w w w . r b o . o r g . b r
Original
Article
Evaluation
of
elbow
flexion
following
free
muscle
transfer
from
the
medial
gastrocnemius
or
transfer
from
the
latissimus
dorsi,
in
cases
of
traumatic
injury
of
the
brachial
plexus
夽
Frederico
Barra
de
Moraes
∗,
Mário
Yoshihide
Kwae,
Ricardo
Pereira
da
Silva,
Celmo
Celeno
Porto,
Daniel
de
Paiva
Magalhães,
Matheus
Veloso
Paulino
DepartmentofOrthopedicsandTraumatology,FaculdadedeMedicina,UniversidadeFederaldeGoiás(UFG),Goiânia,GO,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received24March2014 Accepted21October2014 Availableonline20October2015
Keywords:
Brachialplexus/surgery Muscle/transplant
Reconstructivesurgicalprocedures
a
b
s
t
r
a
c
t
Objective:Tocomparethegaininelbowflexioninpatientswithtraumaticinjuryofthe brachialplexusfollowingmuscletransferfromlatissimusdorsiwiththegainfollowingfree muscletransferfromthemedialbellyofthegastrocnemius.
Methods:Thiswasaretrospectivestudyinwhichthemedicalfilesofaconvenience sam-pleof13patientsoperatedbetween2000and2010werereviewed.Group1comprisedseven patientswhounderwenttransfersfromthegastrocnemiusandgroup2(controls)comprised sixpatientswhounderwenttransfersfromthelatissimusdorsi.Thefollowingfunctions wereevaluated:(1)rangeofmotion(ROM)ofelbowflexion,indegrees,usingmanual goniom-etryand(2)gradeofelbowflexionstrength,usingamusclestrength scale.Satisfactory resultsweredefinedas:(1)elbowflexionROM≥80◦and(2)elbowflexionstrength
≥M3.The
FisherexactandKruskal–Wallistestswereused(p<0.05).
Results:Thepatients’meanagewas32years(range:17–56)and72%hadbeeninvolvedin motorcycleaccidents.Elbowflexionstrength≥M3wasobservedinsevenpatients(100%)
ingroup1andinfivepatients(83.3%)ingroup2(p=0.462).Noneofthepatientspresented M5,andonepatient(16.7%)ingroup2hadapoorresult(M2).ElbowflexionROMwitha gain≥80◦
(dailyfunctions)wasfoundinsixpatients(86%)ingroup1andinthreepatients (50%)ingroup2(p=0.1).
Conclusion:Thepatientsingroup1hadgreatergainsinstrengthandROMthandidthosein group2,butwithoutstatisticalsignificance.Thus,transfersfromthegastrocnemiusbecome anewsurgicaloption,ifothertechniquescannotbeused.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
StudycarriedoutatHandandMicrosurgeryService,HospitaldasClínicas,UniversidadeFederaldeGoiás(UFG),Goiânia,GO,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](F.B.deMoraes).
http://dx.doi.org/10.1016/j.rboe.2015.09.007
Avaliac¸ão
da
flexão
do
cotovelo
após
transferência
muscular
livre
do
gastrocnêmio
medial
ou
transferência
do
latíssimo
do
dorso
na
lesão
traumática
do
plexo
braquial
Palavras-chave:
Plexobraquial/cirurgia Músculo/transplante Procedimentoscirúrgicos reconstrutivos
r
e
s
u
m
o
Objetivo: Compararoganhodeflexãodocotoveloempacientescomlesãotraumáticado plexobraquialapóstransferênciamusculardolatíssimodorsal(TMLD)comatransferência muscularlivredoventremedialdogastrocnêmio(TMLGM).
