w w w . r b o . o r g . b r
Original
Article
Assessment
of
spontaneous
correction
of
lumbar
curve
after
fusion
of
the
main
thoracic
in
Lenke
1
adolescent
idiopathic
scoliosis
夽
Danilo
Mizusaki
∗,
Alberto
Ofenhejm
Gotfryd
IrmandadedaSantaCasadaMisericórdiadeSantos,Santos,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received17December2014 Accepted23March2015 Availableonline13January2016
Keywords:
Scoliosis Bonescrews Treatmentoutcome
a
b
s
t
r
a
c
t
Objective:To evaluate the clinicalandradiographic responseof the lumbarcurve after fusionofthemainthoracic,inpatientswithadolescentidiopathicscoliosisofLenketype1.
Methods:Forty-twopatientswithLenke1adolescentidiopathicscoliosiswhounderwent operationsviatheposteriorroutewithpediclescrewswereprospectivelyevaluated.Clinical measurements(sizeofthehumpandtranslationofthetrunkinthecoronalplane,bymeans ofaplumbline)andradiographicmeasurements(Cobbangle,distallevelofarthrodesis, translation ofthelumbarapicalvertebralandRisser)weremade.Theevaluationswere performedpreoperatively,immediatelypostoperativelyandtwoyearsaftersurgery.
Results:ThemeanCobbangleofthemainthoraciccurvewasfoundtohavebeencorrected by68.9%andthelumbarcurveby57.1%.Eightypercentofthepatientspresentedimproved coronaltrunkbalancetwoyearsaftersurgery.Infourpatients,worseningoftheplumb linemeasurementswasobserved,buttherewasnoneedforsurgicalintervention.Less satisfactoryresultswereobservedinpatientswithlumbarmodifierB.
Conclusions: InLenke1patients,fusionofthethoraciccurvealoneprovidedspontaneous correctionofthe lumbarcurve andledtotrunkbalance.Lesssatisfactoryresultswere observedincurveswithlumbarmodifierB,andthismayberelatedtoovercorrectionof themainthoraciccurve.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Avaliac¸ão
da
correc¸ão
espontânea
da
curva
lombar
após
a
fusão
da
torácica
principal
na
escoliose
idiopática
do
adolescente
Lenke
1
Palavras-chave:
Escoliose
r
e
s
u
m
o
Objetivo:Avaliararespostaclínicaeradiográficadacurvalombarapósafusãodatorácica principal,empacientescomescolioseidiopáticadoadolescente(EIA)Lenke1.
夽
WorkperformedintheSpineGroup,DepartmentofOrthopedicsandTraumatology,SantaCasadaMisericórdiadeSantos,Santos,SP, Brazil.
∗ Correspondingauthor.
E-mail:[email protected](D.Mizusaki).
http://dx.doi.org/10.1016/j.rboe.2015.03.013
Parafusosósseos Resultadodetratamento
Métodos: Foramavaliadosprospectivamente42pacientesportadoresdeEIAtipoLenke1 operadospor viaposteriorcomparafusospediculares.Fizeram-semensurac¸õesclínicas (tamanhodagibaetranslac¸ãodotronconoplanocoronalpelofiodeprumo)eradiográficas (ângulodeCobb,níveldistaldaartrodese,translac¸ãodavértebraapicallombareRisser).As avaliac¸õesforamfeitasnopré-operatório,pós-operatórioimediato(POI)edoisanosapósa cirurgia.
Resultados: Foiobservadacorrec¸ãode68,9%,emmédia,doângulodeCobbdacurvatorácica principal(TPR)e57,1%dalombar.Oitentaporcentodospacientesapresentarammelhora doequilíbriocoronaldotronco,doisanosapósacirurgia.Emquatropacientesfoiobservada pioradosvaloresdamedidadofiodeprumo,sem,entretanto,havernecessidadedenova intervenc¸ãocirúrgica.Osresultadosmenossatisfatóriosforamobservadosempacientes commodificadorlombarB.
