SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Double-bundle
PCL
reconstruction
using
autologous
hamstring
tendons:
outcome
with
a
minimum
2-year
follow-up
夽
Ricardo
de
Paula
Leite
Cury,
Rômulo
Neves
Castro
Filho,
Daniel
Akira
Sadatsune,
Davi
Ribeiro
do
Prado,
Ricardo
José
Peruzzo
Gonc¸alves,
Marcos
Barbieri
Mestriner
∗FaculdadedeCiênciasMédicasdaSantaCasadeMisericórdiadeSãoPaulo(FCMSCSP),DepartamentodeOrtopediaeTraumatologia, SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received16March2016 Accepted13June2016 Availableonline6March2017
Keywords: Knee/surgery
Posteriorcruciateligament Kneeinjuries
Evaluationofresultsoftherapeutic interventions
a
b
s
t
r
a
c
t
Objective:Topresenttheoutcomesofposteriorcruciateligament(PCL)double-bundle recon-structionusingautologoushamstringtendons,withaminimumfollow-upoftwoyears. Methods:Evaluationof16casesofPCLinjurythatunderwentdouble-bundlereconstruction withautogenoushamstringtendons,between2011and2013.Thefinalsampleconsistedof 16patients,15menandonewoman,withameanageof31years(21–49).Thepredominant mechanismwasmotorcycleaccidentinhalfofthecases.Therewasameanintervalof 15monthsbetweenthetimeoflesionandthesurgery(threeto52months).Fivelesions wereisolatedand11,associated.Clinicalevaluation,applicationofvalidatedscores,and measurementswithuseoftheKT-1000wereperformed.
Results:The analysisshowed a mean preoperative Lysholm score of50 points(28–87), progressing to 94 points (85–100) postoperatively. The IKDC score also demonstrated improvement.Inthepreoperativeevaluation,fourand12patientswererespectively clas-sifiedasC(abnormal)andD(veryunusual),andinthepostoperativeevaluationsixasA (normal)andtenasB(closetonormal).Inthepost-operativeevaluationbyKT1000 arthrom-eter,13 patientsshoweddifferencebetween0–2mmand3between3and5mm,when comparedwiththecontralateralside.
Conclusion: Autologoushamstringtendonsareaviableoptionindouble-bundle reconstruc-tionofthePCL,withgoodclinicalresultsinaminimumfollow-upoftwoyears.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheFaculdadedeCiênciasMédicasdaSantaCasadeMisericórdiadeSãoPaulo(FCMSCSP),Departamentode OrtopediaeTraumatologia,GrupodeCirurgiadoJoelho,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](M.B.Mestriner).
http://dx.doi.org/10.1016/j.rboe.2017.02.006
Reconstruc¸ão
do
ligamento
cruzado
posterior
em
dupla
banda
com
tendões
flexores
autólogos:
resultados
com
seguimento
mínimo
de
dois
anos
Palavras-chave: Joelho/cirurgia
Ligamentocruzadoposterior Traumatismosdojoelho Avaliac¸ãodosresultadosde intervenc¸õesterapêuticas
r
e
s
u
m
o
Objetivo: Apresentarosresultadosdeumasériedecasosdereconstruc¸ãodoligamento cruzadoposterior(LCP)emduplabandacomousodostendõesflexoresautólogos,com seguimentomínimodedoisanos.
Métodos: Avaliac¸ãode16casosdelesãodoLCPsubmetidosareconstruc¸ãoemduplabanda comtendõesflexoresautólogosentre2011e2013.Aamostrafinalfoi compostapor 16 pacientes,15homenseumamulher,commédiade31anos(21-49).Omecanismo predom-inantefoiacidentemotociclísticoemmetadedoscasos.Houveumintervalomédiode15 mesesentrealesãoeacirurgia(trêsa52meses).Cincolesõeseramisoladase11, associ-adas.Foramfeitasavaliac¸ãoclínica,aplicac¸ãodeescoresvalidadosemensurac¸ãocomuso doartrômetroKT-1000.
Resultados: Aavaliac¸ãopela escalade Lysholmpré-operatóriatevemédia de55pontos (28-87),evoluiuparaumamédiapós-operatóriade94 pontos(85-100).OIKDCtambém demonstroumelhoria.Naavaliac¸ãopré-operatória,quatroe12pacientesforam respectiva-menteclassificadoscomoC(anormal)eD(muitoanormal);naavaliac¸ãopós-operatória,
seisforamclassificadoscomoA(normal)edezcomoB(próximoaonormal).Naavaliac¸ão pós-operatóriapeloartrômetroKT1000,13pacientesapresentaramdiferenc¸aentre0-2mm etrês,entre3-5mm,nacomparac¸ãocomoladocontralateral.
