringhospitalstay: assessmentofnewborn’s medicalrecord
(intervention:13preand 13post;control:14pre and9post)
•Accordingtothequestionnaire: Interventionhospital:
-Step1:writtennorm:40%→87%a
-Step2:skillsinBFmanagement: 35%→60%
-Step6:non-useofsupplement: 45%→87%a
-Step7:roomingin:90%→100% -Step9:non-useofbottle: 30%→67%a
-Step9:non-useofpacifier: 50%→67%
-Step10:encouragesupportgroups: 5%→47%a
•Accordingtomedicalrecords: experimentalvs.control-Adherenceto BFHI:
24.4%→31.9%a×20.2%→22.5%
-EBFduringhospitalstay: 31%→54%a×43%→0%a
Coutinhoetal.29
(2005) Pernambuco 1998(previous cohort)and2001
Fair(13/20) •2hospitalsfromSUS
•42professionalstrained (90%ofmidwivesand nurseaids)
•334mother-child binomialsof364eligible ones(2001)comparedto 364(1998).Urbanarea, singlebirth,withBW
≥2500g,healthy
•Beforeand aftertype (historical control)
•Theoreticaland practical training:18-h WHO/UNICEF-BFHI course+2hof breastfeeding counselingand educational material
•AdherencetoSteps4to 9ofBFHI:interviewwith mothersinthefirst48h and10daysafterdelivery.
historicalcontrol→experimentalgroup -Step4:
Skin-to-skincontact:25.8%→37.2%a
HelpwithBFatbirth:5.8%→6.0% -Step5:latching/positioning: 9.6%→21.0%a
-Step6:EBFwithinthe1st48h: 21.2%→70.0%a
-Step9:useofpacifier: 47.2%→24.3%a
Hospital
training
in
breastfeeding
447
Table3 (Continued)
Author(yearof publication),place andyearof
performance,quality score
Qualityscore Studysetting,population, andsamplesize
Study design
Exposure variable
Outcomeandmethod ofassessment
Resultsonhospitalpractices
Zakarija-Grkovi´c etal.30(2012)
Croatia 2008--- 2010
Good(16/20) •1tertiaryhospital
•Trained80%ofthe271 staffprofessionals
•Mother-childbinomials (388pre-trainingand385 post)withBW>2500g, withoutICUadmission, singlebirths(interviewed 94.2%ofeligible)
•Beforeand aftertype
•Theoreticaland practicaltraining: 20-h
WHO/UNICEF-BFHI course:oneclassin May2008and anotherinFebruary 2009
•AdherencetoSteps3to 9ofBFHI:assessmentof newborn’smedicalrecord; interviewwithmothers preandpost-training
•Accordingtothemedicalrecord:
-EBFwithin48h:6.0%→11.7%a
•Accordingtotheinterviews:
-Step3:recommendationsonchild feeding:10.8%→9.9%
-Step4:heldthebabyatthe1st contactfor>60min:0.8%→3.2%a
-Step4:babysuckedatthe1st contact:8.6%→4.2%
-Step5:helpwithlatching/positioning: 70.3%→69.0%
-Step5:wasshownexpressionbyhand: 44.1%→44.8%
-Step6:useofsupplements: 81.1%→79.4%
-Step7:roomingin: 0.3%→5.1%a
-Step8:BFondemand: 21.1→29.3%a
-Step8:durationondemand: 17.5%→28.6%a
-Step9:useofbottle:79.0%→77.8% -Step9:useofpacifier:0.3%→0%
BF,breastfeeding;EBF,exclusivebreastfeeding;BFHIBaby-FriendlyHospitalInitiative;BW,birthweight.
448 deJesusPCetal.
breastfeeding,18 onestudyappliedanightworkshop,17one
useda1.5-h trainingcomplementedby tutorialmaterial,9
oneusedmaterialforself-learning,23 andonestudyuseda
methodologycomprisingfivediscussionsessionswitheach
professional.25
Theoutcomedefinedbyninestudieswasthe
profession-als’ knowledge of breastfeeding,two studies investigated
thecapacityofprofessionalsincounselingandmanagement
ofbreastfeeding,threeinvestigatedprofessionalpractice,
andnineinvestigatedhospitalpractices,usuallyregarding
adherencetotheBFHIsteps.
