ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Determinants
of
quality
of
life
in
Paget’s
disease
of
bone
Gláucio
Ricardo
Werner
de
Castro
a,b,∗,
Silvania
Ana
Fernandes
de
Castro
c,d,
Ivanio
Alves
Pereira
a,e,
Adriana
Fontes
Zimmermann
b,e,
Maria
Amazile
Toscano
f,
Fabricio
Souza
Neves
e,
Maria
Aparecida
Scottini
a,
Juliane
Paupitz
b,
Julia
Salvan
da
Rosa
g,
Ziliani
Buss
g,
Tânia
Silvia
Fröde
gaUniversidadedoSuldeSantaCatarina,FaculdadedeMedicina,Palhoc¸a,SC,Brazil bHospitalGovernadorCelsoRamos,UnidadedeReumatologia,Florianópolis,SC,Brazil cUniversidadedoValedoItajaí,FaculdadedePsicologia,Itajaí,SC,Brazil
dUniversidadedoSuldeSantaCatarina,FaculdadedeFisioterapia,Tubarão,SC,Brazil
eUniversidadeFederaldeSantaCatarina,HospitalUniversitário,UnidadedeReumatologia,Florianópolis,SC,Brazil fCentroCatarinensedeReabilitac¸ão,Florianópolis,SC,Brazil
gUniversidadeFederaldeSantaCatarina,CentrodeCiênciasdaSaúde,DepartamentodeAnálisesClínicas,Florianópolis,SC,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received6June2016 Accepted26April2017
Availableonline28September2017
Keywords:
Paget’sdiseaseofbone Qualityoflife
SF-36 WHOQOL-bref
a
b
s
t
r
a
c
t
Objective:ToevaluatetheparametersassociatedwithqualityoflifeinpatientswithPaget’s diseaseofbone.
Methods:PatientswithPaget’sdiseaseofbonewereevaluatedwithSF-36andWHOQOL-bref questionnaires.Patientswithotherdiseasesthatcouldcausesignificantimpairmentoftheir qualityoflifewereexcluded.Wesearchedforcorrelationsbetweentheresultsand:age,time fromdiagnosis,typeofinvolvement,painrelatedtoPaget’sdiseaseofbone,limitationto dailyactivities,deformities,bonespecificalkalinephosphatase,theextentofinvolvement andtreatment.
Results:Fiftypatientswereincluded.ResultsoftheSF-36totalscoreanditsdomains, physi-calandmentalhealth,weresignificantlycorrelatedwithbonepainanddeformities.Marital statuswassignificantlycorrelatedwiththeSF-36totalscoreandMentalHealthDomain.BAP levelsanddiseaseextensionweresignificantlycorrelatedtoSF-36PhysicalHealthDomain. Aftermultivariateanalysis,theonlyparametersthatremainedsignificantlyassociatedwith theSF-36totalscoreandtoitsMentalHealthandPhysicalHealthDomainswerepainand maritalstatus.
TheWHOQOL-breftotalscorewassignificantlyassociatedwithpain,physicalimpairment anddeformities.WHOQOL-brefDomain1(physical)scorewassignificantlyassociatedwith maritalstatus,painanddeformities,whileDomain2(psychological)scorewasassociated withmaritalstatus,physicalimpairmentandkindofinvolvement.Aftermultivariate anal-ysis,thepresenceofpain,deformities,andmaritalstatusweresignificantlyassociatedwith
∗ Correspondingauthor.
E-mail:[email protected](G.R.WernerdeCastro). https://doi.org/10.1016/j.rbre.2017.06.002
resultsoftheWHOQOL-breftotalscoreanditsDomain1.WHOQOL-brefdomain2results weresignificantlypredictedbypainandmaritalstatus.
Conclusion: Themaindisease-relatedfactorassociatedwithSF-36resultsinPaget’sdisease ofbonepatientswasbonepain,whilebonepainanddeformitieswereassociatedwith WHOQOL-bref.
©2017ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Determinantes
da
qualidade
de
vida
na
doenc¸a
de
Paget
óssea
Palavras-chave:
Doenc¸adePagetóssea Qualidadedevida SF-36
WHOQOL-bref
r
e
s
u
m
o
Objetivo: Avaliarosparâmetrosassociadosàqualidadedevidaempacientescomdoenc¸a dePagetóssea(DPO).
Métodos: Avaliaram-sepacientescomDPOcomosquestionáriosSF-36eWHOQOL-bref. Excluíram-sepacientescomoutrasdoenc¸asquepudessemcausarcomprometimento sig-nificativodaqualidadedevida.Buscou-seporcorrelac¸õesentreosresultadoseidade,tempo dediagnóstico,tipodeenvolvimento,dorrelacionadacomaDPO,limitac¸ãoàsatividades diárias,deformidades,fosfatasealcalinaespecíficadoosso,extensãodoenvolvimentoe tratamento.