Conclusão: Ousodostendõesflexoresautólogoséumaopc¸ãoviávelnareconstruc¸ãodoLCP emduplabanda,apresentabonsresultadosclínicosemseguimentomínimodedoisanos.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Reconstructionsoftheposteriorcruciateligament(PCL)are achallengetotheknee surgeon.Thefrequentlyassociated injuriesanddifficultiesofthereconstructiveprocedurelead todifficulttoachieveand ofteninferiorresultswhen com-paredto anterior cruciate ligament (ACL)reconstructions.1
The main discussions regarding this treatment refer to graft options and reconstruction with single or double bundle.
Theflexortendonshavebeenshowntobeaveryuseful toolinthereproductionofthePCL’sbiomechanicalproperties. Suchgraftshavetheadvantagesofreadyavailabilitywithout theneedofatissuebank,noaggressiontotheextensor mech-anism,lowmorbidityinthedonorarea,andthegraftseasy passagethroughthebonetunnels,inadditiontocomplete fill-ingoftunnels,favoringintegrationandstability.2–6Moreover,
itispossibletoremovetendonsfrombothkneesandincrease thefinalthickness,withgreaterresemblancetotheoriginal PCL.
AnotherquestionconcernsthereconstructionofthePCL withasinglefemoraltunnelordouble-bundle,thelatterbeing anattempttomoreeffectivelyreproducetheoriginalanatomy oftheligament.Bycreatingtwofemoraltunnels,theknee sur-geonaimstomaintainthe biomechanicalpropertiesofthe PCL.Recentstudieshavedemonstratedthesuperiorityofthis techniqueintermsofkneestability,despitethegreater com-plexityoftheprocedure.7–14
Theobjectiveofthepresentstudyistopresenttheresults ofaseriesofcasesofdouble-bundlePCLreconstructionusing autologousflexor tendonsofbothknees,with aminimum follow-upoftwoyears.
Patients
and
methods
Thestudy includedcasesofisolated grade2or 3PCL rup-turesthatweresymptomaticafterconservativetreatmentor wereassociatedwithotherinjuries,treatedbetween2011and 2013.Skeletallymaturepatients,withnoagelimit,andwithno previousinjuriesand/orsurgicaltreatmentinthekneewere included.Thefinalanalysisincluded16patients,15menand onewoman.Themeanpatientagewas31years(21–49);the mainmechanismwasmotorcycleaccidentineightpatients, automobileaccident infour,and sports injuryinfour.The mean interval between injuryand surgerywas 15 months (3–52).
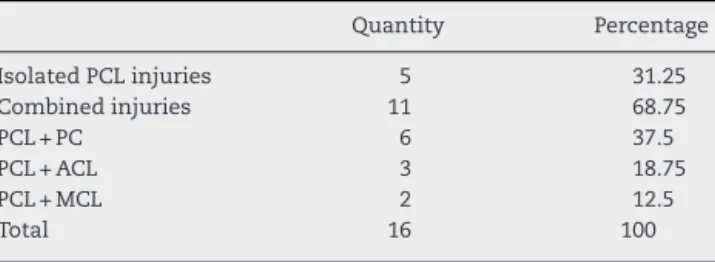
Five patients had isolated PCL involvementand 11 pre-sentedassociatedligamentdamage.Table1summarizesthe associatedlesions.
Thosewhodidnotmeetthecriteriamentioned,with clini-caland/orradiographicsignsofosteoarthrosisorboneinjuries (fractures)inthekneeregion,wereexcluded.
Patients underwent preoperative evaluation including physicalexaminationandapplicationoftheLysholm15 and
Table1–Frequencyofligamentinjuries.
Quantity Percentage
IsolatedPCLinjuries 5 31.25
Combinedinjuries 11 68.75
PCL+PC 6 37.5
PCL+ACL 3 18.75
PCL+MCL 2 12.5
Total 16 100
PC,posterolateral corner;ACL, anteriorcruciate ligament;MCL, medialcollateralligament;PCL,posteriorcruciateligament. Observation:Ofthepatientswith combinedinjuries,fivehada chondralinjury(31.25%) andonehada lateralmeniscal injury (6.25%).