Asfortheevaluationmethod,twelvestudiesevaluated
theeffectoftrainingthroughinterviewsor questionnaires
that were self-administered by health professionals, six
evaluated through an interview or a questionnaire that
was self-administered by the mothers, one reported the
observation of the maternity areas, and three performed
a retrospective evaluation throughthe analysis of
mater-naland/orneonatalmedicalrecords.Regardingthetypeof
analysis,most studies performed only comparative
analy-sesusingstatisticalsignificancetests7,9,16---18,20---23,25---27,29and
threeusedmultiplelogisticregressionanalysis.19,28,30
Regarding the quality assessment, three studies were
classifiedashavinggoodinternalvalidity,7,19,30 whereas14
wereclassifiedasfair.9,16---18,20---29
In the nine studies that investigated knowledge, the
intervention showed positive results. Five studies
mea-suredgain of knowledge through general scores, andone
by specifying the factors that achieved improvement. In
twostudies,21,24theprofessionalsweretrainedthroughthe
theoretical and practical training of BFHI14 with a
dura-tion of 20h, one with a duration of 18h,20 one through
the WHO counseling course32 lasting 40h,7 one
interven-tion trained multipliers using the Wellstart-SLC16 133-h
course,33 one applied the 18-h theoretical and practical
courseonbreastfeeding,18onestudyusedworkshopsapplied
during the night shift,17 and one provided material for
self-learning.23Asuperioreffectwasnotidentifiedin
inter-ventionswithlongerduration.
Only two studies investigated the effect of
train-ingthroughbreastfeeding counseling31 andmanagement32
coursesontheprofessionalskills, withonestudy
discrim-inating the gains in listening and learning, and building
confidence and giving support,7 and another
demon-strating the achieved advances through mean scores.24
Threestudieshadprofessionalpracticesasoutcome,9,20,21
with gains being observed only in part of the practices
(Table2).Nine studies9,16,19,25---30 evaluatedthe changesin
hospital practices, obtaining advances in most of them
(Table3).
Asfortheresultsoftrainingonhospitalchangesrelated
tothe TenSteps,14 theobject ofninestudies, Step3 was
the least assessed, by only two investigations, with no
effect.16,30 Steps 1, 2, and 8 were also scarcely
investi-gated, by only three studies,9,16,19 with positive changes
being achieved in two-thirds of interventions for Steps 1
and 8 and in one-third for Step 2. Step 10, assessed in
fourinterventions,9,16,19,27showedadvancesinthree.Step5,
assessedinsixstudies,16,19,27,29,30 reachedpositivechanges
intwo-thirdsoftheinterventions.Thetraininghadapositive
effectonfiveoftheseveninterventionsthatassessedStep
79,16,19,26---28,30andStep9.9,16,19,27---30Steps416,19,20,25,27---30and
69,16,19,25,27---30werethemostoftenassessed,ineightstudies
each,showingfavorablechangesin75%(Step4)and62.5%
(Step6)oftheinterventions(Table3).
Discussion
Thestudiesincludedinthisreviewshowedpositiveeffects of trainingonthe assessedoutcomes:professional knowl-edge,skills,andpractices,aswellashospitalpractices.
The studies were carried out in different contexts, in developed and developing countries on five continents (America,Europe,Africa,Asia,andOceania).Thisdiversity seemstoindicatethatindiversescenarios,thecoursesused wereatleastpartiallyeffective,despiteeconomic,ethnic, andculturaldifferences.
Alltrainingmethodsemployed,regardlessofthemodel, duration, and target audience, showed increase in the knowledgeandskillsofhealthprofessionalsin breastfeed-ing,withnodose-responseeffectobservedinthissystematic review for the number of class-hours and the obtained effect.Benefitsforprofessionalandhospitalpracticeswere also observed; however, the interventions did not always achieve changes regarding the ‘‘Ten Steps to Successful Breastfeeding’’.