Conclusões:EmpacientesLenke1,afusãoexclusivadacurvatorácicaproporcionoucorrec¸ão espontâneadacurvalombarecompensac¸ãodotronco.Osresultadosmenossatisfatórios foram observadosem curvascommodificador lombarBe podem estarrelacionados à hipercorrec¸ãodacurvatorácicaprincipal.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Incasesofadolescentidiopathicscoliosis,theaimof surgi-caltreatmentistoprovidecompensationforthetrunkand vertebralfusionforcurvaturethatisconsideredtobe struc-tured.Forthis,thecurvatureisdeterminedinaccordancewith thepreoperativeradiographicflexibility,andthisguidesthe planningofthelevelsthataretoundergoarthrodesis.King etal.1introducedtheconceptofselectivethoracicarthrodesis
incasesthatwerenamed“falsedoublecurves”.Thisconcept hasbeenrefinedoverrecentdecades,especiallyconsequent tothepaperpublishedbyRichardsin1992.2
In2001,Lenkeetal.3publishedatwo-dimensional
classifi-cationofadolescentidiopathicscoliosis.Inthis,thecurvature isgroupedintosixmaintypesandisalsodescribedinterms oflumbarandsagittalmodifiers.LenketypeIisthemost fre-quentclassification,andthisonlypresentsstructuringofthe mainthoraciccurve (TPR). Thereisa consensusinthe lit-eraturethattype1Acurvatureshouldonlyreceivefusionof themainthoraciccurve.However,intypesBandC, inclu-sionofthelumbarcurvature(TL/L)isamatterofcontroversy. Moreover, with the evolution of operative techniques and instrumentsthathavegreatercorrectivepower,ithasbeen observedthatgreaterinteresthasbeentakeninidentifying factorsthatpredictequilibriumoriatrogenicdecompensation ofthetrunkafterselectivefusionofthespine.
Theobjectiveofthepresentstudywastoevaluatethe clin-icalandradiographiccorrectionoflumbarcurvatureandits predictivefactors,afteronlyperformingfusionofthethoracic curveinpatientswithLenke1adolescentidiopathicscoliosis.
Materials
and
methods
Thisstudywasapprovedbytheinstitutionalresearchethics committee of the Catholic University of Santos (UNISAN-TOS)underthenumberCAAE31602014.4.0000.5536.Forty-two patientswithadolescentidiopathicscoliosispresenting cur-vaturegreater than 40◦ who underwent spinal arthrodesis
participatedinthisstudy.Theywereevaluatedclinicallyand radiographicallyinaprospectivemanner:beforethe opera-tion,immediatelyaftertheoperation(10daysafterwards)and aftertwoyearsoffollowup.Allthepatientswereoperatedby thesameseniorsurgeon.Theclinicalandradiographic evalu-ationswereperformedbymembersofthemedicalteamwho didnothavedirectparticipationintheresearch.
Thefollowingindividualswereconsideredtobewithinthe inclusioncriteria:bothgenders;thosewithLenketype1 ado-lescentidiopathicscoliosis;thoseoperatedbetweentheages of11and18years;thosewithCobbanglesbetween40◦ and 90◦4;andthosewhounderwentarthrodesisofthemain
tho-racicspinebymeansofaposterioraccessroute,usingpedicle screws.Patientswhorequiredpreoperativetractionordistal fusionatL1andthosewhosedatawereincompletelyfilledout wereexcluded.
Theclassificationofthecurvesfollowedthecriteria pro-posedbyLenkeetal.3Inthis,thecurveswereclassifiedinto
sixmaintypes,accordingtotheirstructuring,andwerealso describedintermsofalumbarmodifier(relationshipbetween acentral-sacralverticallineandthelumbarapicalvertebra) andasagittalmodifier(kyphosisbetweenT5andT12).
CorrectionoftheTPRfollowedtheprinciplesofderotation oftheconcavitywitharodbymeansofthetechniqueofCotrel andDubousset.5Thismethodwasusedincaseswithlumbar
curvewasused,inordertominimizetheriskofiatrogenic decompensationofthetrunk.
