www.jped.com.br
ORIGINAL
ARTICLE
Comparison
of
the
finger-feeding
versus
cup
feeding
methods
in
the
transition
from
gastric
to
oral
feeding
in
preterm
infants
夽
,
夽夽
Cláudia
M.D.
Moreira
a,
Regina
P.G.V.
Cavalcante-Silva
b,
Cristina
I.
Fujinaga
c,
Francine
Marson
a,∗aUniversidadeFederaldoParaná(UFPR),Curitiba,PR,Brazil
bUniversidadeFederaldoParaná(UFPR),DepartamentodePediatria,Curitiba,PR,Brazil
cUniversidadeEstadualdoCentro-OestedoParaná(UNICENTRO),DepartamentodeFonoaudiologia,Irati,PR,Brazil
Received14September2016;accepted14December2016 Availableonline14July2017
KEYWORDS Preterm;
Suckingbehavior; Feedingmethods
Abstract
Objectives: Toassessthefinger-feedingtechniquewhencomparedwiththecupfeedingmethod
duringtheearlystageofpreterminfantfeedingtransitionregardingmilkloss,milkingestion
period,andcomplications.
Methods: Experimental,randomized,prospectivestudyincluding53preterminfantswith
ges-tation age<37 weeks,clinicallystable, andwith ascore of>28 pointsintheOral Feeding
ReadinessAssessmentScale.Thepretermbabieswererandomizedtobeincludedinthe
con-trolgroup,whichunderwentthefeedingtransitionusingacuporintheexperimentalgroup,
whichusedthefinger-feedingtechnique.TheanalysisofdatawasperformedusingStudent’s
t-testtoevaluatedifferencesbetweenmeanvaluesoftheappointedvariables,andFischer’s
testfor categoricalvariables;theasymmetricvariableswereassessedby theKruskal---Wallis
ANOVAtest.
Results: Whencomparedwiththecontrolgroup,theexperimentalgroupshowedlowermilk
loss,longermilkingestiontime,andalowerfrequencyofcomplicationsduringfeeding.The
significancelevelwassetat5%,withaconfidenceintervalof90%.
Conclusion: Thefinger-feedingtechniquewasshowntobeabetterfeedingtransitionmethod
regardingefficacywhencomparedwithcupfeedingmethod,duetolowermilklossandfewer
complicationepisodes.
©2017SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen
accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/
4.0/).
夽
Pleasecitethisarticleas:MoreiraCM,Cavalcante-SilvaRP,FujinagaCI,MarsonF.Comparisonofthefinger-feedingversuscupfeeding methodsinthetransitionfromgastrictooralfeedinginpreterminfants.JPediatr(RioJ).2017;93:585---91.
夽夽
StudyconductedatUniversidadeFederaldoParaná(UFPR),Curitiba,PR,Brazil.
∗Correspondingauthor.
E-mail:[email protected](F.Marson). http://dx.doi.org/10.1016/j.jped.2016.12.008
PALAVRAS-CHAVE Prematuro;
Aleitamento materno; Métodosde alimentac¸ão
Comparac¸ãoentreométodosonda-dedoversuscoponatransic¸ãoalimentar
dorecém-nascidoprematuro
Resumo
Objetivo: Avaliaratécnicasonda-dedoemcomparac¸ãoaocoponoiníciodatransic¸ãoalimentar
doprematuroquantoàperdadeleiteofertado,tempodeingestãoecomplicac¸ões.
Métodos: Estudo experimental, randomizado,não cego, prospectivocom 53prematuros de
idadegestacional<37semanas,clinicamenteestáveisecomescore>28pontosnaAvaliac¸ãoda
Prontidãoparainíciodaalimentac¸ãoporviaoral.Osprematurosforamrandomizadosparao
GrupoControlequerealizouatransic¸ãoalimentarcomocopoeparaoGrupoExperimentalque
utilizouatécnicasonda-dedo.Naanálisedosdados,foramaplicadosotestetdeStudentpara
avaliaradiferenc¸ademédiaseotesteexatodeFisherparaasvariáveiscategóricas,enquanto
paraasvariáveisassimétricasfoiaplicadoaAnovadeKruskal-Wallis.
