USE OF THE BIFURCATED
NEEDLE FOR BCG
VACCINATION
OF NEWBORN!3’9 ’
Leone1 Rojas S.,’ J. M. Borgok
D.,4 Elsa Hh~ras,~ Ximena Ferrer,5
Ximena Valero,5 Luisa Miranda,6 and Teresa Lincoqueo6
It has been suggested that the bifurcated needle technique used successfully against smallpox might be gainfully employed in BCG vaccination of newborns against tuberculosis. The two Chilean studies described here were conducted in order to assess its potential in this regard and to reexamine the previously reported technical difficulties involved.
Introduction
The bifurcated needle affords a simple means of vaccination that has been used successfully against smallpox (I, 2). Indeed, the simplicity of this technique is regarded as one of the factors which contributed sig- nificantly to smallpox eradication on the Asian Continent.
Shortly before completing the massive phase of smallpox vaccination in Asia and in some African countries, the idea arose of employing the existing organization of mobile vaccination teams to conduct a campaign against tuberculosis using the same bifurcated needle technique. This would eliminate the need for retraining personnel in new vaccination techniques and procedures.
Before deciding to use the bifurcated needle for BCG vaccination, however, it was judged essential to compare its technical efficacy with that of the intradermal
IAlso appearing in Spanish in Bol Of Sand Panam 83(Z), 1977.
ZThis study was financed by a grant from the Tuberculosis Unit of the World Health Organization.
SEpidemiology Section, Chilean National Health Service.
khief, Health Protection Division, Chilean Na- tional Health Service.
BNurse, Southern Area Santiago, Barros Luco Hospital.
CMidwife, Central Area Santiago, Salvador and San Borja Hospitals.
technique-the best of the currently avail- able methods. The comparison was made by various investigators on the basis of tubercu- lin sensitivity and vaccinal skin lesions.
Studies were made of children in India (3), Cameroon (4), The Central African Republic (5), Tanzania (6), and Mexico (7). In no case, even with BCG vaccine concentrations of 160 mg per ml, did the effectiveness of the bifurcated needle tech- nique match that of the intradermal method. At best, it was estimated that the actual BCG vaccine dose which penetrated the subjects was only one-third of the intra- dermally injected dose. Furthermore, the results were observed to vary significantly from one subject to the next, a circumstance appreciably reducing the reliability of the method.
If the technical efficacy of bifurcated needle vaccination could be improved to a point where half of the standard intrader- ma1 dose penetrated the subject, and if variations introduced by different vaccina- tors could be reduced, this would then be the ideal method for BCG vaccination of the newborn. In fact, it has been recom- mended for some time that the dose administered to newborns and infants should be half the standard dose in order to avoid local complications such as abscesses and satellite adenopathies (8).
Therefore, two consecutive studies were
designed and carried out in order to further test the effectiveness of the bifurcated needle in BCG vaccination of the newborn. This article presents the results of those studies.
Study I
Materials and Methods
The first study was performed in 1975 in the maternity wards of the Barros Luco, San Borja, and Salvador hospitals in Santiago, Chile. A total of 895 newborns were vaccinated with either the intradermal or the bifurcated needle technique without any prior tuberculin testing.
The vaccines employed were as follows: a) Freeze-dried BCG vaccine from Japan at a concentration of 80 mg per 1.0 ml. This was administered with the bifurcated needle technique. Since each ampule contained 80 mgof vaccine, 1.0 ml of diluent was added
’ to achieve the required concentration.
b) An international reference prepara- tion of BCG vaccine was furnished by the Serum Institute of Copenhagen, Denmark. This was administered by the intradermal route and was used in two concentrations, the standard dose and half the standard dose.
The vaccines were evaluated at the Chilean Bacteriological Institute. It was found that the number of viable particles per ml in samples taken at the time of vaccination did not vary significantly from the viability indicated by the producing laboratories. This was taken to indicate that the products had been properly preserved and transported.
The intradermal vaccination, adminis- tered with an Omega Syringe, introduced 0.1 ml of vaccine at standard or half- standard strength into the outer face of the left arm, 2 cm below the top of the shoulder, in accord with WHO standards (9).
The multiple puncture vaccination was
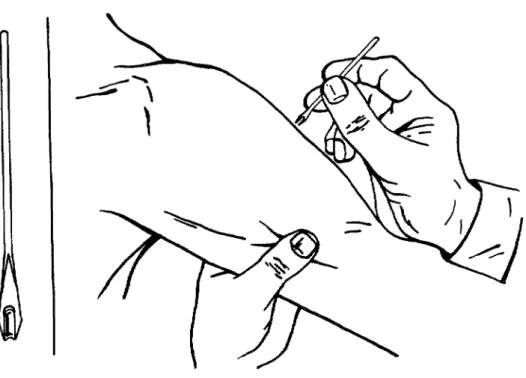
cated needle into the vaccine vial in such a way that, on withdrawal, a droplet of vac- cine remained on the prong fork. Nine vertical punctures were then made in the skin of the subject’s arm at the same site used for the intradermal injections. The bifurcated needles were sterilized with dry heat. Figure 1 shows this vaccination proce- dure.