Steps1---3,8,and10weretheleastinvestigated.Among them, Step 2 (train the entire health staff) and Step 3 (inform pregnant women) showed fewer positive results. Possibly,thelowerperformanceinStep2isduetotraining programsthatdidnotincludeallprofessionalcategories,in additiontostaffturnover,whichimpairsthepermanenceof trainedstaff.34
Asfor Step 3,the prenatalclinic is veryoften located
outside the hospital complex, and the professionals that
provide prenatal care are not the same asthose working
in the maternity hospital. This hinders their involvement
with the BFHI and the investigation of adherence to this
Step.35 It is worth mentioning the importance of
provid-inginformationtopregnantwomenaboutthebenefitsand
managementofbreastfeeding,asmostwomendefinetheir
intentiontobreastfeedduringpregnancy,36whichinfluences
theonsetand durationofbreastfeeding.37 Inastudy that
nationallyre-evaluatedadherencetotheTenStepsin 167
Brazilian BFHI accredited between 1992 and2000, Araujo
andSchmitz10alsofoundloweradherencetoSteps2and3.
Step1 (written norm) and Step 8 (stimulus to
breast-feedingondemand)obtainedpositiveresultsintwo-thirds
oftheinterventions, indicatingthatthetrainingprograms
maybeusefulforthedisclosingoftheinstitution’s
breast-feedingpolicyandfortheencouragementofbreastfeeding
ondemand.InBrazil,in SaoPaulo38 andRiodeJaneiro,35
little restrictionwas observed regarding thefree interval
between feedingsin publicandprivatehospitals, showing
goodadherencetothisprocedure.
The training alsoshowed to be effective in promoting
improvements in the practice of Step 10 (post-discharge
support) inthree-quartersofthe interventions,whichis a
relevantresult,consideringthedifficultiesfoundincarrying
outthisstepindifferentBrazilianscenarios.29,35
Steps4---7, and9, which arebasically hospital-related,
were more often investigated; the training programs
Hospitaltraininginbreastfeeding 449
(helpinitiatepostpartumbreastfeeding),oneofthemajor
barriers to breastfeeding at birth has been cesarean
delivery,39 whichis on therise in the Brazilian context;40
itisimportantthatprofessionalsareabletostimulate
skin-to-skincontactandearlysuctioneveninbabiesbornthrough
C-section.
Regarding Step5 (managementofbreastfeeding),
ade-quatemanagement of breastfeeding depends not only on
theoreticaltraining,butalsotheacquisitionofskillsbythe
healthprofessionalthatassistsmothers.Mostofthetraining
programsstudied inthisreviewwereboththeoreticaland
practical,whichmayhavecontributedtothepositiveresults
achievedby75%oftheinterventions.Advancesin62.5%of
theinterventionsregardingtheStep6(notofferthe
new-bornotherfoodsordrinksratherthanbreastmilk)suggest
that, despite its difficult adherence due tothe pressures
ofinfantformulaindustrymarketing,hospitalroutineshave
advancedsignificantly.10,35,41
The positive results observed in more than70% of the
studiesinvestigatingStep7(roomingin)indicatesevolution
inthestructureandroutineofhospitals,becauseroomingin
dependsnotonlyonprofessionaltraining.26RegardingStep9
(notusingartificialnipplesorpacifiers),theuseofpacifiers
andbottlesmaypreventtheadequatedynamicofsucking
thenipple-areolaregionandreducethefrequencyof
feed-ingsand,thus, thereductionobservedin theuseofthese
artifactsinmorethan70%ofthestudiesthatinvestigated
themisextremelybeneficial.