ThecriteriaofSuketal.6wereusedtodeterminethefusion
level.Thus, whenadifference ofup totwolevels between theneutralvertebraandtheterminalvertebrawasobserved, fusionwasperformedasfarastheneutralvertebraandwhen thisdifferencewithgreaterthantwolevels,fusionwasdone as far as one vertebra before the neutral vertebra. Radio-graphsoftheentirespinewereproducedonpanoramicfilm (90cm×30cm),inanteroposteriorview(AP),lateralview(P) andactivesupinelateralobliqueanteroposteriorview.7 The
followingparameterswere evaluated aspossiblepredictive factors for trunkcompensation: Cobb angles of the proxi-malthoraciccurve(TPX),TPRandTL/L4;Rissersign8;distal
levelofthearthrodesis;andtranslationofthelumbarapical vertebra.9Thepercentagecorrectionofthecurveswas
calcu-latedinaccordancewiththeformulaproposedbySuketal.6:
Cobb pré-operatório−Cobb pós-operatório
Cobb pré-operatório ×100
Preoperative Cobb−postoperativeCobb
Preoperative Cobb ×100
Afterthis,ratiobetweentheCobbangleofthemain tho-raciccurvatureandthethoracolumbar/lumbarcurvaturewas calculated.
Theclinical measurementscomprisedthetranslation of thetrunkinthecoronalplane,measuredusingaplumbline (ScoliosisResearchSociety)10andthesizeofthelumbarhump
(cm).Thesemeasurementsweremadeduringamaneuverof anteriorinclinationofthetrunk.11
Statisticalanalysis
Thepatients’qualitativecharacteristicswereevaluatedand weredescribedusingabsoluteandrelativefrequencies.Their quantitativecharacteristics were described using summary measurements(mean,standarddeviation,median,minimum andmaximum).
Thepreoperativeandpostoperativescalesweredescribed usingsummarymeasurementsandwerecomparedbetween the timesusing paired Wilcoxon tests.12 Thescales
evalu-atedbefore the operation, inthe immediatepostoperative periodandtwoyearsaftertheoperationweredescribedand comparedusingFriedman tests,12 followedbythe multiple
nonparametric comparisonsforpaired datathat were pro-posedbyNetteretal.13
Spearmancorrelationswerecalculatedbetweenthescales relatingtotwoyearsaftertheoperationinordertoascertain correlationsinthefinalresultsfromthepatients,betweenthe scales.12
Measurements oftrunk equilibriumusing a plumb line weredescribed,alongwiththoracolumbar/lumbarCobbangle values.Afterthis,thesevalueswerecorrelatedwiththedistal anatomicallevelofthearthrodesis(instrumenteddistal verte-bra),bymeansoftheMann–Whitneytest.12Thepreoperative
andpostoperativeplumblinevaluesandthescaleofplumb linechangeswerecomparedwiththethreetypesoflumbar modifiersofLenkeetal.,bymeansoftheKruskal–Wallistest.12
Thetestswereperformedwithasignificancelevelof5%.
Results
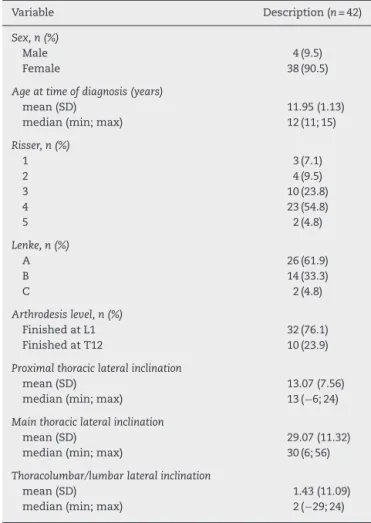
Amongthe42patientsincludedinthisstudy,4(9.5%)were maleand38(90.5%)werefemale;55%presentedtype4Risser signatthetimeofthesurgery.Theirmeanagewas11.9years and61.9%presentedlumbarAmodifier,33.3%presentedBand 4.8%presentedC.TheinstrumenteddistalvertebrawasT12 in23.9%andL1in76.1%(Table1).
