Jebmh.com
Original Article
J. Evid. Based Med. Healthc., pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 3/Issue 33/Apr. 25, 2016 Page 1586
CLINICAL PROFILE OF ANAEMIA IN A TERTIARY CARE HOSPITAL
Ather Akhtar Pasha1, Suhail Bin Ahmed2
1Assistant Professor, Department of General Medicine, Deccan College of Medical Sciences.
2Assistant Professor, Department of General Medicine, Deccan College of Medical Sciences.
ABSTRACT
BACKGROUND
Anaemia causes a reduction in the oxygen carrying capacity of the blood resulting in tissue hypoxia. Cardiac output at rest is not usually increased in most chronic anaemia until haemoglobin levels fall below 7 g/dL, but abnormal rise in output with exercise may occur with levels as high as 10 g/dL. The increase in cardiac output has been observed to correlate well with the degree of anaemia. Other compensatory mechanisms to chronic anaemia available to the body include decreased circulation time and increased tissue oxygen uptake. The latter is facilitated by a shift to the right of the oxygen haemoglobin dissociation curve. Cardiomegaly may also be as a result of the increased workload on the heart from the increased viscosity of blood in anaemia patients. Anaemia in the elderly is an extremely common problem that is associated with increased mortality and poorer health-related quality of life, regardless of the underlying cause of the low haemoglobin. A study of anaemia in elderly patients found a wide variation in prevalence, ranging from 2.9% to 61% in men and 3.3% to 41% in women. Higher rates were found in hospitalised patients than in community dwellers. It is easy to overlook anaemia in the elderly, since such symptoms as fatigue, weakness, or shortness of breath may be attributed to the ageing process itself.Our objective is to show the prevalence of anaemia even in a tertiary health care centre.
METHODS
One hundred patients were identified who were admitted in the Department of Medicine, Deccan College of Medical Sciences. Among the 100 patients, 38 were male and 62 were female.
The study was conducted from Jan 2014 To Jan 2015.
Patients having haemoglobin less than 10 g% in the medical wards were enrolled in the study.
RESULTS
Among the 100 patients, 38 were male and 62 were female. The average haemoglobin was 6.4 g%, the lowest being 2.8 g%. Peripheral blood smear showed hypochromic picture in 58, macrocytic picture in 22 and the morphology was normocytic normochromic in 20 cases.
Tuberculosis leading to anaemia was seen in 24, Internal haemorrhoids/Fissures 5, Taenia infestation in 3, Haematological Malignancies 2, GI Malignancies 3, Connective tissues disorders 3, Nutritional iron deficiency 8 and Anaemia of chronic diseases in remaining cases.
Among the 22 cases having macrocytic anaemia, 11 had vitamin B 12 deficiency, 6 had subclinical hypothyroidism, 5 had alcoholism.
Among the 20 patients having normocytic normochromic blood picture, 4 had haemolytic anaemia, 1 had aplastic anaemia and remaining were having anaemia of chronic disease mainly chronic kidney disease.
Regarding treatment, 23 patients were transfused blood. Out of total 100 patients included in the study, in-hospital mortality was 10.
CONCLUSIONS
Anaemia is associated with a variety of diseases. As Tuberculosis and B 12 Deficiency are among the leading causes of anaemia, hypochromic and microcytic picture was the predominant picture in peripheral blood smear. Among the patients having normocytic normochromic blood picture, majority were having chronic kidney disease which may be due to the fact that our hospital is a tertiary referral centre for chronic renal failure. In-hospital mortality due to anaemia alone is lower in tertiary care centres, but the mortality in our study is due to associated comorbid conditions like chronic renal failure and malignancy.
KEYWORDS
Anaemia, Tertiary Hospital, Prevalence, Chronic Diseases, Age Distribution.
HOW TO CITE THIS ARTICLE: Pasha AA, Ahmed SB. Clinical profile of anaemia in a tertiary care hospital. J. Evid. Based Med. Healthc. 2016; 3(33), 1586-1589. DOI: 10.18410/jebmh/2016/356
INTRODUCTION: According to WHO, anaemia is the qualitative and or quantitative diminution of haemoglobin or RBC or both in respect to the age and sex of the individual, and anaemia is defined as a reduction of the total circulating red cell mass below normal limits. Though anaemia is less common among males, but they do suffer from anaemia to a considerable extent to their counterpart in developed
Financial or Other, Competing Interest: None. Submission 01-04-2016, Peer Review 15-04-2016, Acceptance 23-04-2016, Published 25-04-2016. Corresponding Author:
Dr. Ather Akhtar Pasha,
#10-01-128/1/2D, 1st Floor, Ali Manor Masab Tank, Hyderabad-500028, Telangana.
