Bull Pan Am Health Organ 15(l), 1981.
DEEP MYCOSES
IN PATIENTS
WITH
ABNORMAL
CHEST
X RAY FINDINGS
Humberto
Campins, 2 N&tor
Rinch,J
Maria B. de Albornoz
,4
Ladislao
Pollak,s and Rafael Darricarreres
A group of 510 patients with abnormal chest X ray findings at Venezuela’s Vargas Hospital were examinedfor mycotic disease. The results showed that serologic tests for histoplasmosis and paracoccidioidomycosis made valuubL contributions to diagnosis of these ailments.
Introduction
Deep mycoses were first reported in
Venezuela early in this century, when the
Venezuelan medical literature began register-
ing the occurrence of mycetomas caused by
Actinomyces and Eumycetes (I-4). The earliest
literature on confirmed cases of sporotrichosis
appeared in the 1930s (5L 6, 7), when the
existence of paracoccidioidomycosis (8, 9, 10)
and chromomycosis (11, 12) was also demon-
strated.
Coccidioidomycosis was discovered in
1948. The first cases of this disease were
reported in 1949 (13, 14), and the extent and
infectious potential of the largest endemic area
in Venezuela was defined (15). This was the
third such area in the world to be recognized.
The presence of cryptococcosis (16) was
also confwmed in 1949 and the first evidence
of histoplasmosis (17) was obtained, the exis-
tence of this latter disease being fully con-
firmed some time later (18, 19).
Since these discoveries, many publications
IProject supported by the Pan American Health Orga- nization.
ZMedical Mycology Section, Institute of Pathological Anatomy, Vargas Hospital, Caracas, Venezuela.
3Pneumology Service, Vargas Hospital.
*Medical Mycology Section, National Dermatology Institute, Vargas Hospital.
SLaboratory Service, National Tuberculosis Institute, Caracas.
6Department of Microbiology, Institute of Pathologi- cal Anatomy, Vargas Hospital.
on these and other deep mycoses have ap-
peared in the Venezuelan medical literature
(20-24). These have enriched the published
record of reported cases, have described
diverse affected regions and clinical disease
forms, and have provided interesting informa-
tion about the epidemiology of the causative
agents and some of their ecological features.
Despite this wealth of scientific informa-
tion, however, Venezuelan physicians still
lack precise pathological data about the extent
and some of the peculiarities of these diseases.
Some of the various causes of this situation are now in the process of being overcome; and the
perfection and simplification of diagnostic
techniques, together with recent methods
derived from progress in immunology, have
paved the way for dispelling the unknown.
The purpose of the work reported here-a
study of 510 patients with abnormal chest X
ray findings- is to contribute to that end.
Materials and Methods
The aforementioned group of patients at
the Vargas Hospital in Caracas-whose chest
X rays indicated some abnormality-were
sent to the hospital’s Pneumology Service and
to the Mycology Section of the Institute of
Pathological Anatomy. Patient case histories,
if unavailable, were drawn up; blood was ob-
tained for serologic study; and intradermal
tests were conducted with coccidioidin, histo-
plasmin, and paracoccidioidin.
50 PAHO BULLETIN l vol. 15, no. 1, 1981
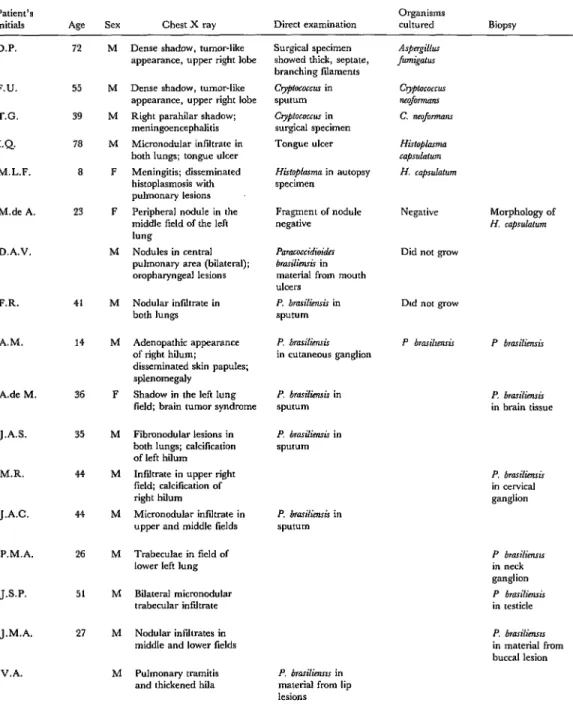
Table 1. Diagnostic findings for 17 patients
Patient’s
initials Age Sex Chest X ray Direct examination
Organisms
cultured Biopsy
D.P. 72
F.U. 55
T.G. 39
I.Q. 78
M.L.F. 8
M.de A. 23
D.A.V.