ThemeanCobbangleoftheTPXwas24.69◦(SD7.34)and thelateralinclinationwas13.07(SD7.56).Intheimmediate postoperativeperiod,themeanTPXcurvaturewas12.57(SD 6.84)anditwas12.64(SD6.89)twoyearsafterthesurgery.A meancorrectionof48.8%wasobserved.
Forthemainthoraciccurvature(TPR)beforetheoperation, themeanwas58.10◦(SD9.23)andthelateralinclinationwas 29.07◦(SD11.32).Intheimmediatepostoperativeperiod,the meanvalueobservedwas15.90◦(SD6.46),whileitwas18.02◦ (SD6.91)twoyearsaftertheprocedure,i.e.animprovement of68.9%.
The thoracolumbar/lumbarcurvature (TL/L) presenteda meanof34.57◦ (SD9.18)beforetheoperation,withalateral inclinationof8.07◦(SD11.09).Intheimmediatepostoperative period,thevalueobservedwas12.05◦(SD8.36)andaftertwo
Table1–Generalcharacteristicsofthesample.
Variable Description(n=42)
Sex,n(%)
Male 4(9.5)
Female 38(90.5)
Ageattimeofdiagnosis(years)
mean(SD) 11.95(1.13)
median(min;max) 12(11;15)
Risser,n(%)
1 3(7.1)
2 4(9.5)
3 10(23.8)
4 23(54.8)
5 2(4.8)
Lenke,n(%)
A 26(61.9)
B 14(33.3)
C 2(4.8)
Arthrodesislevel,n(%)
FinishedatL1 32(76.1)
FinishedatT12 10(23.9)
Proximalthoraciclateralinclination
mean(SD) 13.07(7.56)
median(min;max) 13(−6;24)
Mainthoraciclateralinclination
mean(SD) 29.07(11.32)
median(min;max) 30(6;56)
Thoracolumbar/lumbarlateralinclination
mean(SD) 1.43(11.09)
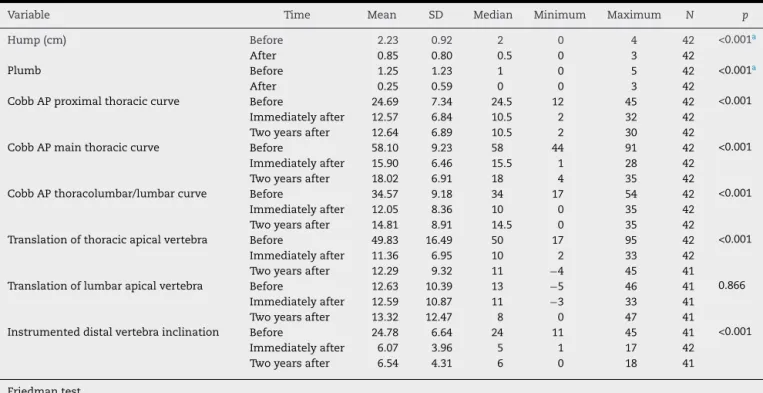
Table2–Resultsfromtestscomparingbeforeandaftertheoperation.