Jebmh.com
Original Article
J. Evid. Based Med. Healthc., pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 3/Issue 33/Apr. 25, 2016 Page 1587
countries. Adverse effects of anaemia are various as for example on nervous system, on physical response to diseases, physiological stressed condition like pregnancies and like iron, vit. B12 and folate deficiencies are the common causes of anaemia. Anaemia is wide spread in India, but it varies in severity from state to state and zone to zone. Poor diet, lack of sense of hygiene which leads to worm infestations, lack of health consciousness, chronic infections, social taboos and poor economic status, all contribute to overwhelming prevalence of anaemia.
Anaemia is defined as decreased red cell count or its one of the content the haemoglobin. The diagnosis to confirm is also usually done by measuring the haemoglobin content in the blood. There are different ways to identify anaemia. It can also be done by performing either the total RBC count or by estimating the packed cell volume. Clinically, there are a plethora of signs to identify the disease. Paleness either in the lower part of palpebral fissure, nails or tongue are the important sights that are frequently examined to estimate the degree of anaemia. However, detection of morphological types of anaemia depends on various blood indices.
Anaemia can be classified either morphologically or aetiologically. The most common causes are enumerated below:
Nutritional deficiencies (especially deficiencies of iron and vitamin B12).
Aplasia of bone marrow.
Anaemia associated with chronic diseases.
Anaemia associated with renal failure.
Anaemia associated with inherited diseases.
Anaemia due to blood loss.
Aetiologically, they can be further classified into two broad groups, they are:
1. Due to decreased red cell production:
Stem cell failure (aplastic anaemia).
Progenitor cell failure (pure red cell failure, chronic renal failure, chronic diseases).
Precursor cell failure (megaloblastic, iron deficiency, thalassaemia).
2. Due to red cell destruction:
Acquired causes (acute blood loss,
hypersplenism, antibody mediated).
Hereditary causes (membrane defects, enzyme defects, globin defects).
There is a plethora of causes that are included in both the above said aetiological causes.
Morphologically, the anaemia can be classified into:
Hypochromic microcytic anaemia.
Normochromic normocytic anaemia.
Macrocytic anaemia.
In the clinical settings, the identification of the anaemia is quite difficult because the signs and symptom depends upon a lot of variables. Acute anaemia is usually presented
as a patient with shock. Chronic patients on the other hand will be accustomed to the disease and the signs and symptoms differs in chronic anaemia.
Anaemia causes a reduction in the oxygen carrying capacity of the blood resulting in tissue hypoxia.1 Cardiac
output at rest is not usually increased in most chronic anaemia until haemoglobin levels fall below 7 g/dL, but abnormal rise in output with exercise may occur with levels as high as 10 g/dL.2 The increase in cardiac output has been
observed to correlate well with the degree of anaemia.3
Other compensatory mechanisms to chronic anaemia available to the body include decreased circulation time and increased tissue oxygen uptake. The latter is facilitated by a shift to the right of the oxygen haemoglobin dissociation curve.4,5 Cardiomegaly may also be as a result of the
increased workload on the heart from the increased viscosity of blood in anaemia patients.6 Anaemia in the elderly is an
extremely common problem that is associated with increased mortality and poorer health-related quality of life, regardless of the underlying cause of the low haemoglobin.7,8 A study of anaemia in elderly patients found
a wide variation in prevalence ranging from 2.9% to 61% in men and 3.3% to 41% in women. Higher rates were found in hospitalised patients than in community dwellers.9 It is
easy to overlook anaemia in the elderly, since such symptoms as fatigue, weakness, or shortness of breath may be attributed to the ageing process itself.10
Our objective is to show the prevalence of anaemia even in a tertiary health care centre. So, treating anaemia while evaluating its cause with careful history, examination and relevant investigations will help to control the growing menace of anaemia and its associated mortality and morbidity.