P.R. 41
A.M. 14
A.de M. 36
J.A.S.
M.R.
J.A.C.
P.M.A.
J&P.
J.M.A.
35
44
44
26
51
27
V.A.
M
M M M F
F
M
M
M
F
M
M
M
M
M
M
M
Dense shadow. tumor-like appearance, upper right lobe Dense shadow, tumor-like appearance, upper right lobe Right parahilar shadow; meningcencephalitis Micronodular infiltrate in both lungs; tongue ulcer Meningitis; disseminated histoplasmosis with pulmonary lesions Peripheral nodule in the middle field of the left lung
Nodules in central pulmonary area (bilateral); ompharyngeal lesions
Surgical specimen showed thick, septate, branching fiiaments
Crypfococcw in sputum
C~pfoc0ccu.r in surgical specimen Tongue ulcer
His~oplmm in autopsy specimen
Fragment of nodule negative
Paracoccidioides bro.rilimrir in material from mouth ulcers
Nodular inltrate in P. brariIimsi.r in
both lungs sputum
Adenopathic appearance of right hilum; disseminated skin pap&s; splenomegaly
Shadow in the left lung field; brain tumor syndrome
P. b7asilim.G
in cutaneous ganglion
P. bra.&mir in P. bm&n.ris
sputum in brain tissue
Fibmncdular lesions in both lungs; calcification of left hiIum Infiltrate in upper right field; calcilication of right hilt””
Micronodular inliltrate in upper and middle fields
P. brarilimis in
P. brariliensir in sputum Trabeculae in field of
lower left lung Bilateral micronodular trabecular inlidtrate Nodular infiltrates in middle and lower lields Pulmonary tramitis and thickened hila
P. bra.rilienm in material fmm lip lesions
Negative
Did not grow
Morphology of
H. caprulahm
Dtd not grow
P. bmasiliemir
in cervical ganglion
P bra.riiimms
in neck ganglion
P bmilimis
in testicle
P. bmilimrr
in material from buccal lesion
’ Blank spaces indicate the tests in question were not perfomwd. The meaning of the various letters m the table are as follows: H 3 Immuncdiffusion test for histoplasmosis.
P - lmmuncdiffusion test for paracoccidioidomycosis. Hc = Hisloplama capsuhlum antigen.
Camjhs et al. l MYCOSES IN PATIENTS WITH ABNORMAL, X RAYS 51
with confirmed mycotic disease.
lmmunodiIlL3ion
Ser010gy Intradennal inoculation with:
Complement fixation Paracoccidmidin
Yeast- Fiiame”tous- Restrepo antigen at: Fava Netto antigen at:
phase phase Histo- Coccidio-
antigen antigen plasmin idin 24 hours 48 hours 24 hours 48 hours
H (M and H bands) P negative H (M band) P negative H negative P negative H negative P positive
H negative P positive H negative P positive
H negative P positive H negative P positive H negative P positive H negative P positive H negative P positive H negative P positive H negative P positive H negative P positive
Hc 1:16 i:64 Pb neg. 1:8 Hc I:64 I:256 Pb i:32 1:32
C I:16
Hc neg. Pb neg. C Hc neg. Pb I:64 C
neg. neg. neg. neg. I:64 neg. Hc neg. Pb 1:32 C Hc neg. Pb neg. C Hc neg. Pb I:128 C Hc neg. Pb 1:32 C Hc neg. Pb 1:16 C Hc I:16 Pb 1:16 C Hc 1:16 Pb I:256 C UC neg. Pb 1:128 C Hc 1:8 Pb I:128 C Hc 1:16 Pb I:16 C
neg. neg. doubtful doubtful
13mm 0 16mm 15mm 17mm 14mm
neg. 0
1:32 neg.
neg. 0
I:16 neg.
neg. 0
I:128 neg.
neg. 0
I:32 neg.
neg. 15mm
1:16 neg.
neg. 5mm
1:8 neg.
neg. 0
1:64 neg.
neg. 15mm
1:128 neg.