Variable Time Mean SD Median Minimum Maximum N p
Hump(cm) Before 2.23 0.92 2 0 4 42 <0.001a
After 0.85 0.80 0.5 0 3 42
Plumb Before 1.25 1.23 1 0 5 42 <0.001a
After 0.25 0.59 0 0 3 42
CobbAPproximalthoraciccurve Before 24.69 7.34 24.5 12 45 42 <0.001 Immediatelyafter 12.57 6.84 10.5 2 32 42
Twoyearsafter 12.64 6.89 10.5 2 30 42
CobbAPmainthoraciccurve Before 58.10 9.23 58 44 91 42 <0.001 Immediatelyafter 15.90 6.46 15.5 1 28 42
Twoyearsafter 18.02 6.91 18 4 35 42
CobbAPthoracolumbar/lumbarcurve Before 34.57 9.18 34 17 54 42 <0.001 Immediatelyafter 12.05 8.36 10 0 35 42
Twoyearsafter 14.81 8.91 14.5 0 35 42
Translationofthoracicapicalvertebra Before 49.83 16.49 50 17 95 42 <0.001 Immediatelyafter 11.36 6.95 10 2 33 42
Twoyearsafter 12.29 9.32 11 −4 45 41 Translationoflumbarapicalvertebra Before 12.63 10.39 13 −5 46 41 0.866
Immediatelyafter 12.59 10.87 11 −3 33 41 Twoyearsafter 13.32 12.47 8 0 47 41
Instrumenteddistalvertebrainclination Before 24.78 6.64 24 11 45 41 <0.001 Immediatelyafter 6.07 3.96 5 1 17 42
Twoyearsafter 6.54 4.31 6 0 18 41
Friedmantest.
a PairedWilcoxontest.
yearsitwas14.81(SD8.91),whichrepresentedspontaneous correctionofthelumbarcurvatureof57.1%.
Thepreoperativethoracichumpwas2.23cm(SD0.92)and it was 0.85cm (SD 0.80) two years after the operation, i.e. animprovementof 61.8%(p<0.001).The mean plumbline measurementwas1.25cm(SD1.23)beforetheoperationand 0.25cm(SD0.59)afterthesurgicalprocedure,i.e.an improve-mentof80%(p<0.001).
Thetranslationofthelumbarapicalvertebrawastheonly parameteranalyzedthatdidnotpresentanystatistically sig-nificantimprovement(p=0.866)(Table2).
Itwasobservedthattherewerestatisticallysignificant dif-ferencesfortheTPX,TPRandTL/Lcurvature,incomparing thepreandpostoperativevalues(p<0.001).TheTPRandTL/L
curvatures presentedangularworsening regardingthe val-uesobtainedintheimmediatepostoperativeperiodandtwo yearsaftertheoperation(p=0.006andp=0.005,respectively) (Table3).
Fourpatientspresentedworseningoftheirtrunk equilib-rium, as measured using a plumb line. Of these,two also presentedincreasedlumbarhumps.Thesecaseswere clas-sified as Lenke A (one patient) and B (three patients). A descriptionoftherelationshipbetweentrunkcompensation andthelumbarmodifierispresentedinTables4and5.
Alsoinrelationtoclinicalmeasurementsonthe lumbar hump,accordingtoeachsubtypeofthelumbarmodifier(A, BorC),weobservedthattherewasnostatisticaldifference betweenthegroups,aspresentedinTable6.
Table3–Comparisonsbetweentheevaluationtimes.
Variable Comparison Zvalue p
Table4–ChangeinplumbaccordingtothelumbarmodifiersofLenkeetal.
Changeinplumb Lenke p
A B C Total
N % n % n % n %
Worsened 1 3.8 3 21.4 0 0.0 4 9.5 0.097
Nochange 4 15.4 4 28.6 1 50.0 9 21.4
Improved 21 80.8 7 50.0 1 50.0 29 69.0
Total 26 100 14 100 2 100 42 100
Kruskal–Wallistest.
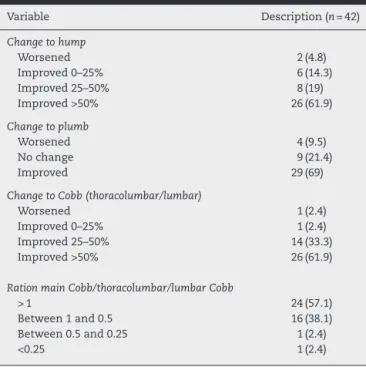
Table5–Gradingofthechangestotheparameters evaluated.