AIMS AND OBJECTIVES:
1. To study the prevalence of anaemia in tertiary health care.
2. To find the most common cause. 3. To study the blood picture. 4. To study the correlation of age.
5. To study the mean Hb% in different causes of anaemia.
MATERIALS AND METHODS: One hundred patients were identified who were admitted in the Department of Medicine, Deccan College of Medical Sciences. Among the 100 patients, 38 were male and 62 were female.
The study was conducted from Jan 2014 To Jan 2015. Patients having haemoglobin less than 10 g percent in the medical wards of were enrolled in the study.
Jebmh.com
Original Article
J. Evid. Based Med. Healthc., pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 3/Issue 33/Apr. 25, 2016 Page 1588 Inclusion Criteria:
1. Patients who were aged between 20 and 30 years of age.
2. Patients who were admitted and were unknown of the anaemia state was included.
Exclusion Criteria:
1. Patients who were on drugs which are known to cause anaemia (drug-induced anaemia) were excluded.
RESULTS: Among the 100 patients, 38 were male and 62 were female. The prevalence was found to be high in females.
Chart 1: Prevalence correlation in sex
The mean age group was 38 years in males and 27 years in females.
Chart 2: Age correlation in individual sex
The mean haemoglobin was 6.4 g% the lowest being 2.8 g%.
Peripheral blood smear showed hypochromic picture in 58, macrocytic picture in 22 and the morphology was normocytic normochromic in 20 cases.
Chart 3: Morphological Distribution
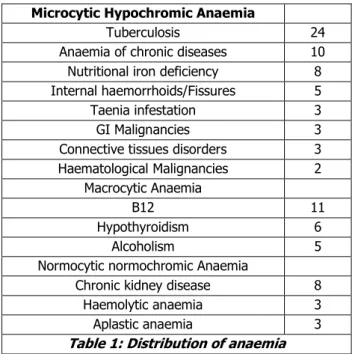
Tuberculosis leading to anaemia was seen in 24, Internal haemorrhoids/fissures 5, Taenia infestation in 3, Haematological Malignancies 2, GI Malignancies 3, Connective tissues disorders 3, nutritional iron deficiency 8 and anaemia of chronic diseases in remaining cases.
Among the 22 cases having macrocytic anaemia, 11 had vitamin B 12 deficiency, 6 had subclinical hypothyroidism, 5 had alcoholism. Among the 20 patients having normocytic normochromic blood picture, 4 had haemolytic anaemia, 1 had aplastic anaemia and remaining were having anaemia of chronic disease mainly chronic kidney disease.
Regarding treatment, 23 patients were transfused blood. Out of total 100 patients included in the study, in-hospital mortality was 10.
Microcytic Hypochromic Anaemia
Tuberculosis 24
Anaemia of chronic diseases 10
Nutritional iron deficiency 8
Internal haemorrhoids/Fissures 5
Taenia infestation 3
GI Malignancies 3
Connective tissues disorders 3
Haematological Malignancies 2
Macrocytic Anaemia
B12 11
Hypothyroidism 6
Alcoholism 5
Normocytic normochromic Anaemia
Chronic kidney disease 8
Haemolytic anaemia 3
Aplastic anaemia 3
Table 1: Distribution of anaemia
DISCUSSION: In the medical wards, Anaemia is a common clinical condition. Most of the patients who are admitted in the tertiary care have been diagnosed with anaemia. Most of the patients were having some other medical problems and were having associated anaemia. The patients never came with any signs and symptoms of anaemia. They were accidentally diagnosed on routine examination of the peripheral smear. As nutritional iron deficiency is very common and people having haemoglobin more than 10 without other comorbidities rarely seek medical suggestions in our setup, patients having haemoglobin less than 10 were included in the study. Females are affected more than males, more likely due to higher occurrence of nutritional deficiencies and its complications as well as loss of blood due to worm infestation. The misery these parasites inflict on humans remains a major health problem worldwide.11
The relationship between parasitic infestation and anaemia is a pathogeno-physiologic type.12 Among the 100
patients, 38 were male and 62 were female. The prevalence was found to be high in females. This study is not in agreement with that of K. S. Lamsal.13 This may be due to
Jebmh.com
Original Article
J. Evid. Based Med. Healthc., pISSN- 2349-2562, eISSN- 2349-2570/ Vol. 3/Issue 33/Apr. 25, 2016 Page 1589
studied is different and the other fact might be because of the present study has been done in a tertiary centre, most of the referral cases are chronically ill which is known to diminish erythropoiesis.