Metódos: Estudoretrospectivo,revisãodeprontuários,amostradeconveniência,com13 pacientesoperados,entre2000e2010.Grupo1(TMLGM)comsetepacientesegrupo2ou controle(TMLD)comseis.Func¸ãoavaliada:1)amplitudedemovimento(ADM)emgraus da flexãodocotovelo,goniometriamanual; 2)graude forc¸adeflexão docotovelo,por escaladeforc¸amuscular.Satisfatórios:1)ADM:flexãodocotovelo≥80◦
;2)Forc¸a:flexão docotovelo≥M3.TestesexatodeFishereKruskal–Wallis(p<0,05).
Resultados:Médiadeidadefoide32anos(17a56).Acidentedemotoem72%.Forc¸adeflexão docotovelo≥M3nogrupo1emsetepacientes(100%)eogrupo2emcinco(83,3%)(p=0,462).
NãotivemosM5eogrupo2apresentouumpaciente(16,7%)comresultadoruimM2.ADM naflexãodocotovelocomganho≥80◦
(func¸õesdiárias)foramencontradosnogrupo1em seispacientes(86%)enogrupo2emtrês(50%)(p=0,1).
Conclusão:Pacientesdogrupo1tiveramumganhomaiordeforc¸aeADM,quando compara-doscomosdogrupo2,semsignificadoestatístico.Assim,TMLGMsetornaumanovaopc¸ão cirúrgica,casonãopossamseraplicadasoutrastécnicas.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Traumaticbrachialplexusinjuries(BPIs)canhindertheelbow flexion function and thus dramatically alter the quality of lifeofindividuals.Veryoften,theinitialmicroneurosurgery cannotappropriatelyrestoremovementinthisjoint.Inolder injuries,nerverepairsurgeriesarenotrecommended,asthere isdefiniteatrophyandclassicmuscletransfers(MT)are pos-sible only in partial lesions. Thus, some patients require complementary interventions for functional gain of elbow flexion.Theseprocedures arerelated toMTorfreemuscle transfer(FMT).1
The MTs were the first techniques described. Steindler flexorplastyanduseofthelatissimusdorsi,pectoralismajor and triceps were the main types.2 The FMTs are newer and exhibit higher technicaldifficulty, due to the need to perform the neurovascular microanastomosis between the transplantedmuscle pedicleand the vesselsandnerves of the injurysite. Inthe upperlimb,and morespecifically to gainelbowflexion,thetechniquesusedaretheFMTofthe contralaterallatissimusdorsi(LD),rectusfemorisandgracilis muscles.1,3
Theliteraturehasonlythreestudiesconcerningthemedial gastrocnemius(MG)usedintheupperlimbforFMT,inorder torecoverthefunctionofaninjuredmusclegroup.Liuetal.4 useditforVolkmann’sischemiccontractureintheforearm, withgoodfunctionalresults.Serafin5proposedthattheMG wouldhavesignificantpotentialtorestoreelbowflexionor extension.Kwaeetal.6describedtheFMToftheMGtogain elbowflexioninpatientswithtraumaticBPI.
Theaimofthisstudywastocomparethegaininelbow flexioninpatientswithtraumaticBPIafterstandardsurgical procedureofMToftheLD(controlgroup)withFMToftheMG (studygroup).
Method
Retrospective study carried out by the review of medical recordsfromaconveniencesampleconsistingof13patients withtraumaticBPIthatwereconsecutivelysubmittedto sur-gicalprocedurefromDecember2000toDecember2010atthe HandandMicrosurgeryService.Thesepatientsweredivided intotwogroups.Group1orstudyconsistedofsevenpatients submittedtoFMToftheMGandgroup2orcontrolconsisted ofsixpatientssubmittedtoMToftheLD.
Patientsthatwereincludedinthetwogroupshadmuscle strengthequaltoM0(withoutstrength)anddegreeofelbow flexionbetween0and10◦ (nomovement),whohadalready
beensubmittedtosurgerywithothertechniques,but with-outsuccess,orthosethathadtheplexusinjuryforabouta yearandhadnotbeentreatedsurgically,withoutthe possi-bilityofapreviousneuralsurgery.Also,asinclusioncriteria, patientswithpreoperativeLDmuscleactivity≥M4were
cho-senfortheLDcontrolgroup,whilefortheMGstudygroup, patientswithLDstrength≤M3wereselected,asLDtransfer
wouldbecontraindicatedinthissituation.
