www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Glucose
metabolism
disorders
and
vestibular
manifestations:
evaluation
through
computerized
dynamic
posturography
夽
Roseli
Saraiva
Moreira
Bittar
a,∗,
Maruska
D’Aparecida
Santos
a,
Raquel
Mezzalira
baDepartmentofOtoneurology,HospitaldasClínicas,FaculdadedeMedicina,UniversidadedeSãoPaulo(FM-USP),SãoPaulo,SP,
Brazil
bDepartmentofOtorhinolaryngology,HeadandNeckSurgery,UniversidadeEstadualdeCampinas(UNICAMP),Campinas,SP,Brazil
Received1November2014;accepted26May2015 Availableonline6November2015
KEYWORDS
Dizziness;
Glucosemetabolism disorders;
Diet carbohydrate-restricted
Abstract
Introduction:Globalsugarconsumptionhasincreasedinthepast50years;itsabusiveintakeis responsibleforperipheralinsulinresistance,whichcausesthemetabolicsyndrome---obesity, diabetesmellitus,hypertension,andcoronaryheartdisease.
Objective:To evaluate the effect of afractionated diet without glucose as treatment for labyrinthinedisordersassociatedwithglucose---insulinindex.
Methods:Thestudydesignwasaprospectiverandomizedcontrolledtrial.Fifty-onepatients weredividedintotwogroups:thedietgroup(DG),whichcomprised subjectstreatedwitha fractionateddietwithglucoserestriction,andthecontrolgroup(CG),inwhichindividualswere notcounseledregardingdiet.Patientsunderwentcomputerizeddynamicposturography(CDP) andvisualanalogscale(VAS)onthefirstand30thdaysofthestudy.
Results:There was improvement in the assessed posturographic conditions and VAS self-assessmentintheDGgroupafter30dayswhencomparedtothecontrolgroup.
Conclusion:Thefractionateddietwithglucoserestrictionwaseffectiveforthetreatmentof vestibulardysfunctionassociatedwithglucosemetabolismdisorders.
© 2015 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
夽
Pleasecitethisarticleas:BittarRSM,SantosMA,MezzaliraR.Glucosemetabolismdisordersandvestibularmanifestations:evaluation throughcomputerizeddynamicposturography.BrazJOtorhinolaryngol.2016;82:372---6.
∗Correspondingauthor.
E-mail:[email protected](R.S.M.Bittar).
http://dx.doi.org/10.1016/j.bjorl.2015.10.005
PALAVRAS-CHAVE
Tontura; Transtornosdo metabolismode glicose;
Dietacomrestric¸ão decarboidratos
Distúrbiosdometabolismodaglicoseemanifestac¸õesvestibulares:avaliac¸ãopela posturografiadinâmicacomputadorizada
Resumo
Introduc¸ão: Oconsumomundialdeac¸úcartriplicounosúltimos50anoseasuaingesta abu-sivaéresponsávelpelaresistênciaperiféricaàinsulinaqueoriginaasíndromemetabólica ---obesidade,diabetesmellitus,hipertensãoarterialedoenc¸ascoronarianas.
Objetivo: Avaliardeformaobjetivaoefeitodadietafracionadaesemglicosecomoformade tratamentodosdistúrbioslabirínticosassociadosàsalterac¸õesdacurvaglicoinsulinêmica.
Método: Trata-sedeumensaioclínicocontroladorandomizadoprospectivo.Estudorealizado com51pacientesdivididosemdoisgrupos:GrupoDietacompostoporindivíduostratadoscom dietafracionadacomrestric¸ãodeglicoseeGrupoControlenoqualosindivíduosnãoforam ori-entadosemrelac¸ãoàdieta.OspacientesrealizaramPosturografiaDinâmicaComputadorizada eEscalaAnálogoVisualnoprimeiroetrigésimodiasdoestudo.
Resultados: Foiobservadamelhoranascondic¸õesposturográficasavaliadas emelhoraclínica do grupodieta naanálisedaescala análogovisual quandocomparadosgrupodieta egrupo controle.
Conclusão:A dieta fracionada e restritiva de glicose mostrou-se eficaz no tratamentodas disfunc¸õesvestibularesassociadasaosdistúrbiosdometabolismodaglicose.
© 2015 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Globalsugarconsumption hastripledinthepast50years,
anditsabusive intakeisresponsible for peripheral insulin
resistance,whichleads tothemetabolic syndrome---
obe-sity, diabetes mellitus, hypertension, and coronary heart
disease.1,2Anestimated40%ofindividualswithweight
con-siderednormaldevelopsomeformofmetabolicsyndrome,
asaresultofglucoseconsumption.3Accordingtothesame
authors, in the United States the situation hasbecome a
matterofnationalsecurity,asyoungindividualsare
becom-ingincreasinglyobeseandunfitformilitaryservice.