The mean age group was 38 years in males and 27 years in females. The mean age of the girls presenting is significantly lower when compared to the mean age of the male counterpart. This might be due to the menstruation cycle blood loss and non-compensation of the lost blood by consumption of incomplete diet and top of that the burden of the disease. All combined together may be the answer to the above question.
The mean haemoglobin was 6.4 g%, the lowest being 2.8 g%. Peripheral blood smear showed hypochromic picture in 58, macrocytic picture in 22 and the morphology was normocytic normochromic in 20 cases. Tuberculosis leading to anaemia was seen in 24, Internal haemorrhoids/Fissures 5, Taenia infestation in 3, Haematological Malignancies 2, GI Malignancies 3, Connective tissues disorders 3, Nutritional Iron Deficiency 8 and Anaemia of chronic diseases in remaining cases. Among the 22 cases having macrocytic anaemia, 11 had vitamin B 12 deficiency, 6 had subclinical hypothyroidism, 5 had alcoholism. Among the 20 patients having normocytic normochromic blood picture, 4 had haemolytic anaemia, 1 had aplastic anaemia and remaining were having anaemia of chronic disease mainly chronic kidney disease.
The mortality was also on the higher side which comprised of ten percent. This shows the potential of this silent disease in a tertiary hospital if not taken into consideration and treated accordingly.
CONCLUSION: Anaemia is associated with a variety of diseases. as tuberculosis and B 12 deficiency are among the leading causes of anaemia, hypochromic and microcytic picture was the predominant picture in peripheral blood smear. Among the patients having normocytic normochromic blood picture, majority were having chronic kidney disease which may be due to the fact that our hospital is a tertiary referral centre for chronic renal failure. In-hospital mortality due to anaemia alone is lower in tertiary care centres, but the mortality in our study is due to associated comorbid conditions like chronic renal failure and malignancy.
REFERENCES:
1. Wintrobe MM. The cardiovascular system in anaemia, with a note on the particular abnormalities in sickle cell anaemia. Blood 1946;1:121-128.
2. Duke M, Abelmann WH. The haemodynamic response to chronic anaemia. Circulation 1969;39:503-515. 3. Horne MK. Sickle cell anaemia as a rheologic diseases.
Am J Med 1981;70(2):288-298.
4. Adeniyi JO, Akintude EA. Sickle cell haemoglobin survey among children in Ilorin, Nigeria. Program and book of abstracts, Sixth congress of International society Haematology Lagos, Nigeria 1987.
5. Powars DR, Chan LS, Schroode WA. The variable expression of sickle cell disease is genetically determined. Semin Hematol 1990;27(4):360-365. 6. Varat MA, Adolph RJ, Fowler NO. Cardiovascular
effects of anaemia. Am Heart J 1972;83(3):415-426. 7. Udristioiu A, Cojocaru M, Florescu C, et al. Screening tests for latent anaemia in hospitalized adults over the age of 65. Lab medicine 2010;41(5):288-291. 8. Tanne D, Molshatzki N, Merzeliak O, et al. Anaemia
status, haemoglobin concentration and outcome after acute stroke: a cohort study. BMC Neurol 2010;10: 22.
9. Beghe C, Wilson A, Ershler WB. Prevalence and outcomes of anaemia in geriatrics: A systematic review of the literature. Am J Med 2004;116(Suppl 7A):3S-10S.
10. Shrivastava SR, Hippargi SB, Ambali AP, et al. Patterns of anaemia in geriatric age group. JKIMSU 2013;2(1):77-81.
11. Kaeni Agiomea. Anaesthetic considerations in patients with parasitic diseases and anaemia. 2003;1-8. http://www.nda.ox.ac.uk/wfsa/dL/html/papers /pap021.htm;
12. Stepon LS, Latham C, Kurz KM, et al. Relationships of S. haematobium, hookworm and malarial infections and metrifonate treatment on haemoglobin level in Kenyan school children. Am J Trop Med 1985;34(3): 519-528.