X-raysofbothkneesinanteroposteriorandlateralviews,axial viewofthepatella,panoramicX-rayofthelowerlimbs,and magneticresonanceoftheaffectedknee.
Thesurgicalprocedurewasalwaysperformedbythesame surgeon,afterphysicalexaminationundersedationthat clin-icallydocumentedtheobservedlesions.Theflexortendons (semitendinosusandgracilis)wereremovedfrombothlimbs andwerepreparedandmeasuredbyanassistantsurgeon.
Toreconstructisolated PCLinjuriesthe transtibial tech-niquewasusedtoreconstructisolatedPCLinjuries,withthe flexortendonsdivided asfollows:twosemitendinosus ten-dongraftsreservedforthereconstructionoftheanterolateral (AL)bundleandtwogracilisgraftsfortheposteromedial(PM) bundle.Thisstrategyaimedtoensureasatisfactorythickness ofthereconstructedligament.Ameansizeof9–10mmwas achievedwiththeassociationofsemitendinosusgraftsandof 8–9mmwithgracilisgrafts;thesevaluescomprisethemean thicknessofeachbundleanditsrespectivefemoraltunnel.
Incasesofassociatedperipheralinjury,asingle semitendi-nosustendonwasusedforreconstruction.Inthesesituations, thePCLtreatmentstrategywasmodified:theremnant semi-tendinosustendonassociatedwithonegraciliswasreserved forAL bundle reconstruction, and a singlegracilis muscle graftwasreservedforthePMbundle.TheFanellitechnique wasthechoiceforinjuriesoftheposterolateralregion.16
ACL-associatedinjurieswerereconstructedinasecondmoment, usingthecentralthirdofthepatellartendonoftheinjured knee.Injuriesofthemedialcollateralligamentweretreated conservatively.
The arthroscopic stage of the surgery was initiated by carefuljointinspection;meniscalandchondrallesionswere documented and treated. Then, the injured ligament was debridedandthedistalbedofthePCLwaspreparedthrough anaccessoryposteromedialportal.Thecreationofthetibial tunnelsbeganwiththeuseofanappropriateguideand flu-oroscopiccontrolofthewirepassagetominimizetheriskof vascularinjury.ThechosensitewasthecenterofthePCL foot-printintheanteroposteriorview,placedinthemidpointofthe lowerhalfofthePCLfacetinthelateralview.Femoraltunnels werecreatedwiththehelpofanoutside-inguide,respecting theanatomicalpositionofthePCL;thecenteroftheALand PMbundlestothearticularcartilagemeasured7and9mm, respectively.
Afterthegrafts werepassed,asingletibialfixationwas carried out. TheAL bundlewas fixated first in the femur,
tensionedat90degreesofflexion.Subsequently,thekneewas extendedandthePMbundlewasfixatedinfullextension.In alltunnels(femoralandtibial),thefixationwasachievedwith absorbableinterferencescrews(Arthrex®,Naples,FL,USA).
Figs.1and2showthesiteswherethetunnelsweremadeinthe tibiaandfemurforPCLreconstruction,whileFig.3showsthe processofreconstructionoftheposterolateralcorner.Fig.4
showstheappearanceofthePCLreconstructioninmagnetic resonanceimaging(MRI).
Aftertheprocedure,thepatientsunderwentastandardized rehabilitationprotocol.17
Inthepostoperativeperiod,thefinalassessmentwasmade ataminimumfollow-upoftwoyears,whenaoppositelimb comparativephysicalexaminationwasperformed. The tib-ialposteriorizationwasmeasuredusingtheKT-1000,andthe IKDCandLysholmscoreswereagainapplied.Both preopera-tiveandpostoperativeassessmentswereperformedbythree oftheauthors.
ThestudywasapprovedbytheResearchEthicsCommittee underCAAENo.15810213.3.0000.5479.
Results
When assessing the scores, a mean preoperative Lysholm of55points(poor) wasobserved,rangingfrom 28to87.In the postoperative evaluation, there was a significant score improvement,withameanof94points(excellent),ranging from 85 to100. When separatingisolated PCLinjuries and associatedinjuries,thepostoperativeanalysisdemonstrated aconsiderablenumericalsimilarity.Inpatientswithisolated PCLinvolvement,ameanprogressionfrom63.6to94.6was observed.Inpatientsinwhomtheposterolateralcornerwas also involved(six cases),the mean progressionwent from 52.75 to94; incases ofPCL and ACL injuries(three cases) were from63.6to94.6.Finally,inpatientswithPCL associ-atedwithmedialcollateralligamentinjuries(twocases),from 40.5to95.Theseresultshighlightthelowersubjective preop-erativeevaluationofthepatientswithassociatedperipheral injury, both in the posterolateral corner and the medial compartment.