The significanceofglucosemetabolismdisorders(GMD)
can be observed in otoneurology when their high
preva-lenceisobservedinpatientswithlabyrinthdisorders.4Itis
estimatedthatbetween30%and90%ofpatientswith
dizzi-nesshave alteredlevelsofbloodglucoseandinsulin.5---8 In
recent years,several authors have investigated GMDas a
causeofinnereardysfunctions.4,5,7,9,10Moreover,vestibular
dysfunctionhas been described asa new complicationof
diabetes andacts asa potentiating riskfactor forfalls in
thesepatients.11
Basedontheaboveobservations,itwasdecidedtoassess
thepostural performanceofpatients withdizzinessand a
clinicalhistoryofGMDafterafractionateddietwithglucose
restriction,inordertotestthehypothesisthatthisdietis
effectiveinthetreatmentofvestibulardysfunctions
associ-atedwiththiscondition.Theaimsofthisstudyincluded:
1. Assess theposturography conditions ona moving
plat-form (conditions 4, 5, 6) and the composite score
in patients with body balance disorders and glucose
metabolismalterationsbeforeandafterafractionated
dietwithglucoserestrictionfor30days.
2. Assesstheimpactofthefractionateddietwith
carbohy-drate restrictiononthequalityoflife ofpatients with
body balance disorders and glucose metabolism
alter-ationsusingthevisualanalogscale(VAS).
Methods
Thiswasaprospective,randomized,controlledclinicaltrial,
previouslyapproved bythe ResearchEthics Committeeof
theinstitution (No.482/05) andregistered in theClinical
TrialProtocolRegistrationSystem(NTC02,226,536).All
par-ticipantsinthestudysignedtheinformedconsent.
The study subjects were adults older than 18 years.
Theyunderwentallthenecessaryexaminationstoattaina
finaldiagnosisofvestibulardisorder:audiometry,
videonys-tagmography,electrophysiological tests,andimagingtests
when needed. Among these, individuals with dizziness
relatedtofood(fastingand/oraftersugarintake)andwho
hadan alteredthree-hourglucosetolerancetest, namely:
bloodglucose ≤55mg/dL; and/or blood glucosebetween
145and199mg/dL inthesecond hourofthetest and/or;
sumofinsulinlevelsofthesecondandthirdhours>60U/mL
wereselectedforstudy.12---15
Patients with complaints non-attributable to the
ves-tibular system, orthopedic or neurological disorders that
mightinterferewiththecomputerizeddynamic
posturogra-phy(CDP),anddiabeticpatientsaccordingtotheAmerican
DiabetesAssociation (2010and2011)werenotincludedin
thestudy.13,14
Patients diagnosed with vestibular disorders such as
Meniere’s disease (anamnesis supported by the American
Academycriteria)werealsonotincludedinthestudy.
Non-vestibular dizziness symptoms are those without
movementorvertigo), suchas: syncope,visualdarkening,
ataxia,lightheadedness,headpressure.
Therewerenopatientexclusions.
Thesampleconsistedof51patients,42femalesandnine
males,dividedintotwogroups:
1. DietGroup(DG):26individualswhoreceiveda
fraction-ateddieteverythreehourswithsugarrestriction.
2. ControlGroup(CG):25individualswhokepttheirregular
diet.Therewerenodietaryrestrictions.
Patientswerealwaysrandomizedbythesameexaminer,
accordingtothenumericalorderofarrivalattheservice.
Bothgroups wereinstructed toingestacorn starchtablet
(placebo)twiceaday,whichwasdeliveredbythe
investi-gatoratthestartoftheintervention.
All study subjects were asked about the clinical
char-acteristicsoftheirdizziness.Toquantifyself-perceptionof
bodybalance,thesubjectsansweredusingaVAS,inwhich
zero meant no dizziness and ten meant the worst
possi-bledizziness. Postural assessment wasconducted by CDP
throughasensoryorganizationtest(SOT),EquitestSystem®
version4.0(NeuroComInternacional---UnitedStates).
Both the VAS and the SOT were carried out at two
momentsofthestudy:thefirstday(D1)andafter30days,
whenthedietaryinterventionended(D30).
After 30 days, patients in both groups delivered the
packagewiththeplacebotabletssothattheexaminercould
observewhetherthetabletshadbeeningested.Adherence
totheproposeddietarytreatmentwasinvestigatedthrough
thequestion:‘‘Didyoufollowthedailydietasindicated?’’