Weexcluded patientsthathad incomplete dataintheir medicalrecords,orpreoperativestrength≥M1andelbow
Thedatacollectedfrommedicalrecordsconsistedofage, timeof injuryin months,neural injury level, typeof neu-raldamage,typeofmuscletransfer,typeofprevioussurgery, elbowflexionstrengthandrangeofmotionforbothpre-and postoperativeperiods.
Thelevel and type ofneurologic injurywere diagnosed bypreoperativeelectromyography.Asforelbowflexion,the degreeofmusclestrengthwasmeasuredbytheBritish Med-icalCouncil scale (M0=no movement;M1=onlya trace or flicker of movement is seen or felt, or fasciculations are observed;M2=musclecanonlymoveifresistanceofgravity isremoved;M3=jointcanbemovedonlyagainstgravitywith examiner’s resistance completely removed; M4=strength reduced,but contraction canstill movejoint against resis-tance;M5=normalstrength)andamanualgoniometerwas usedtomeasurerangeofmotion(ROM),startingfromzero degrees in total elbow extension to the maximum angle achievedandmaintainedbythepatient,oneyearafter mus-culartransfersurgery.
Ingroup1,theMGFMTwasperformedwiththe follow-ingsteps:(1)mediancurvilinearlongitudinalincision,which starts8cmproximaltothepoplitealcrease,extendsdistally upto10cmproximaltothemedialmalleolus;(2)dissection oftheintermuscularseptumbetweenthetwogastrocnemius bellies,laterallydisplacingthesmallsaphenousveinandthe sural nerve, individualizing the muscle and neurovascular structuresofthepoplitealfossa;(3)theoriginoftheMGisthen severedfromthefemoralmedialcondyleandthemedialsural neurovascularbundleisdissectedandclampedforresection, initslongestextension,1cmproximaltothejoint;(4) identifi-cationofthesciatic,medialpoplitealandtibialnerve(fromthe rootsofL4–L5/S1–S3ofthelumbosacralplexus),fromwhich thebranch totheMGoriginates, calledmedialsuralnerve (MSN),accordingtotheanatomicalmodeldescribedbyMoraes etal.7(5)identificationofthenumberofarterialandvenous branchesthatarriveattheMGpedicle,aswellasthecrossing ofthesmallsaphenousveinovertheMSN,whichmay hin-deritsdissection;(6)deltopectoralincisionandsubcutaneous dissectionintheupperlimbtowhereoneintendsto trans-fertheMGforbicepsfunctionwithdissectionoftheartery, thethoracodorsalveinandthecephalicvein;(7)MGFMTfor elbowflexion,withfixationoftheproximalventralregionat theproximalendofthehumerusthroughthebonewindow andfixationwithcorticalscrewsinthedistalregionofthe distalstumpofthebicepstendon;(8)microanastomosisofthe arterialbranchoftheMGinthethoracodorsalartery;theveins wereattached,oneinthethoracodorsalveinandanotherin thecephalicvein;(9)themicroanastomosisoftheMGMSN wascarriedoutindifferentperipheralbranches,with neuro-tizationstothemusculocutaneousfromtheulnar,intercostal oraccessorynerves.1,8,9
Oneofthe principlesof surgicalreconstructionof trau-matic BPIs is the recovery of elbow flexion. Thus, the following parameters are considered satisfactory: (1) ROM: elbowflexion≥80◦and(2)strength:elbowflexion≥M3.Group
2 consisted of patients submitted to ipsilateral latissimus dorsitransfer,whichwasperformedaspreviouslydescribed inliterature.1,2
Data were collected and stored in Excel for Windows andanalyzedusingthestatisticalsoftwareprogramSPSSfor
Windows,version13.0.AllsampleswereevaluatedbyFisher’s exacttestforparametricdataandKruskal–Wallistestfor non-parametricdata.Statisticalsignificancewassetatp≤0.05.