Table2–Pre-andpostoperativeIKDC.
IsolatedIKDClesions Preoperative period
Postoperative period
Complex IKDClesions
Preoperative period
Postoperative period
A 0 0 A 0 6(54.5%)
B 0 5(100%) B 0 5(45.5%)
C 3(60%) 0 C 2(18.2%) 0
D 2(40%) 0 D 9(81.8%) 0
Total 5(31.25%) Total 11(68.75%)
Total 16(100%)
InthepostoperativeanalysisusingtheKT-1000 arthrome-ter,thedifferencerangedfrom0to2mmin13casesandfrom 3to5mminthree.
Thereversepivot-shifttestwasperformed,andthe exter-naltibial rotation was measured bydial test at30 and 90 degrees.Nocasewaspositive,andtheremainingexternal tib-ialrotationwaslessthan5degreesinallcasesoperated.The postoperativerangeofmotionwassimilartothenon-operated limbinallcases.Mildpatellofemoralcrepituswasobservedin sixcases.Nosignificantmuscleatrophywasobservedinthe operatedpatients.Therewerenocomplaintsofpainrelated tograftremoval.
Discussion
EffectivelyreproducingthebiomechanicalpropertiesofPCL ischallenging, giventhe biomechanicalcharacteristics and
forcesactingonthisgraft,inadditiontothelowerincidence ofinjuries,whichmakesthelearningcurvesteeper.
Theuse ofthe flexortendonsisaveryfunctional alter-native, with good results documented in the literature. In the1990s,Pinczewskietal.18 presentedaseriesof40cases
of PCL reconstructions using flexor tendons. At that time, Shino et al.19 published a technique that used the
semi-tendinosus/gracilisforsinglebundlereconstruction,butwith suspensoryfixation;bothpresentedsatisfactoryresults.
Thepresentstudyhasanewfeatureinrelationtothe pre-viousliterature:reconstructionutilizingadoublebundlewith autologous graft oftheflexor tendons,removed from both limbs.Thisoptionrepresentstheevolutionofalineofresearch bytheauthorsinthereconstructionsofthePCL.Theauthors believe thatthis technique, albeitmoredemandingfrom a technicalstandpoint,reproducesmoreeffectivelythe poste-riorstabilizationoftheknee.Thedoublebundle,whichinthe
Fig.2–Femoraltunnelreamingsitesinthemedialfemoral condyleinPCLreconstruction,showingthedistanceof eachtunnelinrelationtotheborderofthedistalcartilage (inblack,ALbundleandinyellow,PMbundle).
pastlackedbetterqualitystudiesinrelationtothe methodol-ogyemployed,hashaditssuperioritydemonstratedinrecent studies.Inarecentmeta-analysisthatincluded435patients, Zhao et al.20 observed that double-bundle reconstruction
wassuperiortothesingle-bundletechniqueinisolatedPCL injurieswhenkneestabilitywasmeasuredat90degreesof flexion.
Theliteraturealso features the comparisonofdifferent grafts.Chenetal.21 madeacomparativeanalysisoftheuse
ofthe flexortendons and quadricepstendon, both autolo-gous.Atotalof54patientswere assessedandthe authors concludedthatbothgrafts weresatisfactory.Acomparative analysisbetweentheuseoftheAchillestendonandthe semi-tendinous/gracilistendonswasretrievedintheliterature.Ahn etal.1randomized36patientsbetweentheaforementioned
grafts.Thoseauthorsfoundsimilarresultswithboth tech-niques,notingthatthe smallerlengthanddiameterofthe flexortendonsdidnotinterfereintheresults.
Fig.3–Illustrationofthetechniqueusedforposterolateral cornerreconstruction.