Resultados: Incluíram-se50pacientes.Osresultadosdapontuac¸ãototaldoSF-36eseus domínios,saúdefísicaesaúdemental,secorrelacionaramsignificativamentecomador ósseaedeformidades.Oestadocivilsecorrelacionousignificativamentecomapontuac¸ão totaldoSF-36ecomseudomíniosaúdemental.OsníveisdeBAPeaextensãodadoenc¸ase correlacionaramsignificativamentecomodomíniosaúdefísicadoSF-36.Depoisdaanálise multivariada,osúnicosparâmetros quepermaneceramsignificativamenteassociadosà pontuac¸ãototaldoSF-36eaosseusdomíniossaúdementalesaúdefísicaforamadoreo estadocivil.Apontuac¸ãototaldoWHOQOL-brefestevesignificativamenteassociadaàdor, aocomprometimentofísicoeadeformidades.OescoredoDomínio1(físico)do WHOQOL-brefestevesignificativamenteassociadoaoestadocivil,doredeformidades,enquantoo Domínio2(psicológico)esteveassociadoaoestadocivil,comprometimentofísicoetipode envolvimento.Depoisdaanálisemultivariada,apresenc¸adedor,deformidadeseestado civilestevesignificativamenteassociadaàpontuac¸ãototaldoWHOQOL-brefeàpontuac¸ão doseuDomínio1.OsresultadosdoWHOQOL-bref2foramsignificativamentepreditospela dorepeloestadocivil.
Conclusão: OprincipalfatorassociadoaosescoresdoSF-36foiadoróssea,enquantoador ósseaeasdeformidadesestiveramassociadasaoWHOQOL-bref.
©2017ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Paget’sdisease of bone(PDB) isa common osteometabolic disease characterized by increased and disorganized bone turnover.Itisusuallyasymptomaticbutmaycausebonepain, fractures, deformities, secondary osteoarthritis, neurologic and cardiac complications and,in rare cases, neoplasm.1,2
Thesecomplicationscanadverselyaffectthequalityoflife (QoL)ofthesymptomaticPDBpatient.Therefore,studies eval-uatingQoLinPDBpatientsandtheeffectsofPDBtreatment inQoLhavebeenpublished.3–10
FewofthesestudieshavefocusedondeterminantsofQoL inthispopulation,butthisknowledgeisimportantinthe eval-uationoftreatmenteffectsonQoL.Iftheparametersrelated withpoorQoLareaffectedbycurrentlyavailabletreatments, anincreaseinQoLisexpectedafterthetreatment. Onthe otherhand,ifsomeimportantparametersarenotinfluenced
by PDB’s treatment, then, measures of QoL would have a limitedroleintheevaluationofdifferenttherapeuticoptions. Thiscouldhelptounderstandtheheterogeneousresultsof PDBtreatmentinQoLindifferentstudies.4,5,10
Thepresentstudywasundertakentoevaluateparameters associatedwithQoLinPDBpatients.
Methods
ofthelowerlimb,fibromyalgia,neurologicalsyndromesnot dueto PDB,acute orchronic infections,peripheral arterial insufficiency,ischemiccardiacdisease,heartfailure,chronic pulmonarydiseases,renalorhepaticinsufficiency,neoplasm andosteoporoticfractures.
PDB and osteoarthritis were diagnosed by typical find-ingsonradiographs.Diseaseactivitywasevaluatedby99mTc MDPbonescintigraphy;apatientwasconsideredtohavethe diseaseifarecentbonescintigraphyshowshighuptake sug-gestiveofPDBandotherpossiblediagnosiswereexcludedby x-raysoranothercomputedtomography.Diseaseextension wasevaluatedbyX-raysandbonescintigraphy,previousand recent.Themethoddescribed byMeunieretal.11 wasused
tocalculatediseaseextensiononbonescintigraphy.Analysis ofbonescintigraphywasdonewithoutidentificationofthe patientordate.
Apatientwasconsideredtobeincurrenttreatmentifhe hadusedoralbisphosphonates(alendronate,risedronateor ibandronate)inthepastsixmonthsorzoledronicacidinthe previous 12 months. Fasting blood samples were collected fordeterminationofbone-specificalkalinephosphatase(BAP) byenzyme-linkedimmunosorbentassay (Mybiosource, San Diego,CA,ref.MBS724100).
Patientswereallowedtotakeparacetamolordipyronefor pain,ifnecessary,accordingtotheirregularprescriptions.