Results
Ofthe13patientsassessedtoimproveelbowflexionfunction aftertraumaticBPI,seven(54%)wereingroup1(free mus-cletransferofthemedialgastrocnemius),withameanlesion timeof18.4months(10–30),andsix(46%)ingroup2orcontrol (latissimusdorsitransfer),withameantimeoflesionof22.3 months(12–36).Allpatientsweremales.
Meanagewas32years(17–56).Therightsidewasaffected in seven(54%)casesand the left insix(46%). Sevencases (54%)werefromGoiâniaandsix(46%)fromthestateofGoiás countryside.Regardingwork,twopatients(15%)were unem-ployed,five(39%)didmanualworkandsix(46%)workedinthe administrativearea.
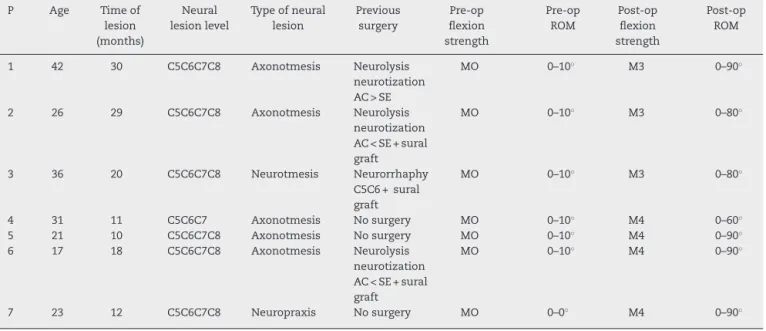
Motorcycle accidentwasthe causeoftheinjury innine patients(70%)(p<0.05);one(7.5%)casewasduetoautomobile accident,one(7.5%)casewashit byacar,one(7.5%)hada work-relatedaccidentandone(7.5%)wasduetofirearminjury. The clinical characteristics of patients in group 1 (MG) relatedtothetypeofbrachialplexusinjuryanditsevolution aftertreatmentareshowninTable1andthoseofgroup2(GD) areshowninTable2.
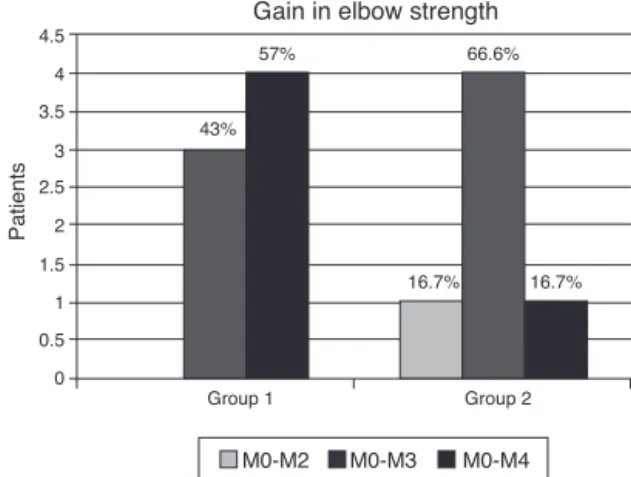
Regardinggainofstrengthinelbowflexion,weobserved thatbothgroupshadsatisfactoryresultswithagainequalto oraboveM3,group1withsevenpatients(100%)andgroup2 withfive(83.3%),butnosignificantdifference(p=0.462).There were noresultswithgainM5and group2hadonepatient (16.7%)withpoorresultsintermsofstrengthgain,whichonly achievedM2(Fig.1).