Source:FanelliGC.16
Although a comparative analysis of the grafts was not included, the present authors have published a series on the use of the quadricipital tendon associated with the semitendinosus.22,23Theauthorslistthefollowingas
advan-tages of the use of the flexor tendons: the nonaggression toextensormechanism, whichenhancesrehabilitationand reducespostoperativemorbidity;greatereaseinpassingthe graftthrough thebonetunnels;thecompletionofthe tun-nels;andthepossibilityoffixationwithinterferencescrews directlyintothegraft,withoutinterfaces.Theauthorsbelieve thatthisbiomechanicalaspectofthefixationcanadd stabil-itytothereconstruction,sincethepostscrewfixationusedfor thequadricipitaltendon,consideredbiomechanicallyinferior, isnolongernecessary.Thepresentresultscorroboratethese hypotheses,sincein81%ofthecasestherewasnodifference inposteriorstabilitywiththekneeat90degreesintheKT-1000 analysis.
Inthepresentstudy,itwasnotpossibletoclearlyestablish anyfactorsthatcould determineaworseor better progno-sisafter ligament reconstruction (gender, age, and trauma mechanism,amongothers).Nonetheless,itwasobservedthat caseswithassociatedinjuries,inwhichtheinstabilitypriorto surgerywasmorepronouncedthanintheisolatedcases, ben-efitedthemostfromthesurgicalprocedure,asassessedbythe greatervariationofthescoresbetweenthepre-and postop-erativeperiod.Patellofemoralcrepituswasobservedincases withlowerpostoperativescore(bothinLysholmandIKDC);the authorsbelievethatitisrelatedtodirecttraumainthe ante-riorregionofthekneeandcanleadtopainand/ordiscomfort eveninthepresenceofastableknee.Thisfactor,however, waspresentbothincasesofisolatedandcombinedlesions.
Animportantquestionrelatedtobilateralremovalofthe flexortendoninvolvesinterventioninthehealthylimb.From a technical standpoint, the removal of all tendons is nec-essary, aimingatamoreexact reproductionofthe natural dimensionsofthePCL,sinceitisbelievedthatgraftthickness playsanimportantroleinthefinalstability.Inthepresent study,nomajorclinicalcomplaintsrelatedtothedonorsite wereregistered.Moreover,nopatellofemoralcrepitusor sig-nificantmuscularatrophywereobserved.Thisinformationis inagreementwiththeliterature.Yasudaetal.24analyzedthe
aspectsofmorbidityin65casesofACLinjuriesthatunderwent removaloftheflexortendons. Theauthorsfoundminimal complaintsrelatedto donorsite.Muscle strength was also measured;thealterationsobservedresolvedinapproximately oneyear.Theauthorsconcludethatflexortendonsarea sat-isfactoryoption,withminimalassociatedmorbidity.
Theinformation presented inthis article isof extreme importanceconsideringthe reality ofmostorthopedic ser-vicesindevelopingcountries,whereaccesstoatissuebankis stilllackingandcostly.
Thelimitationsofthepresentstudyarethesmallnumber ofpatients,thelackofacontrolgroup,andtheinclusionof isolatedandcombinedlesionsinthesamesample.
Conclusion
Theuse offlexortendonautograftisaviableoptioninthe reconstructionofthePCLusingadoublebundle,presenting
goodclinicalresultsinatwo-yearfollow-up.Thistechnique haslowratesofcomplicationsandmorbidityinthegraftdonor site.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.AhnJH,YooJC,WangJH.Posteriorcruciateligament reconstruction:double-loophamstringtendonautograft versusAchillestendonallograft–clinicalresultsofa minimum2-yearfollow-up.Arthroscopy.2005;21(8):965–9.
2.BullisDW,PaulosLE.Reconstructionoftheposteriorcruciate ligamentwithallograft.ClinSportsMed.1994;13(3):581–97.
3.IndelicatoPA,BittarES,PrevotTJ,WoodsGA,BranchTP, HuegelM.Clinicalcomparisonoffreeze-driedandfresh frozenpatellartendonallograftsforanteriorcruciate ligamentreconstructionoftheknee.AmJSportsMed. 1990;18(4):335–42.
4.NemzekJA,ArnoczkySP,SwensonCL.Retroviral transmissioninboneallotransplantation.Theeffectsof tissueprocessing.ClinOrthopRelatRes.1996;(324):275–82.
5.JacksonDW,GroodES,ArnoczkySP,ButlerDL,SimonTM. Freezedriedanteriorcruciateligamentallografts.Preliminary studiesinagoatmodel.AmJSportsMed.1987;15(4):295–303.