PatientswereaskedtoanswertotheBrazilianversionsof SF-3612andWHOQOL-bref13questionnaires.TheSF-36scores
werecalculatedasdescribedbyKalantar-Zadehetal.14 The
questionnaireswereadministeredbyarheumatologist,once perpatient.Resultswerefurthercomparedamongsubgroups definedbyclinicalcharacteristics andcorrelated todisease activityandextensionparameters.Thelocalethical commit-teeapprovedthe studyprotocol (protocolnumber 353,461). Allsubjectssignedaninformedconsentform;thisstudywas conductedbytheprinciplesoftheDeclarationofHelsinki.15
Statisticalanalysis
Statisticalanalysiswascarriedouttoverifyifdisease-related factors could influence QoL in PDB patients. Comparisons of subgroups defined according to clinical characteristics weremadewithMann–WhitneyUtest.Correlationsbetween continuousvariableswereanalyzedbySpearman’srho corre-lation.Generalizedlinearmodelregressionwasusedtoassess the association between the results of QoL tests and PDB parameters.ParameterssignificantlyassociatedtoQoLon uni-variateanalysisaswellasparameterstheoreticallyassociated withdecreased QoLwere entered inthe regression model. Resultsare presented asmean (SD)or median (25–75 per-centiles).
StatisticalanalysiswasperformedwithSPSS20.0,witha levelofsignificanceof0.05.
Results
Seventy-sevenPDB patientswerescreened,and50patients wereincluded. Reasonsforexclusionsarelisted inTable1. Subjectsweremainlywomen(60.8%),Caucasian(96.8%)and married(80.6%).Theyhad amean ageof66.32±8.65years
Table1–Reasonsforexclusionof27of77patientswith Paget’sdiseaseofbonefromthepresentstudy.Some patientshavemorethanonereasonforexclusion.
Number Frequency(%)
Alzheimer’sdisease 2 2.4
Chronicrenaldisease 1 1.2
Primaryosteoarthritisoftheknee 1 1.2
Psoriasicarthritis 1 1.2
Ankylosingspondylitis 1 1.2
Degenerativelumbarstenosis 1 1.2
Fibromyalgia 9 10.3
Ischemicheartdisease 3 3.8
Unabletoanswer 1 1.2
Peripheralarterydisease 1 1.2
Hepaticcirrhosis 1 1.2
Prostatecâncer 1 1.2
Peripheralpolyneuropathy 1 1.2
Parkinson’sdisease 2 2.4
Depression 1 1.2
Refusetoanswer 1 1.2
andhad7.69±6.15yearsfromdiagnosis.Mostsubjectshad apolyostotic disease (74.2%)and29% hadapositive famil-ialhistory.41.9%wereconsideredtobeinactivetreatment, and 38.7% were regardedas havingactivedisease onbone scintigraphy. No patient has taken calcitonin, intravenous ibandronate or pamidronate in the past 12 months. Bone pain relateddoPDB atany momentwasreportedby56.9% ofsubjects,butonly32.3%hadcurrentbonepain,19.4%had deformities secondary to PDB, 12.9% any physical impair-mentsduetoPDBand32.3%hadosteoarthritisconsideredto besecondarytoPDB(Table2).
SF-36
ThemediantotalscoreintheSF-36questionnairewas60.91 (38.81–78.54),themedianscoreofPhysicalhealthcomponent was62.60(38.20–75.80),andofthementalhealthcomponent was59.70(41.30–79.90).ResultsoftheSF-36totalscoreand itsPhysicalhealthandMentalHealthcomponentswerenot significantlydifferentwhensubjectsweredividedaccording tosex,kindofinvolvement(monostoticorpolyostotic), cur-rentdiseaseactivity,currenttreatmentofPDB,thepresence ofphysicalimpairmentsduetoPDB,thepresenceofsecondary osteoarthritis.Resultsofthe SF-36 totalscoreand both its physicalandmentalhealthDomainsweresignificantly differ-entwhenpatientswerecategorizedaccordingtocurrentbone pain(p:0.027,0.008and0.15,respectively)anddeformities sec-ondarytoPDB(p:0.011,0.012and0.017,respectively).Marital statuswassignificantlycorrelatedwiththeSF-36totalscore andMentalHealthDomain(p:0.046and0.016,respectively), butnotwithPhysicalHealthDomain(Table3).BAPlevelsand diseaseextensionweresignificantlycorrelatedtoSF-36 Phys-icalHealthDomain(p:0.038and0.03,respectively),butnotto SF-36totalscoreorMentalHealthDomain.Timefrom diagno-siswasneitherassociatedwithSF-36totalscorenortoanyof itsdomains(Table4).
Table2–Clinicalcharacteristicsof50patientswithPaget’sdiseaseofbone.Resultsareexpressedinpercentageorin mean(DP).