Variable Description(n=42)
Changetohump
Worsened 2(4.8)
Improved0–25% 6(14.3)
Improved25–50% 8(19)
Improved>50% 26(61.9)
Changetoplumb
Worsened 4(9.5)
Nochange 9(21.4)
Improved 29(69)
ChangetoCobb(thoracolumbar/lumbar)
Worsened 1(2.4)
Improved0–25% 1(2.4)
Improved25–50% 14(33.3) Improved>50% 26(61.9)
RationmainCobb/thoracolumbar/lumbarCobb
>1 24(57.1)
Between1and0.5 16(38.1) Between0.5and0.25 1(2.4)
<0.25 1(2.4)
TherelationshipsoftheplumblineandtheCobbTL/Lwith thelast instrumentedvertebraare presentedinTable7.In this,it can beseen that the distallevel ofthe arthrodesis (T12orL10)didnotinfluencetheplumblinemeasurementsor theCobbthoracolumbar/lumbarangle(p=0.479andp=0.194, respectively).
Discussion
Theaimsofsurgicaltreatmentofadolescentidiopathic sco-liosisaretocorrectthedeformity,restoretrunkequilibrium
andimplementarthrodesisonthesmallestnumberofspinal segmentspossible.14
Selectivethoracicfusionforavoidingunnecessaryfusion offlexiblelumbarcurveswasdescribedbyKingetal.1
Sev-eralarticleshavedemonstratedacapacitytoaccommodate lumbarcurvatureinrelationtothoraciccurvature,with main-tenanceoftheoverallalignment.14–16However,insomecases,
theremaybeinsufficientaccommodationofthelumbarcurve andunsatisfactoryestheticresults.Theprognosticfactorsfor accommodationofthelumbarcurvaturearenotfully estab-lishedinthecurrentliterature.
Inthepresentstudy,aspontaneousreductionintheCobb angle ofthe lumbar curvature of 57% was observed. This valueissimilartowhatwasreportedbyLenkeetal.14 and
was greater than what was described by Parisini et al.15
(54.8%) and Peelle (50%).16 However, it was observed two
years afterthe operationthat therehad been a significant increase in the lumbar Cobb angle (p=0.005). This obser-vation is contrary to previous descriptions, in which the spontaneouslumbarcorrectionwasseentobedynamicand the improvement would occur within the first two years after the surgery.14,17,18 However,we observedthat despite
radiographicworsening,nosignificantclinicaldeterioration was observed.Thiscanbeexplainedbythe factthatthere was proportional accommodationofthe instrumentedTPR curve, which maintained the angular ratio between the curves.
Thetranslationoftheinstrumenteddistalvertebra meas-uresthedisplacementofthespinefromthemidline.Forthe lumbarspine,nostatisticaldifferencefrombeforetoafterthe surgerywasobserved.Thiscouldhavebeenexpected,given thatthemajorityofthecurvesincludedwereofLenketype AorBandpresentedlesscoronaltranslationduringthe pre-operativeperiod.Therefore,thesepresentedlesspotentialfor surgicalcorrection.
Table6–Descriptionofclinicalplumblinemeasurementsbeforeandaftertheoperation,inaccordancewithLenkeetal., andtheresultsfromcomparativetests.
Variable Lenke Mean SD Median Minimum Maximum N p
Plumbbefore A 1.52 1.35 1 0 5 26 0.093
B 0.71 0.87 0.5 0 2.5 14
C 1.50 0.71 1.5 1 2 2
Plumbafter A 0.19 0.43 0 0 2 26 0.604
B 0.32 0.82 0 0 3 14
Table7–ComparisonbetweenlastinstrumentedvertebraandchangestoplumbandCobbTL/L.
Variable Arthrodesislevel p
FinishedatL1 FinishedatT12 Total
N % n % n %
Changetoplumb 0.479
Worsened 2 6.2 2 20.0 4 9.6
Nochange 5 15.7 1 10.0 6 14.2
Improved 25 78.1 7 70.0 32 76.2
Changetothoracolumbar/lumbarCobb 0.194
Worsened 0 0.0 1 10.0 1 2.3
Improved0–25% 1 3.1 0 0.0 1 2.3
Improved25–50% 9 28.1 4 40.0 13 31.1
Improved>50% 22 68.8 5 50.0 27 64.3
Total 32 100 10 100 42 100
Mann–Whitneytest.