Resultados: Ogrupo experimentalapresentou em relac¸ãoao grupo controle, diferenc¸a
sig-nificativa quanto a menor perda de leite, maior tempo de dieta e menor frequência de
complicac¸ões.Oníveldesignificânciafoide5%epoderdetestemínimode90%.
Conclusão: Atécnica sonda-dedomostrou-se ummétodo alternativodetransic¸ãoalimentar
superioremsuaeficiênciaquantoamenorperdadeleiteemenorincidênciadecomplicac¸ões.
©2017SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo
OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.
0/).
Introduction
Preterm newborn face a difficult reality, which is that of adaptingtoextrauterinelife.1---3
Breastmilkis thebest foodfor preterm newborns,and itisalwaysindicated,asitcontainsspecificnutrientsthat willcontributetotheirmaturation,representingan impor-tantfactorintheprotectionagainstinfections,leadingto abetterdigestibilityandabsorptionofthesenutrientsand promotingbetterbraindevelopment.4,5
However,in a neonatalintensive care unit (NICU),the preterm population cannot always be fed directly at the mother’s breast, either due to clinical instability or the mother’sabsence.6,7
Furthermore, it is worth noting that preterm new-bornshave inadequateoral functions due toneurological immaturity,abnormalmuscletone,lackofmuscleactivity integration,andalterationsinoralreflexcoordination, lead-ingtolessactive,irregular,anddiminishedstrengthreflexes anddifficultymaintainingalertness.Allthesefactorslead tothe initial need tofeed the preterm newborn through analternativefeedingroute,asisthecaseofgastrictube feeding.8---10
The way the milk is offered to preterm infants is an important variable to consider. The advantages and disadvantages of the methods are discussed in terms of physiological stability and impact on exclusive breastfeeding.11---13
Several forms of feeding are used, such as cup, suc-tionfroma syringewiththegloved finger, translactation, finger-feeding,paladai,andbottle,amongothers;scientific justificationisnecessaryforallmethods,butforthecupand thebottle,whichhavebeenwidelystudied.12---16
The useof techniques tomaturethe sensorimotor-oral systemhasbeenexplored,sothatthepretermnewborncan undergoasaferandshortertransitiontooralfeeding.17
Thefinger-feedingmethodisatechniqueinwhichmilk issupplied bysuctiontopreterminfantsthrougha gastric tubeconnectedtoasyringeandattachedtotheglovedsmall fingerwithadhesivetape.Althoughitisawidelyused tech-nique in several neonatalservices, studies describing the technique, its indications. use, benefits, advantages, and disadvantagesarestillscarce.14,18---20
Therefore,itis necessarytoenhancetechnologiesthat aimtoimprovethesuctionpatternand,consequently,the preterminfant’scapacityoforalfeeding,primarilydirected to breastfeeding.The cup-feeding method has been indi-catedby theWorld HealthOrganization asthemethod of transitionand/ororalfeedingcomplementationforpreterm infants, as it does not cause the nipple confusion phe-nomenonanddoesnotinfluencethepreterminfant’ssuction function.20,21
It should be noted that, in clinical practice and in the NICU routine,mothers are notalways present, which is the reality of many health services. Due to maternal absence,thepreterminfantisfedforlongperiodsusingthe cup, withoutperformingthesuctionfunction. Asaresult, thisconditiondiscouragesmaternalbreastfeeding,because feedingpreterminfantexclusivelythroughthecupinducesa modificationinhis/heroralbehavior.22Thischangein
suck-ingbehaviorisevidentmainlyinthedifficultyinopeningthe mouth and theanteroposterior movement of the preterm infant’s tongue. When the mother comes to the NICU to breastfeed thechild, a change inthe sucking behaviorat themother’sbreastisobserved,delayingandimpairingthe breastfeedingprocess.
suctionactionsperformedinthemother’swomb.Therefore, theaimofthepresentstudywastoevaluatethe effective-nessof thefinger-feeding techniquein preterm infantsin comparisonwiththecup-feeding methodatthe beginning ofthefeedingtransitionfromthegastrictotheoralroute, regardingtheloss ofmilkoffered, timeofmilkingestion, andpresenceofcomplications.