Age(years) 66.32(8.65)
Gender
Female 60.8%
Male 39.2%
Race
Caucasian 96.8%
Afrobrazilian 3.2%
Maritalstatus
Married 80.6%
Singleorwidowed 19.4%
FormofPDB
Monostotic 25.8%
Polyostotic 74.2%
Timefromdiagnosis(years) 7.69(6.15)
PositivefamilialhistoryofPDB 29%
Currentactivityonscintigraphya 38.7%
CurrenttreatmentofPDBb 41.9%
Diseaseextensionc 2.21(2.70)
BAPlevels(U/L) 33.78(42.83)
Bonepain(current) 32.3%
Deformitiesd 19.4%
ImpairmentduetoPDBe 12.9%
Deafnessf 3.2%
Intracranialhypertensionf 3.2%
OsteoarthritissecondarytoPDBg 32.3%
FracturesecondarytoPDBh 3.2%
Osteosarcoma 0
PDB,Paget’sdiseaseofbone;BAP,bone-specificalkalinephosphatase. a Definedbyareasofhighuptakeonbonescintigraphy.
b Useoforalbisphosphonatesinthepast6monthsorzoledronicacidinthepast12months.
c Definedbyareaofhighuptakeonbonescintigraphy.
d Onclinicalexaminationandonradiographs.
e DefinedbylimitedarticularrangeofmotionduetoPDB.
f DuetocranialinvolvementbyPDB.
g OsteoarthritisinjointswithboneinvolvementbyPDB.
h InboneinvolvedbyPDB.
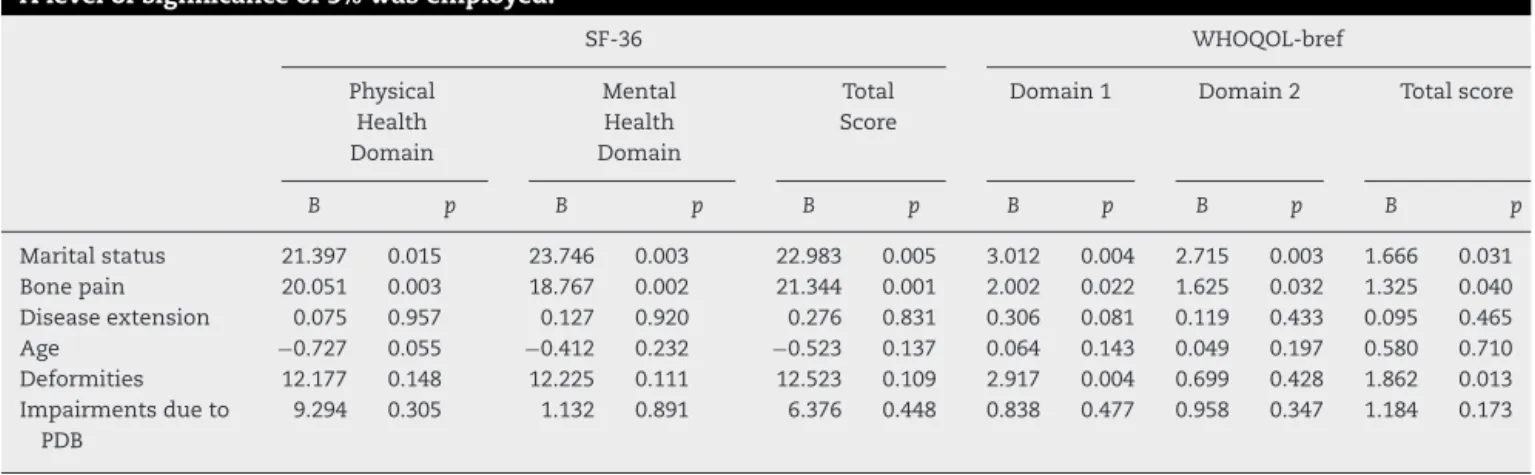
andthepresenceofimpairments.BAPlevelswereexcluded becausetheywere correlated withdiseaseextension (Pear-soncorrelationr:0.673,p<0.001).Afterregression,theonly parametersthat remainedsignificantlyassociatedwiththe SF-36totalscoreandtoitsMentalHealthandPhysicalHealth Domainswerepainandmaritalstatus(valueofpfor, respec-tively,pain:0.001,0.002and0.003;maritalstatus:0.005,0.003 and0.015)(Table5).
WHOQOL-bref
MedianscoreoftheWHOQOL-brefquestionnairewas14,61 (13.03–15.69).Resultsofits domainswere:domain 1 (phys-icalfunction):14.28(12.00–16.14),domain 2(psychological): 14.66 (13.81–17.33), domain 3 (social relationship): 15.33 (13.33–16.00),domain4(environment):14.5(12.89–16.00).The whoqol-breftotalscorewassignificantlyassociatedwithpain, physicalimpairment and presenceofdeformities(p: 0.019, 0.016,0.006,respectively).Itwasnotassociatedwithsex, mar-italstatus,diseaseactivity,currenttreatment,thepresenceof
secondaryosteoarthritisorkindofinvolvement(monostotic or polyostotic)(Table 3). Therewas no correlationbetween WHOQOL-brefscoreand:BAP,age,timefrom diagnosisand diseaseextension(Table4).