Consideringtheclinicalalterationsinrelationtothesize ofthethoracichump,therewasareductionofapproximately 62%afterthesurgery.Sincenothoracoplastywasperformed, weattributetheclinicalimprovementtothecapacityforaxial correctionpresentedbythesurgicaltechniquethatwasused. However,thecorrectioninthisplanewasnottheaimofthe presentstudyanditmightbebetterexplainedthrough
com-putedtomographyevaluations.Regardingthelumbarhump,
althoughthe studiesavailableare limitedtothose compar-inganteriorandposterioraccessroutes,theresultsfromthe presentsampleweresimilartothoseofNewtonetal.19(50%),
butwerelowerthanthoseofLiljenqvistetal.20(63%).
Plumblinemeasurementsareanimportantparameterin surgicaltreatmentforadolescentidiopathicscoliosis.21Inour
study,animprovementinthisparameterof80%wasobtained aftertheoperation,whichwasgreaterthanorsimilartowhat wasfound byParisiniet al.(52%±8.7)15 and byLiljenqvist
etal.20(77.7%).However,therewerefourcasesinwhichthere
wasaworseningofthecoronalequilibriumofthetrunk.Twoof thesepatientspresentedassociatedworseningofthethoracic hump.Amongthecasesinwhichtherewasclinicalworsening, threewereclassifiedashavinglumbarBmodifier.
AspreviouslydescribedbyLenkeetal.22andKingetal.,1
choosingastablevertebraasthedistalfusionlevelprovided trunkequilibriuminmostcases. Inaddition, noclinicalor radiographicdifferenceswereobservedbetweenpatientsfor whomthe instrumenteddistalvertebrawasT12 andthose forwhomitwasL1.
AccordingtoBridwelletal.,23thederotationmaneuvermay
evolvetowarddecompensationofthecompensatorycurves. ThisisgenerallycausedbyovercorrectionoftheTPRand inca-pacityforlumbaraccommodation.Itcanbeexplainedbythe factthatcurveswithlumbartypeBmodifiersometimeshave behaviorsimilartothatoftypeC,14whichmaynotbe
recog-nizedbeforetheoperation.
Thestrongpointsofthepresentstudywerethatithada prospectivedesignandthat ahomogenousgroup ofLenke 1patientswas selected.However,thefactthatmostofthe patientsanalyzedwereclassifiedashavinglumbarA modi-fier,andmuchsmallernumbershadsubtypeBandespecially subtypeC,canbeconsideredtobealimitation.
Conclusion
1. Arthrodesisperformedsolelyonthemainthoracic curva-tureinLenke1patientsprovidedspontaneouscorrectionof thelumbarcurvatureandconsequentcoronalequilibrium ofthetrunk.
2. Theleastsatisfactoryresultswereobservedincaseswith lumbarBmodifierandthesemayhavebeenrelatedto over-correctionofthemainthoraciccurvature.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.KingHA,MoeJH,BradfordDS,WinterRB.Theselectionof fusionlevelsinthoracicidiopathicscoliosis.JBoneJointSurg Am.1983;65(9):1302–13.
2.RichardsBS.LumbarcurveresponseintypeIIidiopathic scoliosisafterposteriorinstrumentationofthethoracic curve.Spine(Phila,PA1976).1992;17Suppl.8:S282–6.
3.LenkeLG,BetzRR,HarmsJ,BridwellKH,ClementsDH,Lowe TG,etal.Adolescentidiopathicscoliosis:anewclassification todetermineextentofspinalarthrodesis.JBoneJointSurg Am.2001;83(8):1169–81.
4.CobbJR.Outlineforthestudyofscoliosis.InstrCourseLect. 1948;5:261–75.
5.CotrelY,DuboussetJ.Anewtechnicforsegmentalspinal osteosynthesisusingtheposteriorapproach.RevChirOrthop ReparatriceApparMot.1984;70(6):489–94.