Methods
This was an experimental, randomized, controlled, non-blinded,prospective,andlongitudinalstudy.
The study population was selected among the 168 preterminfantsadmittedtotheNICUofHospitalde Clíni-casinthecityCuritiba,stateofParaná,Brazil,fromJune 2012toMarch2013.Ofthe93neonatesthatcomprisedthe target population, 53 wereeligiblefor study,selectedby probabilisticsamplingtechnique,withblockrandomization. The sample was calculated considering the main out-comes of the study measured as proportions, considering effectsizeof30%, typeIerrorof 5%,andtypeII errorof 10%,with25---30casesbeingestimatedpergroup.
Forrandomization,theauthorsasequenceofblock let-ters of equal size, placed into brown envelopes, which were drawn by the nurses responsible for the NICU, and theassessedinterventionsweredistributed,blockbyblock, untiltheprocessofallocationofthestudyparticipantswas completedforthecontrolgroup(CG),identifiedbythe let-terA,andfortheexperimentalgroup(EG),identifiedbythe letterB.Theresearchersdidnotparticipateinthisprocess. Therewasasubdivisionregardingthegestationalageranges inbothgroups,aimingtomaintainsamplehomogeneity.
The following were considered as inclusion criteria: gestational age <36 weeks and six days, determined by obstetricultrasoundperformedupto12weeksgestationor bychronology,determinedbytheNewBallardMethod;not receivingoralmilkuntilinclusioninthestudy;ascore>28 pointsinthereadinessfororal feedingassessment,which consists in a speech therapy-audiological assessment consisting of items with a variationin performance, with scores rangingfrom0 to2,totalinga sumranging from0 to3623; and the signing of theinformed consentformby
parents/tutors. The exclusion criteria included: grades 3 and4periventricularhemorrhage;clinicalinstabilityatthe timeorduringthestudy,suchasthepresenceof necrotiz-ingenterocolitis, sepsis,bronchopulmonarydysplasia, and otherrespiratoryorhemodynamicclinicalinstability;Apgar score<5 at the 5thminute; and presence of genetic syn-dromes,neurologicaldisorders,orcongenitalmalformation oftheheadandneckorofcentralnervoussystem.
Trainingforthefinger-feedingtechniquewasperformed bythemainstudyresearcherandlaterofferedtotheNICU healthteamofHospitaldeClínicasregardingthehandling oftheutensilsusedinthetwostudytechniques,i.e.,the cupandfinger-feeding,andeducationalmaterialwasmade available.
Theincubatororcribwasidentifiedwithanimagerelated tothefeedingtransitionmethodperformedbythenursing team,tominimizethe interruptionofthe studyprotocol. The evaluationsat thebeginning ofthefeeding transition werefilmedandthevariablesassessedwere:
- Lossoftheofferedmilk:usingagauzepadunitpositioned below the chin of the neonateand weighed in a preci-siondigitalscalewithasensitivityof0.1g,themilkwas offeredbythecaregiverondutyandthefeedingandgauze weighingweresupervisedbythenursingteambeforeand aftertheneonatewasfed.
- Timeoffeeding:thetimeofthefeedingofferedbythe nursingteamwasobservedduringthefilming.
- Presenceofcomplicationsduringtheoralfeeding:these complicationswereoxygensaturation,cyanosis, respira-toryeffort,andgagging.Theobservationofthesesignsof stresswasperformedbythenursingteam.