ConcerningtoWHOQOL-brefdomains,onlytheresultsof physical(domain1)andthepsychological(domain2) compo-nentswerefurtheranalyzed.Domain1scorewassignificantly associatedwithmaritalstatus,painanddeformities,(p:0.042, 0.011,0.010,respectively)butnotwithsex,physical impair-ment,kindofinvolvementorosteoarthritis,diseaseactivity orcurrenttreatment.Medianresultsofdomain2scoreswere associatedwithmaritalstatus,physicalimpairment,andkind ofinvolvement(p:0.029, 0.021, 0.031, respectively),but not withsexpain, currenttreatment, disease activity, deformi-tiesandosteoarthritis(Table3).WHOQOL-brefdomains1and 2werenotassociatedtoBAP,age,timefromdiagnosis and diseaseextension(Table4).
Table3–ResultsofthequestionnairesSF-36andWHOQOL-brefin50PDBpatientsdividedaccordingtoclinical
characteristics.Resultsareexpressedinmedian(25%and75%percentiles).Alevelofsignificanceof5%wasemployedin
Mann–WhitneyUtest.
SF-36 WHOQOL-bref
Physical Health Domain
Mental Health Domain
Total Score
Domain1 Domain2 Total
score
Gender
Female 50.60(38.20–72.80) 59.70(38.80–80.90) 60.27(38.81–75.68) 14.28(11.42–15.42) 14.66(12.66–16.66) 14.83(12.92–15.69) Male 73.80(36.60–82.80) 68.56(41.30–79.90) 75.93(35.43–80.18) 13.71(10.28–15.42) 15.33(14.00–17.33) 14.30(13.07–16.46)
p 0.316 0.707 0.506 0.674 0.325 0.897
Maritalstatus
Married 61.10(40.80–75.80) 65.25(42.7–80.90) 63.48(40.81–79.00) 14.28(12.00–16.00) 15.33(14.00–17.33) 14.61(13.53–15.69)
Sin-gle/widowed
44.80(30.20–59.60) 38.50(35.46–59.70) 45.29(31.06–60.91) 11.42(10.29–12.57) 13.33(12.00–14.66) 12.76(11.84–14.92)
p 0.097 0.016 0.046 0.042 0.029 0.092
FormofPDB
Polyostotic 69.60(41.20–82.80) 60.80(41.30–71.90) 75.68(38.81–76.12) 14.85(13.14–15.42) 16.66(14.66–17.33) 15.46(14.38–16.30) Monostotic 50.40(38.20–73.80) 56.63(41.30–71.90) 60.07(40.56–76.12) 14.00(10.29–15.42) 14.66(12.66–15.33) 14.22(12.64–15.23)
p 0.159 0.313 0.285 0.252 0.031 0.069
Currentactivityonscintigraphya
Yes 46.40(30.20–69.60) 53.45(38.50–81.80) 47.37(35.43–75.93) 13.71(10.29–15.43) 14.66(12.66–16.66) 14.53(11.84–15.69) No 66.80(48.00–75.80) 63.60(50.36–75.50) 62.10(47.85–79.18) 14.28(11.71–15.42) 14.99(14.66–17.33) 14.76(13.80–15.84)
p 0.114 0.213 0.131 0.384 0.220 0.257
CurrenttreatmentofPDBb
Yes 55.10(40.80–75.6) 60.41(43.20–79.90) 60.59(40.81–79.18) 13.71(11.42–14.28) 14.66(14.00–15.33) 14.22(13.07–15.07) No 63.6(36.6–76.8) 56.70(38.80–74.06) 61.31(38.50–78.41) 14.85(11.14–16.00) 15.33(13.33–17.33) 15.03(13.15–16.46)
p 0.894 0.594 0.581 0.147 0.322 0.324
Bonepain(current)
Yes 42.20(29.4–64.60) 43.20(38.50–56.00) 47.00(32.16–60.91) 11.43(10.29–14.28) 14.66(12.66–15.33) 13.38(11.84–14.92) No 69.60(44.80–77.80) 68.39(51.80–81.80) 72.71(47–79.18) 14.86(12.57–16.00) 15.33(14.00–17.33) 14.92(14.15–16.46)
p 0.027 0.008 0.015 0.011 0.123 0.019
DeformitiesduetoPDBc
Yes 40.70(24.30–45.80) 40.38(32.21–48.63) 40.68(27.31–46.57) 10.00(9.43–12.57) 13.66(12.00–16.33) 12.45(11.22–13.84) No 64.60(41.20–77.80) 61.13(43.20–80.90) 62.10(47.00–79.18) 14.28(12.00–15.43) 14.99(14.00–17.33) 14.92(13.60–16.15)
p 0.011 0.012 0.017 0.010 0.302 0.006
ImpairmentduetoPDBd
Yes 43.50(34.80–48.00) 53.28(41.30–59.70) 47.42(35.43–54.70) 11.71(9.71–12.57) 13.00(12.66–14.66) 12.78(12.00–13.07) No 64.60(40.60–76.80) 60.80(42.36–80.90) 62.10(40.56–79.00) 14.28(11.42–15.71) 15.33(14.00–17.33) 14.87(13.56–15.92)
p 0.113 0.268 0.151 0.053 0.021 0.016
OsteoarthritissecondarytoPDBe
Yes 41.40(31.00–73.20) 46.53(36.31–73.68) 43.78(33.50–78.70) 11.42(9.71–15.42) 14.66(12.66–17.33) 14.15(11.84–15.53) No 63.10(40.80–77.80) 67.56(46.90–81.80) 65.90(40.80–80.35) 14.28(11.43–16.00) 14.93(14.00–16.66) 14.61(13.38–15.69)
p 0.281 0.195 0.195 0.204 0.935 0.544
PDB,Paget’sdiseaseofbone.