Regarding the rangeofmotiongainindegreesofelbow flexion,weobservedthatsatisfactoryresultswithgains>80◦
indailyfunctionswerefoundingroup1insixpatients(86%) andingroup2inthree(50%),butwithnosignificantdifference (p=0.1).Therewerenoresultswithgain>150◦.Regardingthe
resultsinwhichflexionwasonlyachievedupto60◦,therewas
onlyonepatient(14.3%)ingroup1andthreepatientsingroup 2(50%)(Fig.2).
57%
43%
16.7% 16.7%
66.6%
Group 1
Group 2 Gain in elbow strength 4.5
3.5
2.5
1.5
0.5 4
3
2
1
0
Patients
M0-M2 M0-M3 M0-M4
Table1–Clinicalcharacteristicsofpatientssubmittedtofreetransferfromthemedialgastrocnemiusmuscleforgainin elbowflexion(group1).
P Age Timeof
lesion (months)
Neural lesionlevel
Typeofneural lesion
Previous surgery
Pre-op flexion strength
Pre-op ROM
Post-op flexion strength
Post-op ROM
1 42 30 C5C6C7C8 Axonotmesis Neurolysis
neurotization AC>SE
MO 0–10◦ M3 0–90◦
2 26 29 C5C6C7C8 Axonotmesis Neurolysis
neurotization AC<SE+sural graft
MO 0–10◦ M3 0–80◦
3 36 20 C5C6C7C8 Neurotmesis Neurorrhaphy
C5C6+sural graft
MO 0–10◦ M3 0–80◦
4 31 11 C5C6C7 Axonotmesis Nosurgery MO 0–10◦ M4 0–60◦
5 21 10 C5C6C7C8 Axonotmesis Nosurgery MO 0–10◦ M4 0–90◦
6 17 18 C5C6C7C8 Axonotmesis Neurolysis
neurotization AC<SE+sural graft
MO 0–10◦ M4 0–90◦
7 23 12 C5C6C7C8 Neuropraxis Nosurgery MO 0–0◦ M4 0–90◦
Table2–Clinicalcharacteristicsofpatientssubmittedtomuscletransferfromlatissimusdorsiforelbowflexiongain (group2).
P Age Timeof
lesion (months)
Neural lesionlevel
Typeofneural lesion
Previous surgery
Pre-op flexion strength
Pre-op ROM
Post-op flexion strength
Post-op ROM
1 32 36 C5C6 Axonotmesis Neurolysis
neurotization AC<SE+sural graft
MO 0–10◦ M3 0–90◦
2 56 23 C5C6 Neurotmesis Neurolysis
neurotization AC<SE+sural graft+oberain
MO 0–10◦ M2 0–30◦
3 23 18 C5C6C7 Neurotmesis Nosurgery MO 0–10◦ M3 0–80◦
4 50 19 C5C6C7C8 Axonotmesis Neurolysis
neurotization AC<SE+sural graftoberain
MO 0–10◦ M3 0–60◦
5 39 12 C5C6 Axonotmesis NeurolysisC5C6 MO 0–10◦ M4 0–120◦
6 31 26 C5C6 Axonotmesis Neurolysis
neurotization AC<SE+sural graft+oberain
MO 0–10◦ M3 0–60◦
Discussion
Elbowflexionimprovementinpatients withtraumaticBPIs providesanimportantgainintheinjuredlimbfunctionand anelbowconsideredadequateistheonewithstrength≥ M3,
ideally≥M4and withmorethan 80◦ ofactiveflexion.2 The
MTsaremainlyindicatedincaseswherethepatienthashad apartialinjuryoronlyintheuppertrunk(C5C6)orshowsgood handandwristfunction.
TheFMThaveawiderrangeofpossibilities,butwithfar greatertechnicaldifficulties.Forthehandtoworkadequately, theshouldermustbestableandtheelbowmusthave ade-quateflexion–extensionactivity,topositionitinthespace.9 Otherwisethelimbwillbecomenonfunctional.Bothinthe
MTorFMTforelbowrecovery,regardlessofthechosen tech-nique,theelbowjointcannotbeankylosedorcontractedand thechosenmusclemusthaveM4orM5strength.