The videos collected from both groups were analyzed byexperiencedprofessionals,whohadbeenworkinginthe NICUforoverfiveyears.
Useofthefinger-feedingtechnique
Thefinger-feedingtechniquewasusedinamannersimilarto thatdescribedbyFujinagaetal.forthefeedingtransition; first,thetipofthecatheterwascutandfixatedwith adhe-sivetapetotheinner sideofthegloved smallfinger.The otherendofthecatheterwasconnectedtoasyringe with-outthe plunger,attachedlaterallytotheindividualapron wornbythecaregiverat thelevel oftheneonate’s head, withrawmilkmilkedfromthemotherorfromthehuman milkbank.20 The milkwouldslidethroughthetube asthe
suckingpattern was adjusted by the newborn andnot by gravity,atwhichpointthepulpofthesmallfingerwasfacing thehardpalate.
Useofthecup-feedingtechnique
The cup-feeding technique was carried out by the nurs-ingteam according tothe service routine.The technique consistedinofferingthemilkinadisposable,50-milliliter plastic cup. The neonate was kept in a seated or semi-seated position, with head and body aligned. The milk wasplaced ontheedgeof thecup, which waspositioned on the neonate’s lower lip, with the edges touching the labialcommissures, where theneonate performed tongue anteriorization movements, sucking the milk from the cup.13,15,21
Thisstudy wasapprovedbytheCommitteeofEthicsin Researchin Human Beings of Hospital dasClínicas, under CAAENo.01934912.6.0000.0096.
The data were entered in a spreadsheet and the dif-ference between the continuous variables was evaluated usingStudent’s t-test, Mann---Whitneytest,andANOVA for repeatedmeasures,withaminimumsignificancelevelof5%, usingStatistic-StatsoftTM(StatSoft,Inc.,ElectronicStatistics Textbook,USA).
Results
Table1 Characteristicsofthecontrolandexperimentalgroups(n=53).
Characteristics Controlgroup(n=27) Experimentalgroup(n=26) p
GenderM/F 20/07 17/09 0.55a
Correctedgestationalage(weeks) 32.3+2.6 33.0+2.4 0.31b
Birthweight(g) 1812.6+529.9 1985.6+59.9 0.27b
Apgar1stminute<7 04(14.8%) 06(23.1%) 0.41a
Cesarean/vaginaldelivery 18/09 18/08 1.00a
Maternalage(years) 26.6+7.6 29.2+7.7 0.22b
Primiparous 11(40.7%) 07(26.9%) 0.31a
Gestationcomplications
PTL 15(55.5%) 12(46.1%) 0.51a
HDP 07(25.9%) 09(34.6%) 0.47a
GDM 03(11.1%) 04(15.4%) 0.66a
PA 02(7.4%) 01(3.8%) 0.63a
PTL,pretermlabor;HDP,hypertensivediseaseofpregnancy;GDM,gestationaldiabetesmellitus;PA,prematureamniorrhexis. aFisher’sexacttest.
b Student’st-test.
finger-feedingtechnique,comprisedatotalof26newborns, 12with32---34weeksofGA(22.6%)and14with34---36weeks ofGA(26.4%).
Thecontrolandexperimentalgroupswerehomogeneous regardingbirthweight,gestationalage,andgender.There werealso nodifferences regardingmaternal age, typeof delivery,frequencyofmaternalobstetriccomplications,and Apgarscoreatthe1stminute(Table1).