a Definedbyareasofhighuptakeonbonescintigraphs.
b Useoforalbisphosphonatesinthepast6monthsorzoledronicacidinthepast12months. c Onclinicalexaminationandonradiographs.
dDefinedbylimitedarticularrangeofmotionduetoPDB.
e OsteoarthritisinjointswithboneinvolvementbyPDB.
WHOQOL-breftotalscoreand itsDomain1inregression(p
results,respectively:totalscore:0.040,0.013,0.031;domain1: 0.022,0.004,0.004).WHOQOL-brefdomain2resultswere sig-nificantlypredictedbypainandmaritalstatus(p:0.032and 0.003,respectively)(Table5).
ResultsofSF36 totalscoreand WHOQol-breftotal score werewellcorrelated(r:0.741,p<0.001).
Discussion
Table4–CorrelationofcontinuousvariablesandresultsofSF-36andWHO-QOL-brefanalyzedbySperman’srho correlationandexpressedascoefficientofcorrelationin50patientswithPaget’sdiseaseofbone.Alevelofsignificance
of5%wasemployed.
SF-36 WHOQOL-bref
Physical Health Domain
Mental Health Domain
Total Score
Domain1 Domain2 Totalscore
r p r p r p r p r p r p
Age(years) −0.123 0.396 −0.092 0.523 −0.47 0.744 0.008 0.956 0.069 0.637 0.094 0.519 Timefromdiagnosis
(years)
−0.20 0.891 −0.136 0.341 −0.54 0.708 0.001 0.995 −0.080 0.580 −0.051 0.723
Diseaseextensiona −0.308 0.030 −0.255 0.074 −0.276 0.052 −0.167 0.250 −0.089 0.542 −0.205 0.157 BAPlevels(U/L) −0.307 0.038 −0.226 0.131 −0.272 0.068 −0.226 0.131 −0.256 0.087 −0.257 0.085
BAP,bone-specificalcalinephosphatase.
a Definedbyareaofhighuptakeonbonescintigraphy.
Table5–MultivariateanalysisofSF-36andWHOQOL-brefresults.Resultsareexpressedasparameterestimates(B). Alevelofsignificanceof5%wasemployed.
SF-36 WHOQOL-bref
Physical Health Domain
Mental Health Domain
Total Score
Domain1 Domain2 Totalscore
B p B p B p B p B p B p
Maritalstatus 21.397 0.015 23.746 0.003 22.983 0.005 3.012 0.004 2.715 0.003 1.666 0.031
Bonepain 20.051 0.003 18.767 0.002 21.344 0.001 2.002 0.022 1.625 0.032 1.325 0.040
Diseaseextension 0.075 0.957 0.127 0.920 0.276 0.831 0.306 0.081 0.119 0.433 0.095 0.465
Age −0.727 0.055 −0.412 0.232 −0.523 0.137 0.064 0.143 0.049 0.197 0.580 0.710
Deformities 12.177 0.148 12.225 0.111 12.523 0.109 2.917 0.004 0.699 0.428 1.862 0.013 Impairmentsdueto
PDB
9.294 0.305 1.132 0.891 6.376 0.448 0.838 0.477 0.958 0.347 1.184 0.173
these extremes, many patients experience manifestations thatcould impair their QoL,suchas bonepain, secondary osteoarthritis,fractures,peripheralnervecompressionsand hearimpairment.1,2
InthefirststudytoevaluateQoLinthispopulation,Gold etal.9 havefoundthatthemajorityofPDBpatients
consid-eredthattheydidnothavegoodQoL. However,thatstudy didnotemployastandardizedquestionnaireand,althougha highnumberofsubjectswere evaluated,asignificant num-berofthemhadPDBcomplicationsorcomorbiditiesthatcan adverselyaffectQoL.