6.DefrereJ,FranckartA.Freeze-driedfascialataallograftsinthe reconstructionofanteriorcruciateligamentdefects.A two-toseven-yearfollow-upstudy.ClinOrthopRelatRes. 1994;(303):56–66.
7.HarnerCD,JanaushekMA,KanamoriA,YagiM,VogrinTM, WooSL.Biomechanicalanalysisofadouble-bandleposterior cruciateligamentreconstruction.AmJSportsMed.
2000;28(2):144–51.
8.RaceA,AmisAA.PCLreconstruction.Invitrobiomechanical comparisonofisometricversussingleanddouble-bundled ‘anatomic’grafts.JBoneJointSurgBr.1998;80(1):173–9.
9.YasudaK,KitamuraN,KondoE,HayashiR,InoueM. One-stageanatomicdouble-bundleanteriorandposterior cruciateligamentreconstructionusingtheautogenous hamstringtendons.KneeSurgSportsTraumatolArthrosc. 2009;17(7):800–5.
10.NylandJ,HesterP,CabornDN.Double-bundleposterior cruciateligamentreconstructionwithallografttissue:2-year postoperativeoutcomes.KneeSurgSportsTraumatol Arthrosc.2002;10(5):274–9.
11.BordenPS,NylandJA,CabornDN.Posteriorcruciateligament reconstruction(doublebundle)usinganteriortibialistendon allograft.Arthroscopy.2001;17(4):E14.
12.ChenCH,ChenWJ,ShihCH.Arthroscopicdouble-bundled posteriorcruciateligamentreconstructionwithquadriceps tendon-patellarboneautograft.Arthroscopy.2000;16(7):780–2.
13.MarkolfKL,FeeleyBT,JacksonSR,McAllisterDR.
Biomechanicalstudiesofdouble-bundleposteriorcruciate ligamentreconstructions.JBoneJointSurgAm.
2006;88(8):1788–94.
14.ShonOJ,LeeDC,ParkCH,KimWH,JungKA.Acomparisonof arthroscopicallyassistedsingleanddoublebundletibialinlay reconstructionforisolatedposteriorcruciateligamentinjury. ClinOrthopSurg.2010;2(2):76–84.
16.FanelliGC.Fibularhead-basedposterolateralreconstruction oftheknee:surgicaltechniqueandoucomes.JKneeSurg. 2015;28(6):455–63.
17.CuryRPL,KiyomotoHD,RosalGF,BrykFF,OliveiraVM, CamargoOPA.Protocolodereabilitac¸ãoparaasreconstruc¸ões isoladasdoligamentocruzadoposterior.RevBrasOrtop. 2012;47(4):421–7.
18.PinczewskiLA,ThuressonP,OttoDD,NyquistF.Arthroscopic posteriorcruciateligamentreconstructionusingfourstrand hamstringtendongraftandinterferencescrews.Arthroscopy. 1997;13(5):661–5.
19.ShinoK,NakagawaS,NakamuraN,MatsumotoN,Toritsuka Y,Natsu-umeT.Arthroscopicposteriorcruciateligament reconstructionusinghamstringtendons:one-incision techniquewithEndobutton.Arthroscopy.1996;12(5):638–42.
20.ZhaoJX,ZhangLH,MaoZ,ZhangLC,ZhaoZ,SuXY,etal. Outcomeofposteriorcruciateligamentreconstructionusing thesingle-versusdoublebundletechnique:ameta-analysis. JIntMedRes.2015;43(2):149–60.
21.ChenCH,ChenWJ,ShihCH.Arthroscopicreconstructionof theposteriorcruciateligament:acomparisonofquadriceps tendonautograftandquadruplehamstringtendongraft. Arthroscopy.2002;18(6):603–12.
22.CuryRP,SeverinoNR,CamargoOPA,AiharaT,OliveiraVM, AvakianR.Reconstruc¸ãodoligamentocruzadoposteriorcom enxertoautólogodotendãodomúsculosemitendinosoduplo edoterc¸omédiodotendãodoquadrícepsemduplotúnelno fêmureúniconatíbia:resultadosclínicosemdoisanosde seguimento.RevBrasOrtop.2012;47(1):57–65.
23.CuryRPLC,MestrinerMB,KalekaCC,SeverinoNR,Oliveira VM,CamargoOP.Double-bundlePCLreconstructionusing autogenousquadricepstendonandsemitendinousgraft: surgicaltechniquewith2-yearfollow-upclinicalresults. Knee.2014;21(3):763–8.