The vaccinations were administered by two midwives with many years’ experience in giving intradermal vaccinations, six nursing auxiliaries who had previously administered smallpox vaccinations with the bifurcated needle, and two nurses skilled at applying and reading the tubercu- lin test.
The vaccination schedule for the study was established by random selection of the hospitals and the days for vaccination with the bifurcated needle, the standard intra- dermal dose, and the half-standard intra- dermal dose.
Post-vaccinal evaluation was accom- plished by means of a tuberculin test administered five months after vaccination. This test employed 2 tuberculin units of PPD RT 23 with polysorbate 80 (tween 80).
Results
The results of the study were analyzed with the assistance of the Departments of Biostatistics and Public Health of the University of Chile.
Rojas et al. l BCG VACCINATION OF NEWBORNS 127
Figure 1. Vaccination with the bifurcated needle.
The needle is held perpendicular to the subject’s arm.
A droplet of vaccine is suspended The vaccinator’s wrist rests on
in the fork of the needle. the subject’s arm.
Source: World Health Organization, Document WHO/SE/68.2 Rev. 1.
sensitivity. This finding agrees with other published observations (20).
On the other hand, the average tubercu- lin sensitivity shown by those subjects vaccinated with the bifurcated needle was only 4.9 mm, indicating that the amount of vaccine inoculated by this method was ap- proximately one-tenth the standard dose. When the results obtained with the bifur- cated needle were compared with those obtained by injecting half the standard
dose, the difference was found to be signifi- cant. It was therefore concluded that the vaccine concentration was too weak, or else the number of punctures made was insuffi- cient to achieve the desired effect.
Table 1. Tuberculin reactions observed in Study I, five months after BCG vaccination of newborns.
Vaccination technique
No. of newborn subjects
Post-vaccinal tuberculin reaction Average Standard induration deviation
(mm) Intradermal, standard
dose
Intradermal, l/2 standard dose
Bifurcated needle Total
169 7.6 4.6
144 6.3 4.6
582 4.9 3.8
895 - -
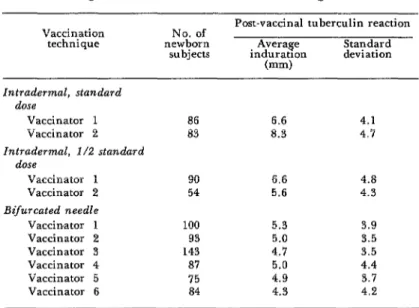
cy of the method. It was felt that if several individuals could obtain virtually identical results, this would indicate that the tech- nique could be applied easily with a minimum of variability. An overall statisti- cal analysis was therefore made of differ- ences in the results obtained by each of the six vaccinators using the bifurcated needle. This analysis found that none of the observed differences were statistically signi-
ficant. Contrary to the results of previous research on schoolchildren, this supports the conclusion that variations introduced by individual vaccinators in the present study were within acceptable limits and would not constitute grounds for objection to the use of this technique.
On the other hand, it is interesting to note that statistically significant differences were observed in the results obtained by the
Table 2. Tuberculin reactions observed in Study I, broken down according to the individual workers administering vaccine.
Vaccination
technique newborn No. of subjects
Post-vaccinal tuberculin reaction Standard Average
induratron deviation (mm)
Intradermal, standard dose
Vaccinator 1 Vaccinator 2 Intrademnal, l/2 standard
dose
Vaccinator 1 Vaccinator 2 Bifurcated needle
Vaccirrator 1 Vaccinator 2 Vaccinator 3 Vaccinator 4 Vaccinator 5 Vaccinator 6
86 6.6 4.1
83 8.3 4.7
90 6.6 4.8
54 5.6 4.3
100 5.3 3.9
93 5.0 3.5
143 4.7 3.5
87 5.0 4.4
75 4.9 3.7
Rojas et al. l BCG VACCINATION OF NEWBORNS 129
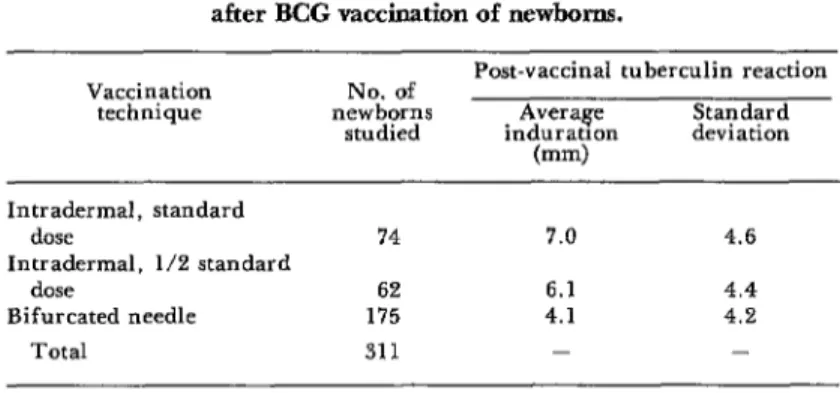
Table 3. Tuberculin reactions observed in Study II, five months after BCG vaccination of newborns.