I:128 0
neg.
neg. 0
I:16 neg.
0
0
0
0
0
0
0
0
0
0
14mm 1Omm 12mm 1Omm
0 0 0
0 0 0
0 0 0
15mm 18mm 20mm 19mm
0 0 8mm 7mm
26mm 26mm 21mm 21mm
1Omm 1Omm IOmm IOmm
52 PAHO BULLETIN * vol. 15, no. 1, 1981
The first two antigens (coccidioidin7 and
histoplasmin8) were administered to all pa-
tients except those with erythema nodosum or
erythema multiforme at a dilution of 1: 10;
the resulting skin reactions were observed at
24 and 48 hours. Two paracoccididioidin an-
tigens were used for these intradermal tests.
One was prepared by the Mycology Section of
the National Dermatology Institute in
Caracas using the Fava Netto Technique
(25). The other, prepared according to the
technique of Angela Restrepo (26) at her
laboratory in Medellin, Colombia, was
generously contributed by her. Both antigens
were administered at a dilution of 1: 10, and
the results were observed at 24 and 48 hours.
(The originators of the methods for preparing
these antigens consider 24 hours to be the op- timal lag time.)
The patients’ sera were used to perform
complement fixation (CF) tests with coccidio-
idin and with antigens of the yeast and fila-
mentous phases of Histoplasma capsulatumg and
Paracoccidioides brasiliensis. In addition, the sera
were employed in plaque precipitation (im-
munodiffusion) tests for histoplasmosis and
paracoccidioidomycosis. These serologic tests
were performed at the Microbiology Section
of the Jo& Ignacio Bald6 National Tuberculo-
sis Institute. The P. brasiliensis antigens for
these serologic tests were prepared by one of
the authors (L.P.), and the H. capsulatum and
Coccidioides immitis antigens were supplied by the U.S. Center for Disease Control in Atlan- ta, Georgia. The research project participants
met periodically for analysis and discussion of
the cases under investigation.
‘Supplied by the Department of Medical Mycobacte- rioloav, School of Medicine. Universitv “I of California. U.S.A. (Prof. D. Pappagianis). ’
@Supplied by the Mycobacteriology Branch, Bacteriol-
ogy Division, Bureau of Laboratories, Center for Disease
Cldntrol, Atlanta, Georgia, U.S.A. (Dr. Hugo David).
9Two varieties of Histoplasma caps&turn are recognized today: var. capstdatum and var. d;boisii. In addition, sex- ual reproduction was demonstrated in 1972 by Kwon- Chung, who referred to the sexual phase as Emmonsklla capsulata (27). All references to the fungus in this article are to the variety caps&turn.
Results: Confirmed Cases
The reasons for arriving at a diagnosis of
confirmed mycosis in 17 of the 510 cases are
indicated in Table 1. Of these patients (3.3
per cent of those examined), 1 had aspergillo-
sis, 2 had cryptococcosis, 3 had histoplasmo-
sis, and 11 had paracoccidioidomycosis.
Aspergillosis
A male patient 72 years of age with
aspergilloma in the upper lobe of the right
lung was operated on for bronchial carcino-
ma. Direct examination and culturing of sur-
gically removed material permitted identifi-
cation of the agent as Aspergillus fumigatus.
Cryptococcosis
One of the two diagnosed cryptococcosis
cases involved a lesion at the same location,
the same radiologic findings, and the same
diagnosis of bronchial carcinoma as did the
case of aspergillosis. However, surgery was
avoided when the mycosis was diagnosed on
the basis of direct examination and the results
of sputum culture. The other case involved a
patient admitted with a clinical picture of
acute meningoencephalitis. Radiology re-
vealed a shadow on the lung, a shadow that at
autopsy proved to be a gelatinous mass of
Cryptococcus neoformans. lo The two patients,
men 55 and 39 years of age, respectively, both
lived in Caracas.
Histophsmosis
A thoracotomy was performed on a woman
23 years of age in order to remove an asymp-
tomatic nodule from her left lung for diagnos-
tic purposes. The extracted material was not
cultured, but histologic study revealed
elements morphologically definable as Histo-
plasma capsulatum.