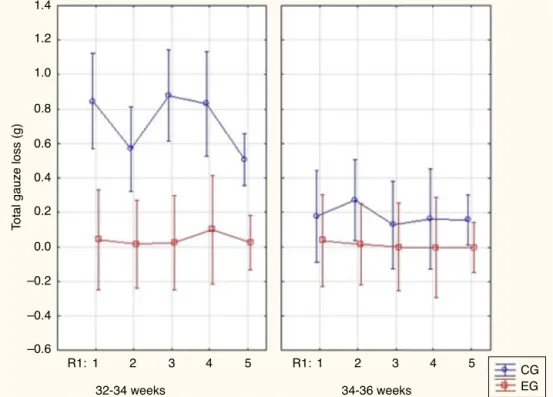
ThecontrolgroupinbothGArangesshowedsignificantly higher values for milk loss, as measured by total gauze weighting,thantheexperimentalgroup.Thismilklosswas higherinthecontrolgroupamonginfantswith32---34weeks ofGA(Fig.1).
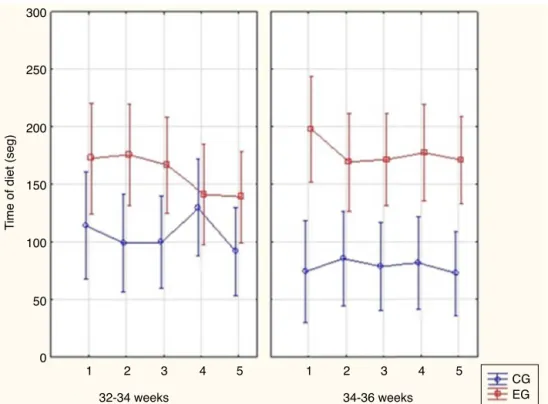
Thetimeoffeedingintheexperimentalgroupwaslonger thanthetimeoffeedinginthecontrolgroup(Fig.2).
Complicationsoccurredsignificantly more oftenamong neonates with 32---34 weeks of GA in the control group (Fig.3).However,nosignificantdifferenceswereobserved regarding complications in the control and experimental groupsintheGArangeof34+1/36+6weeks.
Regardingweightgain,asimilaritywasobservedbetween theassessedgroups.Inthecontrolgroup,themedianweight differencebetweenthe1standthelastweightassessment was 145.0g, ranging from −50g to 850.0g, while in the experimental group, themedian was85.0g,ranging from −140gto1060g(p=0.34).
1.4
1.2
1.0
0.8
0.6
0.4
0.2
0.0
–0.2
–0.4
–0.6
R1:1 2 3 R1:1 2 3
32-34 weeks
T
o
tal gauze loss (g)
34-36 weeks
4 5 4 5 CG
EG
Figure1 Totallossmeasuredbygauzeweighinginthecontrolgroup(CG)andintheexperimentalgroup(EG)with32---34weeks
300
250
200
150
100
50
0 1
32-34 weeks
T
ime of diet (seg)
34-36 weeks
CG EG 1
2 3 4 5 2 3 4 5
Figure2 Timeofdietinthecontrolgroup(CG)andintheexperimentalgroup(EG)with32---34weeksgestationalage(GA)and
34---36weeksGA.Obs:FactorialANOVA:p=0.26.
100 90 80 70 60 50 40 30 20 10 0
CG 32-34
%
No Yes
34-36 CG
EG EG
Figure3 Complicationsinthecontrolgroup(CG)andinthe
experimentalgroup(EG)with32---34weeksofgestationalage
(GA) and34+1to 36+6weeks GA.Obs: Fisher’s exact test:
p=0.001.
Discussion
The feeding transition from the gastric tothe oral route is agreat challenge,notonly for thepreterm infant,but alsoforthehealthcareteam,asitistheirresponsibilityto assessthebestfeedingtransitionmethodforeachnewborn, consideringitisaperiodthatrequiresattentionregarding safetyandefficiencyindietadministration.