TheMT from the tricepsto thebiceps isconsidered by Steindler10asunsatisfactory,asitcanaffectelbowextension. Thetricepshasanimportantfunctionintheupperlimband, therefore,theMTshouldbeusedonlyasalastresort. Accord-ingtosomeauthors,suchasPardinietal.11theyuseitdueto thetechnicalsimplicity,aswellasbecausethisMTisableto allowthepatienttomovethehandtotheheadandmouth withsatisfactoryflexionofaround120◦andprovidesmuscle
strengthtosupportuptothreeandahalfkilograms.
4.5
4
3
2
1 3.5
2.5
1.5
0.5
0
Group 1 Group 2
Patients
0-30 degrees 0-60 degrees 0-80 degrees
0-90 degrees 0-120 degrees
57%
28.7%
14.3% 16.7%
33.2%
16.7%
16.7% 16.7%
Gain in elbow range of motion
Fig.2–Assessmentofgaininelbowflexionrangeof motionbetweenthegroups.
portions are used. Itsmain contraindication in relation to other MTs is damageto the axillaryartery, which impairs thethoracoacromialartery.However,itisnotthefirstoption either,asthepectoralismajorispartoftheshouldergirdle andmaybeusedforshoulderrecoveryanditsresultsarenot satisfactoryformostpatients,whoendupattainingonly60◦
ofelbowflexioninaverageandwithlittlestrength.12 Steindlerflexorplasty10 wasthe first procedureused for rehabilitationoftheparalyzedelbow.Itwasinitiallyapplied inpatientswithpoliosequelae,obstetricalandarthrogrypotic paralysis and onlylater in traumatic BPI. That MT is per-formedbyfreeing the medialelbowepicondylealong with flexor–pronatormusclesoftheforearm(pronatorteres,flexor carpiradialis,palmarislongus,flexordigitorumsuperficialis and flexorcarpi ulnaris)and thensubsequently fixation to amoreproximalportionofthehumerus.Itiscurrentlyone ofthemostwidelyusedtechniques, asitissimpleto per-formandcanattainmorethan100◦ ofelbowflexionin70%
ofpatients.However,itsdisadvantagesareadecreaseinthe flexingstrengthofthehandandwrist;objectscanberaised onlyiftheyweightuptotwokilogramsandthecontractureof elbowjoint.13
However,it isthemainMTusedforelbowrecoveryand from the latissimus dorsi to the ipsilateral biceps, where the results can reach over 100◦ of active elbow flexion
and M4 strength. The latissimus dorsi can be transferred inunipolar or bipolar mannerand the main contraindica-tion isthelackofanadequate postoperativerehabilitation program.14
AsfortheFMT,themostoftenusedmuscleisthe contralat-erallatissimusdorsi15–17followedbythegracilis(GD)fromthe lowerlimb,andrarelytherectusfemoris.1Theindicationfor aFMTcomesfromtheneedtorestoreelbowflexionfunction intraumaticBPIs,evenafterneurosurgicalproceduresinthe plexus,orincasesthatarereferredfortreatmentafterone year.TheFMTwillnotbenecessarywhenscienceisableto maintainthe morphologyand ultrastructureofdenervated musclemakeneuralgraftsdirectlyontothespinalcordand acceleratetheneuronalregenerationvelocity.18
ThegracilisFMTcanbeperformedasasingleprocedure togainelbowflexionfunctionorasdualproceduretoattain elbowflexionandatthesametimeimprovehandfunction and shoulder stability. When it isused onlytogain elbow flexion, approximately 80% of patients reach M4 strength, but when usedasdualfunction, this numberdecreases to 60%.19–21
Accordingtotheliterature,22–26theMGhasattractive fea-turesforFMT,suchas:length,excursioncapacity,contraction forceproportionaltothesectionalarea,longinsertional ten-don, adequate neurovascular bundle(blood supply classI), puremotorbranchoftheMSNfromthemedialpoplitealnerve (95%singlebranch).