Camjhs et al. l MYCOSES IN PATIENTS WITH ABNORMAL X RAYS 53
Another patient, a man 78 years old, was
admitted to the hospital with a pulmonary X
ray picture of granulitis and an ulcerated
tongue. H. capsulatum was isolated from the
tongue ulcer.
The third patient, a girl 8 years of age, was
placed under clinical observation for meningi-
tis. Immunodiffusion (ID) and complement
fixation (CF) tests suggested histoplasmosis.
The disease subsequently spread. The
presence of H. capsulatum in the lung and other
organs was confirmed at autopsy.
In the first of these cases the serologic tests
were negative; in the second the ID test
revealed positive H and M bands, 1 1 and the
CF test yielded titers of 1:64 and 1:16,
respectively, with fllamentous-phase and
yeast-phase antigens of H. capsulatum. In the
third case the ID test showed a positive H
band, and the CF titers with the filamentous-
phase and yeast-phase antigens were 1:256
and 1:64, respectively.
Paracoccidioidomycosis
Seven patients’ X rays showed active or
fibronodular lesions in both lungs; three other
patients had unilateral infiltrates, and one had
a right hilar image suggesting adenopathy. All
these patients were between 14 and 5 1 years of age, and all except one (a woman 36 years old) were males.
Ten of the 11 patients had lesions at other sites as well. These included dermal and buc-
copharyngeal lesions, superficial adeno-
pathies, orchitis, and a brain abcess that was operated on as a brain tumor. In all cases the
presence of the fungus was confirmed by
“Of the six antigenic components discovered by Heiner (29) in histoplasmin, the so-called h and m are found regularly in blood serum of persons with active histoplasmosis. Their presence is detected with methods that make the precipitation bands visible; these appear in agar gel when pukied antigens (30) come in &tact with the corresponding antibodies of patients’ sera. The test may reveal an H-band, an M band, or H and M bands. Patients with H band are usually in the acute, progressive stage of histoplasmosis. Those with M band are considered as being in the chronic stage of the disease or having an old infection.
direct examination, by culture of material
from the various lesions, or by both methods.
One patient showed only pulmonary lesions.
Multi-budded forms of P. brasiliensis were
found in sputum specimens from this patient that had been treated with Grocott stain, but
the organism was not successfully cultured.
In all 11 cases the ID tests yielded positive
results only with the causative organism. As
Table 1 shows, most of the CF tests yielded positive results with both the yeast-phase and
filamentous-phase antigens of Paracoccidioides
brasiliensis. However, three cases yielded rela- tively low titers (1:8 or 1: 16) and one was
negative with yeast-phase antigens, and four
likewise yielded low titers (1:8 or 1: 16) with
filamentous-phase antigens. One patient,
whose ID test was positive for P. brasiliensis but
whose CF test yielded low titers (0 with the
yeast-phase antigen of P. bmsiliensis and 1:16
with the filamentous-phase antigen), also
showed a CF titer of 1: 8 with the filamentous-
phase antigen of H. capsulatum.
We consider that a positive ID test and CF results such as those seen in these 11 cases
(where the disease was confirmed) provide in-
formation of high diagnostic value in cases
where mycological confirmation of P. bmsilien-
sis infection is not possible. We also feel that
such findings justify provision of treatment on
a trial basis, in view of the fact that appropri-
ate medicaments are available, effective, gen-
erally well-tolerated, and easy to administer.
Such trial treatment appears advisable even in
cases where another firmly supported diagno-
sis is available, because it is not unusual for
another or multiple etiologies to exist concur-
rently.
Results: Unconfirmed Cases
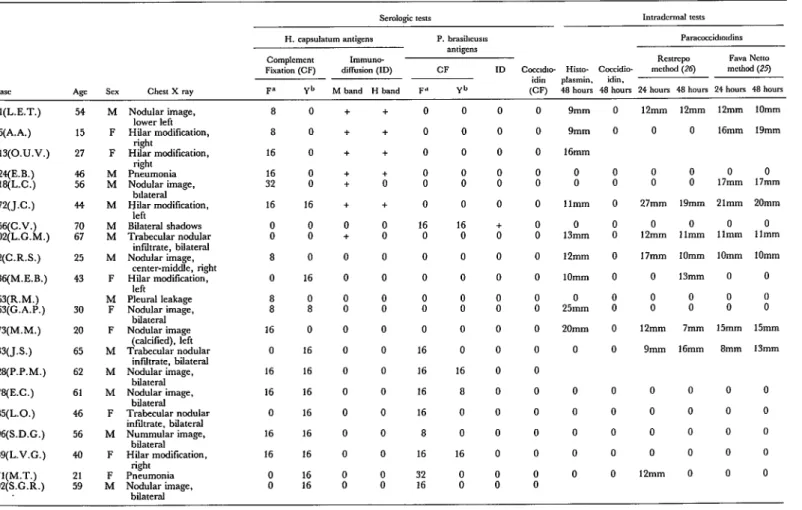
Table 2 summarizes the information about
21 additional cases that involved a variety of
pulmonary lesions and positive serologic tests,
although the hospital’s regular resources did
not permit a definite diagnosis of mycotic
disease. These 21, like the 17 patients cited above, were examined carefully at the Vargas
Table 2. Diagnostic findings for 21 patients with possible mycotic disease.