Astudy conductedin theUnitedStates42 demonstrated
thatSteps4,6,and9wereassociatedwithlongerdurationof
breastfeedingandthatmothersexposedtoatleastsix
hospi-talpracticesrecommendedbytheBFHIhada13-foldhigher
chanceofmaintainingbreastfeeding,comparedtomothers
whodid not have contact withany of the practices. The
observeddose-responseeffectindicatestheimportanceof
trainingprogramsaimedattargetaudiences,suchas
health-careprofessionalsfromvariousprofessionalcategoriesand
working in the different areas assisting pregnant women,
mothers, and babies,so that hospital practices coalesce,
resultinginasynergisticeffectonthedurationof
breast-feeding.
Regardingthelimitationsfoundinthissystematicreview,
theauthorsemphasizethedifferencesinthetraining
pro-gramsusedindifferentstudiesregardingtheduration,type,
and target audience, making it difficult to identify the
mosteffectivemethods,duration,andcontenttogenerate
changes in knowledge, skills, and professional and
hospi-talpractices.Thelack ofahomogeneousmethodofstudy
analysis,whichwouldfacilitatethecomparisonof results,
hindered the calculation of summary measures by
meta-analysis.
Another limitation found was the absence of a
homo-geneousanalysis methodamongthe studies, which would
facilitate comparison of the results. The studies had
different epidemiological designs, and the absence of
experimental studies indicates a higher risk of bias and
uncontrolled confoundingvariables.The evaluationof the
articles through the quality score showed fair quality in
mostarticles,butonlythreeshowedgoodinternalvalidity.
Theretrospectivedatacollection(fromrecords)wasalsoa
limitingfactorinsomestudies,27,28 causedbythe
possibil-ityof informationbiasduetoerror or theabsencein the
datarecording.Moststudiesdidnotmentionthe
represen-tativenessofthesample thatwasselectedandsubmitted
toevaluation.Mostpoorlysummarizedanddescribedtheir
results,hinderingthepresentation ofresultinterpretation
anduniformity.
Theshortperiodbetweeninterventionsandevaluations
usedinmoststudiesdidnotallowverifyingwhetherchanges
inprofessionalknowledge,skills,andpractices,aswell as
inhospitalpractices,canpersistinthelongtermafterthe
interventions.21,30Factorssuchasstaffturnoverandpolicy
changescouldinterferewiththeresultsofevaluations
car-riedoutafterlongerpost-trainingintervals.Tomaintainthe
impactofthesetrainingprograms,itisnecessarytoreapply
themperiodically.7
Informationonthecontextoftheinterventions,onthe
availabledataforevaluation,andonthecost-effectiveness
of the employedtraining programswas sparse or absent,
whichreduces the possibilityof reproducing the research
along similar lines tothose undertaken in other settings.
Thisinformationcouldbeofgreatvalueforhealthfacility
managersandforfuturestudies.
Despite these limitations, the results of this review
demonstrate that the training of health professionals in
breastfeeding promotion brings improvements in
knowl-edge,skills,andpractices,evenwhenthetrainingdoesnot
followtheWHO/UNICEFstandards.
As foradherence totheTenSteps,the evidencefound
inthereview waslessconsistent.Itmustberecalledthat
thesepracticesdependnotonlyonprofessionaltraining,but
alsoonadministrativemanagementsupportforinstitutional
changes.21
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.WorldHealthOrganization.Theoptimaldurationofexclusive breastfeeding: resultsof a WHO systematicreview. Geneva: WHO;2001.
2.MinistériodaSaúde.Saúdedacrianc¸a:nutric¸ãoinfantil: aleita-mentomaternoealimentac¸ãocomplementar(SérieA.Normas eManuaisTécnicos)(CadernosdeAtenc¸ãoBásica,n.23).1st ed.Brasília,DF:MinistériodaSaúde;2009.
3.Nakano AM,ReisMC,Pereira MJ,GomesFA. Oespac¸osocial das mulheres e a referência para o cuidado na prática da amamentac¸ão.RevLatino-AmEnfermagem.2007;15:41---50.
4.AzeredoCM,MaiaTM,RosaTC,SilvaFF,CeconPR,CottaRM. Percepc¸ão de mães e profissionais de saúde sobre o aleita-mentomaterno: encontrosedesencontros.RevPaul Pediatr. 2008;26:336---44.