Vaccination technique
Post-vaccinal tuberculin reaction No. of
newborns Average Standard studied induratIon deviation
(mm) Intradermal, standard
dose
Intradermal, l/2 standard dose
Bifurcated needle Total
74 7.0 4.6
62 6.1 4.4
175 4.1 4.2
311 - -
two vaccinators using the intradermal method-both of whom were experienced in the use of the technique.
No complications were observed in con- nection with any of the methods employed.
Study II
Because of the poor results obtained from the first study-in terms of the efficacy of the bifurcated needle for BCG vaccina- tion-it was decided to conduct a second study in which two modifications were introduced. Specifically, a vaccine concen- tration of 160 mg per ml was selected (0.5 ml of diluent in an ampule containing 80 mg of dry BCG powder), and the number of needle punctures was increased from nine to fifteen. No modifications were made in the doses used with the intradermal method.
Table 3 shows the principal data obtained from this study, which was completed in 1976 and which involved vaccination of 311 newborns. Despite the use of double-strength vaccine and the increased number of skin punctures, the relationships between the results obtained with the three different procedures remained essentially the same as those obtained in the first study. In this case, however, it could be estimated that the average amount of vaccine introduced into the subject with the bifurcated needle was even less than one-tenth of the standard intradermal dose.
Discussion and Conclusions
Most Latin American countries have established appropriate BCG vaccination policies. Nevertheless, for a variety of reasons it has not been possible to achieve effective BCG coverage, so that the present vaccination coverage of children under one year of age in Latin America is only about 25 per cent (II). One of the reasons for this poor coverage is the difficulty of training personnel to administer vaccine by the intradermal method.
Multiple puncture vaccination with a bifurcated needle can be performed by personnel with only basic preparation and a minimum of training; hence the interest in continued investigation of the technical capabilities of this method.
In conclusion, the bifurcated needle less, its evident functional advantages make
1 technique cannot yet be recommended for it worthwhile to continue exploring the BCG vaccination of newborns. Neverthe- technical possibilities of this method.
SUMMARY
The bifurcated needle vaccination method used successfully against smallpox is a relatively simple technique that can be administered by personnel with only basic preparation and a minimum of training. This fact suggests that it could prove useful in campaigns of BCG vaccination against tuberculosis-especially for vaccination of newborns. With this end in mind, two studies were carried out in Santiago, Chile, to examine previously reported difficulties with the method and to assess its potential as an alternative to the best current method, that of intradermal inoculation.
These studies indicated that previously re-
ported variations in the results achieved by different vaccinators could be markedly re- duced. However, they also found that the bifurcated needle method did not cause a suffi- ciently large dose of vaccine to enter the subject-even when fifteen needle strokes and a highly concentrated vaccine (160 mg per ml) were employed. It was thus concluded that although modification of the needle or other changes might ultimately yield satisfactory results, the bifurcated needle technique cannot yet be recommended for BCG vaccination of newborns.
REFERENCES
(I) World Health Organization. SmalZ~ox Eradication. WHO Document WHO/SE/71.30, pp. 225-227 Appendix 1. Geneva, 1971.
(2) Ladnyi, I.D. Studies of Smallpox Vaccina- tion by Bifurcated Needles in Kenya. WHO Document WHO/SE/68.7. Geneva, World Health Organization, 1968.
(3) Narain, R., et al. Results of BCG vaccina- tion with the bifurcated needle. Indian J Med
Res 62(10): 1596-1600, 1974.
(4) Gateff, C., et al. Contribution to the study of BCG vaccination by the multiple pressure technique with a bifurcated needle. Bull Znt Union Tuberc 48 (Suppl): 28-36, 1973.
(5) World Health Organization. BCG Vacci- nation by Bifurcated Needle. WHO Document WHO/TB/Working Paper/73.5. Geneva, 1973.
(6) Vaughan, J. P., et al. Percutaneous BCG immunization trial using the WHO bifurcated
needle. J Trap Med Hyg 76:143-146, 1974. (7) Senties R. Personal Communication. (8) GUM J ., et al. Suppurative lymphadenitis following intradermal BCG vaccination of the newborn. Br Med J 2:1048-1054, 1955.
(9) World Health Organization. Technical
Guide for Assessment of BCG Vaccination
Programmes. WHO Document WHO/TB/
Techn. Guide/Z, Rev. 4. Geneva, 1965. (10) Edwards, L., et al. Effect of Diluting BCG Vaccine and the Significance of Dead Organisms. WHO Monograph Series No. 12. Geneva, World Health Organization, 1953, pp.
125-141.
(II) Pio, A. The Current State of BCG