Semlogic tern Intradennal tcxs
H. caps&mm antigens P. brasibcusls Paracrrcidndinr
antigens
Complcmcnt Immune
RCSlXTpo
Fava NcttoFixation (CF) diflusion (ID) CF ID Cocadn- Hirto- Coccidio- mcrhod (26) method (25) idin plasmin. idin,
F= Yb M band H band Fd Yb (CF) 48 hours 48 hours 24 houn 48 hours 24 hours 48 hours Si(L.E.T.) 6qA.A.) 213(O.U.V.) 22qE.B.) 318(L.C.) 472(J.C.) 52cqz%) 92(C.R.S.) 13qM.E.B.) 263(R.M.) 363(G.A.P.) 473(M.M.) 133(J.S.) 22qP.P.M.) 378(E.C.) 385(L.O.) 396(S.D.C.) 439(L.V.G.) 471(M.T.) 392(S.G.R.) 54 15 27 46 56 44 i: 25 43 30 20 65 62 61 46 56 40 :-!I M F F iti M ii M F M F F M M M F M F F M
Nodular image, lower left Hilar modiIication,
right
Hilar modification, right
Pneumonia Nb~aod;;imagee, Hilar modification,
left
Bilateral shadows Trabecular nodular
infdtrate, bilateral Nodular image,
center-middle, right Hilar modification,
left Pleural leakaee Ncdular ima&
bilateral Nodular image
(c&&d), left Trabecular nodular
infdtrate, bilateral Nodular image,
bilateral Nodular image,
bilateral Trabecular nodular infdtrate. bilateral Nummular image,
bilateral H;!laat modification, Pn&onia Nodular image,
bilateral 8 8 16 16 32 16 0 0 8 0 : 16 0 16 16 0 16 16 : 0 0 0 : 16 0 0 0 16 0 8 0 16 16 16 16 16 16 16 16 + + + + + + 0 + 0 0 0 0 0 0 0 0 0 0 0 i
+
+
+
d
+
0 0 0 0 0 0 0 0 0 0 0 0 0 : 0 0 0 0 0 0 16 0 0 0 0 0 0 16 16 16 16 8 16 32 160 0
0 0
0 0
: i
0 0
16 +
0 0
0 0
0 0
0 0
0 0
0 0
0 0
16 0
8 0
0 0
0 0
16 0
: : 0 0 0 0 0 0 i 0 0 i 0 0 0 0 0 0 0 0 0 9mm 9mm 16mm 0 0 llmm 0 13mm 1Omm 0 25mm 20mm 0 0 0 0 0 0 0 0 0 0 i 0 0 0 0 0 0 0 12mm 0 i 27mm 0 12mm 17mm 0 0 0 12mm 9mm 0 0 0 0 12mm 12mm 0 : 19mm 0 1 lmm 1Omm 13mm 0 0 12mm 16mm 0 17mm 21mm 0 llt%lltl 1Omm 0 i 15mm 1Omm 19mm 0 17mm 20mm 0 llmm 1Omm 0 i 15mm 13mm
aFiiamentous-phase antigen.
Campins et al. l MYCOSES IN PATIENTS WITH ABNORMAL X RAYS 55
reveal some of the possible causes of their
pulmonary lesions. In cases where the patient
was expectorating, cytological studies were
conducted and a search was made for fungi
and Koch’s bacillus. In some cases, material
obtained in the course of a bronchoscopy or
lung biopsy was studied. An effort was also
made to see all the patients frequently and at
regular intervals, but not all of them kept their appointments.