Otherstudies haveevaluatedQoLinPDB patientsusing the SF-36 questionnaire.3,6,8 In general, thesestudies have
reportedreducedQoLinthispopulation,butonlyoneofthem hassearchedforpredictorsofQoL.Langstonetal.3havefound
thatbonepain,ageandpreviousbisphosphonatetreatment predicted SF-36 Physical Health Domain, whilethe Mental HealthDomainwaspredictedbypriorbisphosphonate treat-ment,notbeingmarriedandbonepain.Resultsofthepresent studyareinlinewiththesefindingssincebothQoLscoreswere predictedbybonepainandmaritalstatusandBAPlevelswere notcorrelatedwithQoL.However,inourstudy,WHOQOL-bref resultswerealsopredictedbydeformities.
Both questionnairesemployedinthis study have deter-minedmaritalstatusandpainasdeterminantsofQoLinPDB. Thisresultwasexpectedsincetheseareclassicdeterminants
of QoL. However, deformities, in spiteof being reasonable causes of decreased QoL, only appeared as determinants ofWHOQOL-brefresults. Thisdiscrepancymightbedueto intrinsiccharacteristicsisofthequestionnaires,which eval-uation isbeyondthe scopeofthis study.However,the fact thepredictorfactorswerealmostthesameforboth question-nairesreinforcesthestrengthofthefindings.
TreatmentofPDBwithpotentbisphosphonates, particu-larly zoledronicacid,isveryefficient incontrolling disease activity and reduces bone pain in most patients2,5,16). By
reducingdiseaseactivity,treatmentisalsoexpectedto pre-vent long-term complications of PDB. Therefore, it would be expected that treatment with bisphosphonates results in improvedQoL inPDB and somestudies have evaluated this question,usually asasecondary end point. The Hori-zon study5,10 has shown that zoledronic acid was able to
improveQoLinPDBpatientsandthisresultwasmaintained fora long time.Interestingly,risedronate, inspiteofbeing effective inalarge proportionofpatients, didnotproduce similar effectsonQoL. Bythe otherside, inanotherstudy, the PRISM trial, treatment of PBD was not able to induce improvementsinQoL,4eveninthelongterm.Thismighthave
differences.WhiletheHorizonstudywasdouble-blindedand comparedasingleinfusionofzoledronicacidwith30mgof risedronatefor60days,the Prismstudy wasarandomized openstudy,whichcomparedtreatmentwithbisphosphonates withapain-driventreatment.Populationswerealsodifferent, withSF-36tendingtobehigherintheHorizonstudy.
Inthepresentstudy,asinthestudyofLangstonetal.,3bone
painwastheonlyparameterdirectlyrelatedtoPDBthat sig-nificantlypredictsSF-36results,butnoteveryPDBpatienthas painandpainisnottheonlyindicationfortreatmentofthis disease.Moreover,othersourcesofpain,suchassecondary osteoarthritis,arenotaffectedbytreatmentofPDB.Besides controlofsymptoms, treatmentofPDB isalsoindicatedto preventlong-termcomplications,16,17 so,averylong
follow-upperiodshouldbeemployedtodetectlong-termeffectson QoLduetothepreventionofcomplications.Currently, PRISM-EZisthestudywiththelongestfollow-upofQoLinPDB,three years,whatmaybenotenough.18
OnemajorlimitationofstudiesofQoLinPDB,includingthe presentone,istheircross-sectionaldesign.Longitudinal stud-ieswouldbemoreappropriateforchronicdiseasesasPDB,but itschronicandfrequentlyindolentnaturemakesthiskindof studiesmoredifficult.
AnotherfactorthatcouldimpairtheutilityofQoL ques-tionnaires in the evaluation of PDB treatment is the high prevalenceofcomorbiditiesinelderpeople,thepopulation mostaffectedbyPDB.Wetriedtoavoidthisproblemby exclud-ingsubjectswithotherchronicdiseases.Thisstrategyallowed ustoreduceconfoundingfactorsbutalsointroduceda draw-back,sinceoursamplecouldbehealthierthanthetypicalPDB patients.
Themainlimitationofthepresentstudyistherelatively smallsample,whichresultsinalownumberofsubjectswith somePDBcomplicationsthatcouldimpairQoLbutthatare nothighly prevalent,like hearingimpairment. Besides, we werenotabletocompareourresultstothoseofnormal Brazil-ianpopulationbecausetherearenotreferencevaluesofthese testsforourpopulation.Bytheotherhand,wewereableto excludesubjectswithconcomitantdiseasesthatalsoaffect QoL,thereforeeliminatingaconfusionfactor,whichwasnot donebyotherstudiesthathaveevaluatedQoLinPDB.
Conclusion
Inconclusion,amongthefactorsassociatedwithQoLinPDB, bonepainistheonlyonethatisassociatedwithdisease activ-ity,therefore,susceptibletotreatment.Theremainingfactors, includingdeformitiesandmaritalstatus,cannotbechanged bymedications.