Thefinger-feedingtechniquehasemergedasatransition alternative,widelyusedintheroutineofseveralservicesas aformofsuctiontrainingand/or complementaryfeeding, whenthemotherisabsentatthetimeoffeeding.Itisalso analternativetoartificialnipplesandbottlesinthehospital
environment,insituationswherecup-feedinghasnotbeen successfullyimplemented.13---15,21
Thecup,autensilusedinthefeedingtransitionperiod, haditsapplicabilityassessed in comparisontothe finger-feedingtechniqueregardingtheadministrationprocedures anditsuse,becauseitisthemethodrecommendedbythe WorldHealthOrganization (WHO)andusedin theNICUof HC-UFPR. It was not the objective of this study to chal-lengethe benefitsofcup-feeding inthetransition period, whichhasbeen widelystudied anddemonstrated,12,13,15,21
buttoevaluatetheapplicabilityofbothmethodsina popu-lationofpreterminfantswithdifferentrangesofcorrected GA.
The previous training aimed at teaching all study col-laborators in order to avoid the inappropriate use of the methods or that lack of experience could lead to complicationsorinterferewiththeresultsfound, consider-ingthelackofknowledgeorinadequateuseofalternative techniquesinoral feedinginpreterminfantscanresultin risksituations.17,23,24
Duringthedatacollectionperiod,therewerenochanges inthenursingteamorinthemeasurementequipment.
Thisstudywascarriedoutduringthefeedingtransition periodofpreterminfants,anddatawereassessedfromthe first to the fifth days, because it is a critical period for theimplementationoftheoraldiet,asitrequiresgreater attentionregardingtheeffectivenessofthepreterminfant’s undergoingfeeding transition. Thus, the need for further studiesassessingtheapplicabilityofthefinger-feeding tech-niqueinothervariablesandinthefollow-upofthefeeding transitiontotheoralrouteisreinforced.
results.IninfantswithyoungerGA,suckingmaybe ineffi-cient,resultingingreaterenergyexpenditureandgreater risksduetothelackofswallowing-breathingcoordination, whichmayleadtogreaterchancesofcomplications. More-over,itshouldbenotedthat,withoutthissubdivision,the samplewouldnotbehomogeneousregardingcoordination maturityofthesuction-swallowing-breathingfunctions, as preterminfantswithGAhigherthan34weeksarealready abletofeedmoresafelyandefficiently.2,14,16,23
InbothGAranges,thecontrolgroupshowedsignificantly highervaluesofmilklosswhencomparedwiththe experi-mentalgroup,withahigherlossinthecorrectedGArange of32---34 weeks.Thissuperiority regardingfeeding accep-tance,withlower milkloss observed in the experimental group,isinagreementwithstudiesthatdescribedagreater lossofmilkwiththeuseofthecup-feedingmethod.13,17,21
Otherstudiesobservedthatthefinger-feedingtechnique alsoincreasedtheamountofmilkingestedbythenewborn andamoreefficientuseoftheoraldietwhencomparedto thecup.13,17
Thelossofmilkand,consequently,incompleteingestion ofthetotalprescribedvolumeisasituationwhich,in addi-tionto leading to weightloss, may influence the clinical statusofpretermnewborns.
The finger-feeding technique was shown to require more time and have a higher cost, both in the orga-nization of the material used and in the milk supply when compared with the cup-feeding. Nonetheless, it provides the newborn with oral stimuli that will favor suction training,alertness maintenance, andcoordination of suction/deglutition/breathing. The longer duration of the diet by the finger-feeding technique was due to the fact that milk was offered to the newborn only when he/she sucked the gloved finger, without the possibility of gravity flowing. Therefore, it is believed that feeding occurred more physiologically, respecting the time of the preterm newborn regarding the coordination of the suction-swallowing-breathingfunctions, aswellasresting. Thus,itis believedthat thebenefitsprovidedwhen using the finger-feeding technique for the premature newborn inthefeedingtransition,especiallyinthegestationalage rangebelow34weeks,compensatethelongertimeittakes tousethemethod.16,20,22
Regardingthecomplications,it wasobservedthat they werestatisticallyhigherin thegroupthatusedthe cupin therangeof32---34weeksofGA.Inthegroupof34+1/36+6 weeksofGA,therewasnosignificantdifferencebetween thegroupsregardingthepresenceofcomplicationsduring theuseofeachtechnique.Thisdifferenceisjustifiedbythe factthat preterminfants in the34+1/36+6weeks ofGA havehigherneurologicalmaturity,achievingabetter main-tenanceofalertnessandsucking,swallowing,andbreathing coordinationduringtheoraldiet.