The cases listed in Table 2 can be separated
into two diagnostic categories. The first cate-
gory of cases (including the top seven shown)
yielded positive CF and ID results with either
H. capsulatum or P. brasiliensis antigens. (Six of
the seven patients showed results positive for
H. caps&turn; one showed CF results positive for P. bra&e& and a positive ID response to paracoccidioidin.)
When testing yields results such as these,
we believe there are grounds for making a
serologic diagnosis of the particular mycosis in
question. We also consider that these results
provide grounds (1) for trial antimycotic treat-
ment in possible cases of paracoccidioidomy- cosis and (2) for observing the evolution of the
problem in the case of histoplasmosis-if other
possible etiologies have been ruled out and if
the patient has active pulmonary lesions.
The second diagnostic category of cases in
Table 2 includes the other 14 patients, whose sera yielded positive results in either the CF or ID test but not in both. One of these patients
gave a positive ID M-band response to H. cap-
sulatum antigen; five yielded low positive CF
responses to one or both H. cap&alum an-
tigens; and eight yielded positive CF re-
sponses to both H. capsdatum and P. brasiliensis
antigens (these latter results suggest cross-
reactions).
It is our opinion that results such as these
give grounds for keeping the patient under
clinical-radiologic and serologic observation
for mycotic disease until such time as a
definite diagnosis has been made.
Sera from patients listed in Table 2 and most of those listed in Table 1 were tested by
ID and CF as indicated on page 54.
All skin tests with coccidioidin were
negative. Similarly, with one exception all the
sera yielded negative results when tested by
CF with the filamentous-phase antigen of C.
immitis. The sole exception was serum from
the girl who died of disseminated histoplasmo-
sis (see Table 1), in whom a reaction of 1: 16 to this antigen was recorded.
Only one of the three histoplasmosis cases
listed in Table 1 received a histoplasmin skin
test. That one test, given to a patient with a
pulmonary nodule, yielded a negative result.
Of the 11 patients with proven paracocci-
dioidomycosis, five showed responses measur-
ing 1 Omm or more with the two intradermal I?
brasiliensis antigens, and three of these five
showed responses measuring over 10mm to
histoplasmin. Of the six other patients, one
gave a 9mm response to the Restrepo antigen; another gave an 8mm response to the Fava
Netto antigen; the other four patients with
paracoccidioidomycosis yielded negative
results.
Eighteen of the 2 1 patients listed in Table 2
were skin-tested with Restrepo and Fava
Netto antigens. Of these, 10 showed responses measuring between 9 and 2 1 mm; it should be noted, however, that most of those responding
positively also gave a positive serologic re-
sponse to H. caps&turn antigen, and that the
one patient in this group with positive CF and
ID responses to P. brasiliensis yielded negative
results.
In addition, 139 patients with negative
serologies (of 486 originally tested) responded
positively to one or both of these antigens. In
those cases, as in the cases discussed above,
the differences between the two P. brasiliensis
antigens (in terms of ability to evoke a positive
response) were not sufficiently marked to sug-
gest that one might be more suitable than the other.
In this same vein, Fava Netto (31) has
reported obtaining a positive response with
polysaccharide paracoccidioidin (2.5) in 77 per
cent of 100 patients with diagnosed paracocci-
dioidomycosis, and a positive response in 67
per cent with filtered paracoccidioidin (26). In
addition, Restrepo has asserted that “the
56 PAHO BULLETIN l vol. 15, no. 1, 1981
pears better than the earlier ones” (32). Res- trepo has also reported (33) that she obtained a positive response from 44 of 56 patients with
confirmed paracoccidioidomycosis by using a
cellular paracoccidioidin composed of poly-
saccharides and proteins; 42 of these 56 pa-
tients responded positively to the Fava Netto
antigen ( 25).
Conclusions
Overall, the serologic and intradermal tests
performed provided valuable diagnostic infor-
mation. In particular, we found that in all 11
cases where P. brasiliensis was isolated from a patient’s lesions, that patient’s serum yielded
positive CF and ID results with P. brasiliensis
antigen. Since only one other suspected case
yielded such results (see Table 2), this indi- cates that, taken together, positive CF and ID
tests for paracoccidioidomycosis justify treat-
ment-even when the agent’s presence has
not been otherwise confirmed.