6.SukSI,LeeCK,KimWJ,ChungYJ,ParkYB.Segmentalpedicle screwfixationinthetreatmentofthoracicidiopathic scoliosis.Spine(Phila,PA1976).1995;20(12):1399–405.
7.GotfrydAO,FranzinFJ,PolettoPR,LauraAS,SilvaLCF. Radiografiaseminclinac¸ãolateralcomofatorpreditivoda correc¸ãocirúrgicanaescolioseidiopáticadoadolescente.Rev BrasOrtop.2011;46(5):572–6.
9. LenkeLG,BridwellKH,BaldusC,BlankeK.Preventing decompensationinKingtypeIIcurvestreatedwith Cotrel–Duboussetinstrumentation.Strictguidelinesfor selectivethoracicfusion.Spine(Phila,PA1976).1992;178 Suppl.:S274–81.
10.ScoliosisResearchSociety[online].Adolescentidiopathic scoliosis.Disponívelem:http://www.srs.org/
professionals/education/adolescent/idiopathic.
11.LonsteinJE.Avaliac¸ãodopaciente.EscoliosedeMoeeoutras deformidadesdacoluna.Traduc¸ãodeTerezinhaOppido,2nd ed.SãoPaulo:Santos;1994.p.47–88.
12.KirkwoodBR,SterneJA.Essentialmedicalstatistics.2nded. Massachusetts,USA:BlackwellScience;2006.
13.NeterJ,KutnerMH,NacthsheimCJ,WassermanW.Applied linearstatisticalmodels.4thed.IL,Irwin:McGraw-HillHigher Education;1996.
14.LenkeLG,BetzRR,BridwellKH,HarmsJ,ClementsDH,Lowe TG.Spontaneouslumbarcurvecoronalcorrectionafter selectiveanteriororposteriorthoracicfusioninadolescent idiopathicscoliosis.Spine(Phila,PA1976).
1999;24(16):1663–71.
15.ParisiniP,DiSilvestreM,LolliF,BakaloudisG.Selective thoracicsurgeryintheLenketype1A:KingIIIandKingIV typecurves.EurSpineJ.2009;18Suppl.1:82–8.
16.PeelleMW,Boachie-AdjeiO,CharlesG,KanazawaY,MesfinA. Lumbarcurveresponsetoselectivethoracicfusioninadult idiopathicscoliosis.SpineJ.2008;8(6):
897–903.
17.DobbsMB,LenkeLG,WaltonT,PeelleM,DellaRoccaG, Steger-MayK,etal.Canwepredicttheultimatelumbarcurve inadolescentidiopathicscoliosispatientsundergoinga selectivefusionwithundercorrectionofthethoraciccurve? Spine(Phila,PA1976).2004;29(3):277–85.
18.ChangKW,ChangKI,WuCM.Enhancedcapacityfor spontaneouscorrectionoflumbarcurveinthetreatmentof majorthoracic-compensatoryCmodifierlumbarcurve patterninidiopathicscoliosis.Spine(Phila,PA1976). 2007;32(26):3020–9.
19.NewtonPO,MarksMC,BastromTP,BetzR,ClementsD, LonnerB,etal.SurgicaltreatmentofLenke1mainthoracic idiopathicscoliosis:resultsofaprospective,multicenter study.Spine(Phila,PA1976).2013;38(4):328–38.
20.LiljenqvistU,HalmH,BullmannV.Spontaneouslumbar curvecorrectioninselectiveanteriorinstrumentationand fusionofidiopathicthoracicscoliosisofLenketypeC.Eur SpineJ.2013;22Suppl.2:S138–48.
21.MajdoulineY,AubinCE,RobitailleM,SarwarkJF,LabelleH. Scoliosiscorrectionobjectivesinadolescentidiopathic scoliosis.JPediatrOrthop.2007;27(7):775–81.
22.LenkeLG,BridwellKH,BaldusC,BlankeK,SchoeneckerPL. Cotrel–Duboussetinstrumentationforadolescentidiopathic scoliosis.JBoneJointSurgAm.1992;74(7):1056–67.