Oneofthelimitationsofthisstudyisthelackofcontrol regardingevacuationfrequency or occurrence of diarrhea aspossiblecomplicationsofthetechniquesused.
Additionally, no significant difference was observed in relation to the groups regarding exclusive breastfeeding ratesathospitaldischarge.Theauthorsbelievethereisno difference, because both groups received encouragement andsupporttobreastfeed,suchasearlystimulationof milk-ing,guidelines,andencouragementtopracticethekangaroo
methodandmaternalbreastfeeding,asitisaroutineinthe NICUofHC-UFPR.
Moreover,it shouldbenotedthattheaimof thisstudy wastodemonstratethe safetyofthefinger-feeding tech-niqueasamethodoftransitionfromthegastrictotheoral route, and not asa feeding method. This is because the aimis toalwaysprovideassistancethat canprioritizethe mother’spresence intheNICU,aligningthe techniquesto encouragebreastfeedingwithmaternaldesires.
Furtherstudiesstillneedtobeperformedtoassessthe effects of thefinger-feeding technique ontheprevalence of post-discharge breastfeeding, assessing its long-term impacts.
Finally,it is noteworthy thatalthough the literature is scarceregardingthedescription,indication,anduseofthe finger-feedingtechnique,itisbelievedthelatterisatype offeedingtransitionthatbenefitsthepreterminfant, espe-ciallyinthecorrectedGArangeof32---34weeks,asitallows suctiontrainingandtheprovisionofsafeandeffectiveoral milksupplywhenbreastfeedingisnotpossible.13---17
The results shown here reinforce the benefits of this technique and provide scientific evidence on the evalu-ation of feeding technology in preterm neonates, which shouldcertainly have an impactonthe developmentof a healthier population and,thus, contribute to amore sta-blesocietyfromthephysical,physiological,andemotional standpoints.
The finger-feeding technique wasshown to bea supe-rioralternativemethodatthestartofthedietarytransition regardingitsefficiency,whencomparedwiththecup feed-ing method, due tothe lower milk loss and incidence of complications,mainly intherangeof32---34 weeksofGA. However,thedurationof thedietsupply usingthe finger-feedingmethodwassignificantlylongerthanthatofthecup feedingmethod.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.LamounierJA.Aleitamentomaternoem prematuros:política públicanaatenc¸ãoprimária.RevPaulPediatr.2016;34:137---8.
2.KennerC,DiazPF, ValdebenitoMR.Thetransitionfromtube tonippleintheprematurenewborn.NewbornInfantNursRev. 2007;7:114---9.
3.PereiraLB,AbrãoAC,daSilvaOC,RibeiroCA.Vivências mater-nasfrenteàspeculiaridadesdaprematuridadequedificultama amamentac¸ão.Textocontexto---enferm.2015;24:55---63.
4.Gallegos-MartínezJ,Reyes-HernándezJ,ScochiCG.Oneonato prematurohospitalizado:significadodaparticipac¸ãonaunidade neonatalparaospais.RevLatAmEnferm.2013;21:1360---6.
5.SchanlerRJ.Outcomesofhumanmilk-fedprematureinfants. SeminPerinatol.2011;35:29---33.
6.Brasil. Ministério da Saúde. Secretaria de Atenc¸ãoa Saúde. Departamentode Ac¸õesProgramáticas Estratégicas.Atenc¸ão humanizadaaorecém-nascidodebaixopeso:MétodoCanguru. 2nded.Brasília:MinistériodaSaúde;2011.