Regarding the 21 patients listed in Table 2,
it also appears that the positive CF and ID results obtained in the first seven cases (with
either H. capsulatum or P. brasiliensis antigens)
would provide grounds for making a positive
serologic diagnosis- even without confirma-
tion derived from pulmonary lesions. Such a
diagnosis would justify trial treatment if the
suspected agent was P. brasiliensis and con-
tinued observation if the suspected agent was
H. capsulatum- if other etiologies have been ruled out, and if the patient has active pulmo- nary lesions.
Sera from the other 14 patients in Table 2
gave negative ID responses but responded
positively by CF to one or another of the anti- gens tested. In these cases, the limited positive response gives grounds for keeping the patient
under observation until a definite diagnosis is
made.
ACKNOWLEDGMENTS
We wish to thank Angela Restrepo, Ph.D., Pulmonary Disease Service and the Mycology
Demosthenes Pappagianis, M.D., Ph.D., and Section (Institute of Pathological Anatomy) at
Hugo David, M.D., Ph.D., for supplying Vargas Hospital in Caracas, and to the
Paracoccidioides, Coccidioides, and Histoplasma laboratory staff of the Jose Ignacio Bald6 Na-
antigens, respectively. tional Tuberculosis Institute in the same
We are also grateful to the staffs of the city.
SUMMARY
A study was made of 510 patients with abnormal chest X ray findings at Venezuela’s Vargas Hospi- tal in order to obtain precise pathological data about possible mycotic disease. The study entailed both serologic testing (by complement furation and
immunodiffusion) and intradermal testing for COC-
cidioidomycosis, paracoccidioidomycosis, and
histoplasmosis.
Radiologic evidence, direct microscopic exami- nations, and cultures led to a positive diagnosis of deep mycosis in 17 of the 510 cases. These included 11 paracoccidioidomycosis cases, 3 histoplasmosis
cases, 2 cryptococcosis cases, and 1 case of asper- gillosis. The diagnoses of paracoccidioidomycosis and histoplamosis were confirmed by results of the serologic and intradermal tests.
In 21 other cases, the serologic tests yielded some
positive results-even though the other methods
used did not provide grounds for a clear diagnosis of mycotic disease. In the absence of other diag- nosed etiologies, these results appear to provide justification for either trial treatment or continuing
observation-depending on the nature of the sero-
Camfiins et al. l MYCOSES IN PATIENTS WITH ABNORMAL X RAYS 57
REFERENCES
(1) Montiel, S. El primer case de actinomicosis
comprobado en el Zulia. La Benejicencia. Maracai-
bo, Venezuela, September 1908.
(2) Fonseca, M. Actinomicosis (Paper presented on 14 August 1908 to members of the Sociedad
Vargas). Gaceta Medica de Caracas 23172, 1916.
(3) R&gel, R. Epitelioma y actinomicosis. Guce-
ta Medica de Caracas 16:61, 1909.
(4) Pino Pou, R. Sobre un case de micetoma de
granos negros . Vargos (Caracas) 8:298, 1917.
(5) Vegas, M. Primer case de esporotricosis en
Venezuela. Rev&a de la Policlinica Caracar 21:13,
1935.
(6) JimGnez Rivero, M., and L. Briceiio Irago- rry. La esporotricosis y el primer case de rhinocla-
diosis schenckii en Venezuela. Gaceta Medica de
Caracas 43:225, 1936.
(7) Bricefio b-agony, L. Un nuevo case de espo- rotricosis. Rev&a de la Policlinica Caracas 35~2345,
1937.
(8) O’Daly, J. A. Las blastomicosis en Venezue- la. Boletin de 10s Iiosfiitales de Caracas 36~127, 1937. (9) Iriarte, D., and C. Rodriguez. Un case de
granulomatosis paracoccidioidica o blastomicosis
brasilera. Revista de la Clinica Luis Razetti 2:209,
1939. \
(10) Guerra, P. El granuloma a paracoccidioi-
des, su importancia en patologia pulmonar. Revista
de Sanidad y Asistencia Social (Caracas, Venezuela)
5:921, 1940.
(11) O’Daly, J. A. Las cromoblastomicosis.
Rev&a de la Policlinica Caracas 44:2300, 1938. (1.2) Briceiio Iragorry, L. Sobre cromoblastomi- cosis. Rev&a de la Clinica Luis Rozetti 2: 108, 1938.
(23) Campins, I-E., M. Scharyj, and V. Gluck.