Otheradvantagesare:resectionofonlyonegastrocnemius belly,whichdoesnotaffecttheplantflexionfunctionanddoes notcausemajordeformity.ThescarleftbytheMGremoval is cosmeticallyacceptable, especiallyin men. Moreover,in patientsthatmaybesubmittedtolocaltransfers,theMGFMT hastheadvantageofaddinganothermusclegrouptoa weak-enedupperlimb,aimingatbetterfunction.Thedisadvantages are: thescars inwomen; thesupineposition makesit dif-ficulttodissectatthedonorsite(poplitealfossa)inFMTto upperlimb.Optionally,theprocedurecanbeperformedwith thepatientinthelateraldecubitusposition.
WebelievethattheanastomosisoftheMSNwithpartof theulnarshowedbetterperformancethanwiththeintercostal nerve,duetotheshorterreinnervationdistance.However,the useoftheintercostalnervecanbeconsideredanoptionifthe ulnarisnotavailable.
TheMGFMTtobicepshadnotbeenperformed,untilthen, forthispurpose.ThusKuwaeetal.6describedintwocasesthe MGFMTforelbowflexionfunctionrecoveryinpatientswith traumaticBPIs.Inourstudy,weobservedgoodresults≥M3in
100%ofMGFMTand85.6%inGDMTandexcellentresults withM4in57%oftheMGFMTand29%inGDMT,butwithout significantdifference.Regardingtheelbowrangeofmotion, flexionexceeded80◦in85.6%ofpatientsundergoingMGFMT
andin57%ofpatientssubmittedtoGDMT.Thisdifference wasnotsignificantbetweenthegroups.
Whencomparingtheresultsofthetwogroups,therewas nodifferenceinelbowflexiongain.Patientssubmittedtofree transferofthemedialgastrocnemiusmusclehadahighergain instrengthandROMwhencomparedwiththecontrolgroup submittedtolatissimusdorsitransfer,butwithoutstatistical significance.Thus,MGFMTcanbeconsideredatechniqueof whichresultsarenotinferiortothoseoftheLDMTstandard techniqueand becomesaviableoptionifother techniques cannotbeapplied.
Conclusion
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. VekrisMD,BerisAE,LykissasMG,KorompiliasAV,VekrisAD,
SoucacosPN.Restorationofelbowfunctioninseverebrachial
plexusparalysisviamuscletransfers.Injury.2008;39Suppl
3:S15–22.
2. BengtsonKA,SpinnerRJ,BishopAT,KaufmanKR,
Coleman-WoodK,KircherMF,etal.Measuringoutcomesin
adultbrachialplexusreconstruction.HandClin.
2008;24(4):401–15.
3. BarrieKA,SteinmannSP,ShinAY,SpinnerRJ,BishopAT.
Gracilisfreemuscletransferforrestorationoffunctionafter
completebrachialplexusavulsion.NeurosurgFocus.
2004;16(5):E8.
4. LiuXY,GeBF,WinYM,JingH.Freemedialgastrocnemius
myocutaneousflaptransferwithneurovascularanastomosis
totreatVolkmann’scontractureoftheforearm.BrJPlast
Surg.1992;45(1):6–8.
5. SerafinD.Thegastrocnemiusflap.In:SerafinD,editor.Atlas
ofmicrosurgicalcompositetissuetransplantation.
Philadelphia:Saunders;1996.p.303–10.
6. KuwaeMY,MoraesFB,ParanahybaRM,OliveiraE.
Transferênciamuscularlivrefuncionaldogastrocnêmio
medialemlesãodoplexobraquial:relatodedoiscasos.Rev
BrasOrtop.2007;42(1):37–40.
7. MoraesFB,OliveiraE,ParanahybaRM,KwaeMY,RochaVL.
Estudoanatômicodomúsculogastrocnêmiomedialvisando
transferênciamuscularlivre.RevBrasOrtop.