It should be emphasized that PDB is a very heteroge-neousdisease,andsoaretheindicationsfortreatment.While treatment is recommended for all symptomatic patients, asymptomaticpatientsmayalsobetreated,accordingto fac-torsastheriskoffuturecomplications.Ifanytreatmentcan amelioratesymptomslikepain,someimprovementinQoLis expectedtobeidentifiableintheshortterm.However,ifthe indicationfortreatmentisthepreventionoffuture compli-cationsinanasymptomaticpatient,theeffectsinQoLcould onlybemeasured inlong-termstudies.Hence,thepresent
studysuggeststhat,becauseoftheheterogeneityof manifes-tationsofthisdiseaseandthelongperiodnecessaryforsome complicationstodevelop,QoLquestionnairesmightnotbean appropriateendpointforshort-termstudiesofPDBtreatment. FuturestudiesevaluatingeffectsoftreatmentonQoLinPDB patientsshouldeitherhavealongerduration orassessQoL morefrequently;morespecificquestionnairesofQoLcould alsobeemployed.
Funding
TheprojectdescribedwassupportedbyConselhoNacionalde Pesquisa(CNPq).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.RalstonSH.PathogenesisofPaget’sdiseaseofbone.Bone. 2008;43:819–25.
2.WernerdeCastroGR,HeidenGI,ZimmermannAF,MoratoEF, NevesFS,ToscanoMA,etal.Paget’sdiseaseofbone:analysis of134casesfromanislandinSouthernBrazil:another clusterofPaget’sdiseaseofboneinSouthAmerica. RheumatolInt.2012;32:627–31.
3.LangstonAL,CampbellMK,FraserWD,MaclennanG,SelbyP, RalstonSH.ClinicaldeterminantsofqualityoflifeinPaget’s diseaseofbone.CalcifTissueInt.2007;80:1–9.
4.LangstonAL,CampbellMK,FraserWD,MacLennanGS,Selby PL,RalstonSH.Randomizedtrialofintensivebisphosphonate treatmentversussymptomaticmanagementinPaget’s diseaseofbone.JBoneMinerRes.2010;25:20–31.
5.ReidIR,LylesK,SuG,BrownJP,WalshJP,DelPino-MontesJ, etal.Asingleinfusionofzoledronicacidproducessustained remissionsinPagetdisease:datato6.5years.JBoneMiner Res.2011;26:2261–70.
6.SetonM,MosesAM,BodeRK,SchwartzC.Paget’sdiseaseof bone:theskeletaldistribution,complicationsandqualityof lifeasperceivedbypatients.Bone.2011;48:281–5.
7.ViscontiMR,LangstonAL,AlonsoN,GoodmanK,SelbyPL, FraserWD,etal.MutationsofSQSTM1areassociatedwith severityandclinicaloutcomeinPagetdiseaseofbone.JBone MinerRes.2010;25:2368–73.
8.SarauxA,Brun-StrangC,MimaudV,VigneronA-M,LafumaA. Epidemiology,impact,management,andcostofPaget’s diseaseofboneinFrance.JointBoneSpine.2007;74:90–5. 9.GoldDT,BoistureJ,ShippKM,PieperCF,LylesKW.Paget’s
diseaseofboneandqualityoflife.JBoneMinerRes. 1996;11:1897–904.
10.ReidIR,MillerP,LylesK,FraserW,BrownJP,SaidiY,etal. Comparisonofasingleinfusionofzoledronicacidwith risedronateforPaget’sdisease.NEnglJMed.
2005;353:898–908.
11.MeunierPJ,SalsonC,MathieuL,ChapuyMC,DelmasP, AlexandreC,etal.Skeletaldistributionandbiochemical parametersofPaget’sdisease.ClinOrthopRelatRes. 1987;217:37–44.
12.CiconelliRM,FerrazMB,SantosW,MeinãoI,QuaresmaMR. Traduc¸ãoparaalínguaportuguesaevalidac¸ãodo
13.FleckMP,LouzadaS,XavierM,ChachamovichE,VieiraG, SantosL,etal.Aplicac¸ãodaversãoemportuguêsdo instrumentoabreviadodeavaliac¸ãodaqualidadedevida WHOQOL-bref.RevSaúdePública.2000;34:178–83. 14.Kalantar-ZadehK1,KoppleJD,BlockG,HumphreysMH.
AssociationamongSF36qualityoflifemeasuresand nutrition,hospitalization,andmortalityinhemodialysis.J AmSocNephrol.2001;12:2797–806.
15.WMADeclarationofHelsinki–EthicalPrinciplesforMedical ResearchInvolvingHumanSubjects[Internet].Availablein: http://www.wma.net/en/30publications/10policies/b3/index. html[accessed06.09.12].
16.RalstonSH,LangstonAL,ReidIR.Pathogenesisand managementofPaget’sdiseaseofbone.Lancet. 2008;372:155–63.
17.SelbyP,DavieMW,RalstonS,StoneM.Guidelinesonthe managementofPaget’sdiseaseofbone.Bone.2002;31: 366–73.