Coccidioidomicosis (enfermedad de posadas): Su
comprobaci6n en Venezuela. Archives Venetolanos de
Patologia Tropical y Parasitologia Medica 1: 2 15, 1949. (14) Campins, H., M. Scharyj, and J. R. Cor- tCs. Coccidioidomicosis en Venezuela: Relaci6n de1 Segundo case estudiado. (Sesiones DermatoQicas, homenaje al Prof. Luis E. Pierini; Buenos Aires,
November 1949.) Lopez y Etchegoyen S.R.L.,
Junin 863, Buenos Aires, Argentina, 1950, pp.
73-78.
(15) Campins, H. Coccidioidomicosis: Un
nuevo problema de salud piiblica en Venezuela.
Revista de Sanidad y Asislencia Social (Caracas, Venezuela) 15:1, 1950.
(16) Potenza, L., and E. Benaim Pinto. Obser- vaciones en Venezuela de dos cases de torulopsis
(Criptococcus neofrmans) en el sistema nervioso cen-
tral. Archives Venezolanos de Patologia Tropical y Parasitologia Medica 1~235, 1949.
(17) Campins, H., and M. Scharyj. Investiga- ci6n de la sensibilidad cut&ea a la histoplasmina
en Venezuela. Archives Venezolanos de Patologia
Tropical y Parasitologia Medica 2:75, 1950.
(18) Campins, H., and M. Scharyj. Comproba-
ci6n de la histoplasmosis en Venezuela. Gaceta
Medica de Caracas 61:67, 1953.
(19) Pollak, L., C. Rodriguez, and M. Adrian- za. Histoplasmosis pulmonar: Presentaci6n de un
case. Acta Medica Venezolana 1~242, 1953.
(20) Archila, R. BibliograJa Medica Venezolana
(2nd edition). Editorial Bellas Artes. Caracas,
1955.
(21) Archila, R. Bibliograji’a Medica Venezolana
(3rd edition). Imprenta National, Caracas, 1960.
(22) VtYez Boza, F., and H. Vegas Rodriguez.
Bibliografia mkdica de1 profesorado de la Facultad de Medicina, 1964-1968. Comisidn de Biblioteca y
Publicaciones de1 Consejo de la Facultad de
Medicina, Caracas, 1970.
(23) Silva Alvarez, A., and J. M. Llopis. Biblio-
graf;a mkdica Venezolana, 1965-1967. Ministerio de Sanidad y Asistencia Social, Caracas, 1973.
(24) Kerdel Vegas, F. Bibliografa dermatol6gica
Venezolana. Editorial Arte, Caracas, 1966. (25) Fava Netto, C., and A. Raphael. A reacgo
intradermica con polisacaride do Paracoccidioides
brasiliensis na blastomicose sul americana. Rev Znst Med Trap Sgo Paul0 3(4):161-165, 1961.
(26) Restrepo-Moreno, A., and J. D.
Schneidau. Nature of the skin-reactive principle in
culture filtrates prepared from Paracoccidioides
brasiliensis. J Bacteriol93:1741-1748, 1967.
(27) Kwon-Chung, K. J. Emmonsiella capsulata:
perfect state of Histoplasma capsulatum. Science
177:368-369, 1972.
(28) Kwon-Chung, K. J. A new genus, Filobari-
diella, the perfect state of Cryptococcus neoformans. Mycologia 67:1197-1200, 1975.
(29) Heiner, D.C. Diagnosis of histoplasmosis using precipitin reactions in agar gel. Pediatrics 22:
616-627, 1958.
(30) Bradley, G., L. Pine, M. W. Reeves, and W. MOSS. Purification, composition, and serologi- cal characterization of histoplasmin H and M an-
tigens. Infection and Immunip 9: 870-880, 1974.
(31) Fava Netto, C., M.A.G. Guerra, and E. 0. da Costa. Contribuclo ao estudo immunol6gico da paracoccidioidomicose: Rea$%oes intradermicas em pacientes con dois antgenos hom6logos e dois
heter6logos. Rev Inst Med Trap Sgo Paul0 18: 186-190,
1976.
(32) Restrepo. A. Paracoccidioidomicosis. Acta
Medica Colombiana 3~33-36, 1978.
(33) Negroni, R., et al. Preparacidn y estudio de
un antigen0 celular de P. brasiliensis Gtil para