2007;42(1/2):37–40.
8. HattoriY,DoiK,BaliarsingAS.Apartoftheulnarnerveasan
alternativedonornerveforfunctioningfreemuscletransfer:
acasereport.JHandSurgAm.2002;27(1):150–3.
9. AkasakaY,HaraT,TakahashiM.Freemuscletransplantation
combinedwithintercostalnervecrossingforreconstruction
ofelbowflexionandwristextensioninbrachialplexus
injuries.Microsurgery.1991;12(5):346–51.
10.SteindlerA.MuscleandTendontransplantationattheelbow.
In:ArborA,EdwardsJW,editors.Instructionalcourselectures
onreconstructivesurgery.AnnArbor:JWEdwards;1944.
p.276–83.
11.PardiniAG,FreitasAL,FreitasAD,TavaresKE.Transferências
tendinosasparaflexãodocotovelo.RevBrasOrtop.
1996;31(3):211–6.
12.HiernerR,BergerA.Pectoralismajormuscletransferfor
reconstructionofelbowflexioninposttraumaticbrachial
plexuslesions.OperOrthopTraumatol.2009;21(2):
126–40.
13.Al-QattanMM.ElbowflexionreconstructionbySteindler
flexorplastyinobstetricbrachialplexuspalsy.JHandSurgBr.
2005;30(4):424–7.
14.KawamuraK,YajimaH,TomitaY,KobataY,ShigematsuK,
TakakuraY.Restorationofelbowfunctionwithpedicled
latissimusdorsimyocutaneousflaptransfer.JShoulderElbow
Surg.2007;16(1):84–90.
15.HovnanianAP.Latissimusdorsitransplantationforlossof
flexionorextensionattheelbow;apreliminaryreporton
technic.AnnSurg.1956;143(4):493–9.
16.OberlinC.Brachialplexuspalsyinadultswithradicular
lesions,generalconcepts,diagnosticapproach,andresults.
ChirMain.2003;22(6):273–84.
17.TerzisJK,KostopoulosVK.Thesurgicaltreatmentofbrachial
plexusinjuriesinadults.PlastReconstrSurg.
2007;119(4):73e–92e.
18.BishopAT.Functioningfree-muscletransferforbrachial
plexusinjury.HandClin.2005;21(1):91–102.
19.DoiK,MuramatsuK,HattoriY,OtsukaK,TanSH,NandaV,
etal.Restorationofprehensionwiththedoublefreemuscle
techniquefollowingcompleteavulsionofthebrachialplexus.
Indicationsandlong-termresults.JBoneJointSurgAm.
2000;82(5):652–66.
20.ChungDC,CarverN,WeiFC.Resultsoffunctioningfree
muscletransplantationforelbowflexion.JHandSurgAm.
1996;21(6):1071–7.
21.SalibianAH,RogersFR,LambRC.Microvascular
gastrocnemiusmuscletransfertothedistallegusing
saphenousveingrafts.PlastReconstrSurg.1984;73(2):
302–7.
22.SmrckaV,StinglJ,KubinK,MoravecZ.Anatomicalnoteson
gastrocnemiusmuscleusesformuscleflappreparation.Acta
ChirPlast.1986;28(2):112–20.
23.MairesseJL,MestdaghH,ProcykS,DepreuxR.Contributionà
l’étudedelavascularisationartérielledumuscletriceps
sural.AnatAnz.1984;155(1–5):195–202.
24.DibbellDG,EdstromLE.Thegastrocnemiusmyocutaneous
flap.ClinPlastSurg.1980;7(1):45–50.
25.McCrawJB,FishmanJH,SharzerLA.Theversatile
gastrocnemiusmyocutaneousflap.PlastReconstrSurg.
1978;62(1):15–23.
26.ArnoldPG,MixterRC.Makingthemostofthegastrocnemius