8.LimaAH,CôrtesMG,BouzadaMC,FricheAA.Pretermnewborn readiness for oral feeding: systematic review and meta-analysis.CoDAS.2015;27:101---7.
9.CastelliCT,AlmeidaST.Evaluationoforofacialcharacteristics and breastfeeding in preterm newborns before hospital dis-charge.RevCEFAC.2015;17:1900---8.
10.HaroonS,DasJK,SalamRA,ImdadA,BhuttaZA.Breastfeeding promotioninterventionsandbreastfeedingpractices:a system-aticreview.BMCPublicHealth.2013;13:S3---20.
11.Brandão DS, Venancio SI, Giugliani ER. Associac¸ão entre a implantac¸ãodaRedeAmamentaBrasileindicadoresde aleita-mentomaterno.JPediatr(RioJ).2015;91:143---51.
12.Nyqvist KH, Ewald U. Surface electromyography of facial musclesduringnaturalandartificialfeedingofinfants: identifi-cationofdifferencesbetweenbreast-,cup-andbottle-feeding. JPediatr(RioJ).2006;82:85---6.
13.Flint A, New K, Davies MW. Cup feeding versus other forms of supplemental enteral feeding for newborn infants unable to fully breastfeed. Cochrane Database Syst Rev. 2016;8:CD005092.
14.RahmanMA,SubramanianS,KandrajuH,MurkiS.Comparison ofsuckingpatterninprematureinfantswithdifferentfeeding methods.IndianPediatr.2015;52:961---3.
15.MarofiM,AbediniF,MohammadizadehM,TalakoubS.Effectof paladyandcupfeedingonprematureneonates’weightgainand reachingfulloralfeedingtimeinterval.IranJNursMidwifery Res.2016;21:202---6.
16.MoreiraCM,Cavalcante-SilvaRP,MiyakiM,FujinagaCI.Efeitos da estimulac¸ão da succ¸ão não nutritiva com dedo enluvado natransic¸ãoalimentaremrecém-nascidoprematurodemuito baixopeso.RevCEFAC.2014;16:1187---93.
17.Araújo VC,MacielAC,PaivaMdeA, BezerraAC.Volume der-ramado,saturac¸ãodeoxigênioefrequênciacardíacadurante a alimentac¸ão de recém-nascidos prematuros: comparac¸ão entre dois métodos alternativos de oferta. CoDAS. 2016;28: 212---20.
18.Lemes EF, Silva TH, Correr AM, Almeida EO, Luchesi KF. Estimulac¸ãosensoriomotoraintraeextra-oralemneonatos pre-maturos:revisãobibliográfica.RevCEFAC.2015;17:945---55.
19.Silva WF, Guedes ZC. Preterm and late preterm infants: their differences and breastfeeding. Rev CEFAC. 2015;17: 1232---40.
20.FujinagaCI,DucaAP,PetroniRA,RosaCH.Indicac¸õeseusoda técnica‘‘sonda-dedo’’.RevCEFAC.2011;4:721---4.
21.Pacheco ST, Rodrigues BM, Araújo BB, Cabral IE, Organista RR, Enrici MJ.Significadodo usodo copinhoem unidadede terapiaintensiva neonatal:a vivênciamaterna. Revenferm. 2012;20:434---8.
22.NyqvistKH,EwaldU.Avaliac¸ãoeletromiográficadosmúsculos faciaisduranteoaleitamentonaturaleartificialdelactentes: identificac¸ãodediferenc¸asentrealeitamentomaternoe aleita-mento com uso de mamadeira ou copo. J Pediatr (Rio J). 2006;82:85---6.
23.FujinagaCI,deMoraesSA,Zamberlan-AmorimNE,CastralTC, de Almeida A, Scochi CG.Clinicalvalidation of thePreterm OralFeedingReadinessAssessmentScale.RevLatAmEnferm. 2013;21:140---5.