5.Bonilha AL, Schmalfuss JM, Moretto VL, Lipinski JM, Porci-uncula MB. Capacitac¸ão participativa de pré-natalistas para a promoc¸ão do aleitamento materno. Rev Bras Enferm. 2010;63:811---6.
6.NakanoMA.Asvivênciasdaamamentac¸ãoparaum grupode mulheres: noslimitesde sero corpoparao filhoedeser o corpoparasi.CadSaudePublica.2003;19:S355---63.
450 deJesusPCetal.
8.BassichettoKC,ReaMF.Infantandyoungchildfeeding counsel-ing:aninterventionstudy.JPediatr(RioJ).2008;84:75---82.
9.MartensPJ.Doesbreastfeedingeducationaffectnursingstaff beliefs,exclusivebreastfeedingrates,andBaby-Friendly Hos-pitalInitiative compliance? The experienceof a small, rural Canadianhospital.JHumLact.2000;16:309---18.
10.Araújo MF, Schmitz BA. Dozeanos de evoluc¸ãoda iniciativa HospitalAmigodaCrianc¸anoBrasil.RevPanamSaludPublica. 2007;22:91---9.
11.FairbankL,O’MearaS,RenfrewMJ,WoolridgeM,SowdenAJ, Lister-SharpD.Asystematicreviewtoevaluatethe effective-nessofinterventionstopromotetheinitiationofbreastfeeding. HealthTechnolAssess.2000;4:1---171.
12.Spiby H, McCormick F, Wallace L, D’Souza L, Renfrew MJ, DysonL.Asystematicreviewofeducationandevidence-based practice interventions with health professionals and breast feedingcounsellorsondurationofbreastfeeding.Midwifery. 2009;25:50---61.
13.WHO/UNICEF.InnocentiDeclarationontheprotection, promo-tionandsupportofbreastfeeding.In:MeetingBreastfeedingin the1990s:aglobalinitiative.1990.
14.WHO/UNICEF. Baby-Friendly Hospital initiative: revised, updated and expanded for integrated care. Section 1: Backgroundandimplementation.WHO/UNICEF;2009.
15.DownsSH,BlackN.Thefeasibilityofcreatingachecklistforthe assessmentofthemethodologicalqualitybothofrandomised andnon-randomisedstudiesofhealthcareinterventions.J Epi-demiolCommunityHealth.1998;52:377---84.
16.WestphalMF,TaddeiJA,VenancioSI,BogusCM.Breast-feeding training for health professionals and resultant institutional changes.BullWorldHealthOrgan.1995;73:461---8.
17.McIntyreE,Lawlor-SmithC.Improvingthebreastfeeding knowl-edge of health professionals. Aust Fam Physician. 1996;25: S68---70.
18.Hernández-Gardu˜noAG,delaRosa-RuizL.Breast-feeding train-ingforthenursingstaffattheGeneralHospitalofMexico.Salud PublicaMex.2000;42:112---7.
19.Cattaneo A, Buzzetti R. Effect on rates of breast-feeding of training for the Baby Friendly Initiative. BMJ. 2001;323: 1358---62.
20.OwoajeET,OyemadeA,KoludeOO.PreviousBFHItrainingand nurses’knowledge,attitudesandpracticesregardingexclusive breastfeeding.AfrJMedMedSci.2002;37:137---40.
21.Zakarija-GrkovicI,BurmazT.EffectivenessoftheUNICEF/WHO 20-hourcourseinimprovinghealthprofessionals’knowledge, practices,andattitudestobreastfeeding:before/afterstudyof 5maternityfacilitiesinCroatia.CroatMedJ.2010;51:396---405.
22.Wissett L,DykesF,Bramwell R.EvaluatingtheWHO/UNICEF breastfeedingcourse.BJM.2000;8:294---300.
23.Bernaix LW, Beaman ML, Schmidt CA, Harris JH, Miller LM. Success ofaneducationalinterventiononmaternal/newborn nurses’breastfeedingknowledgeandattitudes.JOGNN.2010; 39:658---66.
24.Moran VH, Bramwell R, Dykes F, Dinwoodie K. An evalua-tion of skills acquisition on the WHO/UNICEF Breastfeeding
ManagementCourseusingthepre-validatedBreastfeeding Sup-portSkillsTool(BeSST).Midwifery.2000;16:197---203.
25.PrasadB, Costello AM. Impactand sustainability of a baby-friendlyhealtheducationinterventionatadistricthospitalin Bihar,India.BMY.1995;310:621---3.
26.TaddeiJA,WestphalMF,VenancioS,BogusC,SouzaS. Breast-feedingtrainingforhealthprofessionalsandresultantchanges inbreastfeedingduration.SaoPauloMedJ.2000;118:185---91.
27.DurandM,LabarereJ,BrunetE,PonsJ-C.Evaluationofa train-ingprogramforhealthcareprofessionalsaboutbreast-feeding. EurJObstGynecolReprodBiol.2003;106:134---8.
28.LabarereJ,CastellM,FournyM,DurandM,PonsJC.Atraining programonexclusivebreastfeedinginmaternitywards.IntJ GynecolObstet.2003;83:77---84.
29.CoutinhoSB,LimaMC,AshworthA,LiraPI.Impactode treina-mentobaseadonaIniciativaHospitalAmigodaCrianc¸a sobre práticasrelacionadasàamamentac¸ãonointeriordoNordeste. JPediatr(RioJ).2005;81:471---7.
30.Zakarija-GrkovicI,Segvic O,BozinovicT,CuzeA, LozancicT, VockovicA, etal.Hospitalpracticesand breastfeedingrates beforeandaftertheUNICEF/WHO20-hourcourseformaternity staff.JHumLact.2012;28:389---99.
31.World Health Organization and United Nations Children’s Fund.Breastfeedingmanagement:amodularcourse.London: UNICEF;1997.
32.WHO.CDDbreastfeedingcounselling:atrainingcourse.Update No.14;1994.
33.Wellstart:theSanDiegoLactationProgram.Statementof cor-poratecapabilities.SanDiego,CA:Wellstart;1990.
34.CanesquiAM,SpinelliMA.SaúdedafamílianoEstadodeMato Grosso,Brasil:perfisejulgamentosdosmédicoseenfermeiros. CadSaudePublica.2006;22:1881---92.
35.OliveiraMI, HartzZM,NascimentoVC,SilvaKS.Avaliac¸ãoda implantac¸ãodainiciativahospitalamigodacrianc¸anoRiode Janeiro,Brasil.RevBrasSaudeMaternInfant.2012;12:281---95.
36.NeifertMR.Theoptimizationofbreast-feedingintheperinatal period.ClinPerinatol.1998;25:303---26.
37.DonathSM,AmirLH,ALSPACStudyTeam.Relationshipbetween prenatalinfantfeedingintentionandinitiationanddurationof breastfeeding:acohortstudy.ActaPaediatr.2003;92:352---6.
38.TomaTS,MonteiroCA.Avaliac¸ãodapromoc¸ãodoaleitamento maternonasmaternidadespúblicaseprivadasdoMunicípiode SãoPaulo.RevSaudePublica.2001;35:409---14.
39.Esteves TM, Daumas RP, Oliveira MI, Andrade CA, Leite IC. Fatoresassociadosàamamentac¸ãonaprimeira horadevida: revisãosistemática.RevSaudePublica.2014;48:697---703.
40.LealMC,PereiraAP,DominguesRM,ThemeFilhaMM,DiasMA, Nakamura-PereiraM, et al.Intervenc¸õesobstétricas durante otrabalhodepartoepartoemmulheresbrasileirasde risco habitual.CadSaudePublica.2014;30:S17---47.
41.Rea MF.Reflexões sobrea amamentac¸ãono Brasil:de como passamosa 10meses de durac¸ão. Cad SaudePublica. 2003; 19:S37---45.