Statisticalanalysis
Theprimaryvariablesconsidered weretheposturographic
conditions C4, C5, and C6 (conditions 4, 5, 6, which are
platform-oscillatingconditions)and compositescore (CS),
toassesstheimpactofvestibularresponsesandtheireffect
onthefinalposturalmaintenance.4,16---18VASresponseswere
alsoconsidered,characterizingtheself-perceptionof
treat-mentimpactonearlysymptoms.
Forthestatisticalanalysisthefollowingtestswereused:
• Chi-squaredtests.19
• Student’st-test.19
• Fisher’sexacttest.20
• Cochran’stest.19
• Analysisofvariance(ANOVA).19
• Tukey’stest.19
Results
Samplecharacterization
TheDG consisted of26 subjects,meanage of45.8±11.3
years. The CG consisted of 25 patients, mean age of
52±13.7 years. Forty-two patients (82.4%) were females
andnine males(17.6%). The values found showednormal
distribution. When compared by the Student’s t-test and
Fisher’sexacttest,thegroupswerehomogeneousregarding
genderdistribution(p=0.948)andage(p=0.086).
Table1 C4valuesinDGandCGondayoneandday30.
C4 Dayone Day30 p-Value Group Mean±SD Mean±SD
Diet 69.24±15.21 77.09±9.73 0.0128 Control 62.30±14.50 61.94±15.22 0.9991
p-Value 0.0420 0.0002
C4,condition4ofposturography;DG,dietgroup;CG,control group.
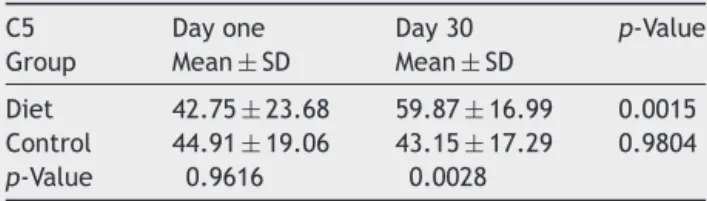
Table2 C5valuesintheDGandCGondayoneandday 30.
C5 Dayone Day30 p-Value Group Mean±SD Mean±SD
Diet 42.75±23.68 59.87±16.99 0.0015 Control 44.91±19.06 43.15±17.29 0.9804
p-Value 0.9616 0.0028
C5,condition5ofposturography;DG,dietgroup;CG,control group.
Table3 C6valuesintheDGandCGondayoneandday 30.
C6 Dayone Day30 p-Value Group Mean±SD Mean±SD
Diet 41.17±18.03 55.23±15.95 0.0024 Control 45.65±18.03 46.93±14.66 0.9874
p-Value 0.6370 0.1390
C6,condition6ofposturography;DG,dietgroup;CG,control group.
Regardingtheclinical characterizationofdizzinessand the results of theglucose tolerance test, the chi-squared and Cochrantestswere used.The most commontypes of dizziness were floating (70.5%) and the feeling of imbal-ance (60%). The most frequent laboratory diagnosis was hyperinsulinemia,presentin76.47%ofcases.Hypoglycemia occurredin21.56%ofthesample.
The ANOVA test was applied to assess variables C4, C5, C6,CS, VAS,andTukey’smultiple comparisons, which identified the significant differences.19 When comparing
posturographicconditionsbeforeandafterthedietperiod,
therewassignificantimprovementintheDGinrelationto
theCGinallofthem,asshowninTables1---4.
Table4 CSvaluesintheDGandCGondayoneandday 30.
CS Dayone Day30 p-Value Group Mean±SD Mean±SD
Diet 64.28±11.37 73.44±8.80 0.0002 Control 64.55±9.62 63.95±10.61 0.9838
p-Value 0.9984 0.0002
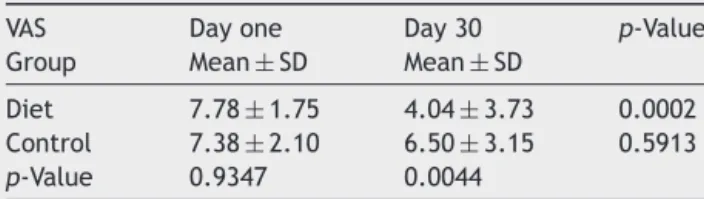
Table5 VASvaluesintheDGandCGondayoneandday 30.
VAS Dayone Day30 p-Value Group Mean±SD Mean±SD
Diet 7.78±1.75 4.04±3.73 0.0002 Control 7.38±2.10 6.50±3.15 0.5913
p-Value 0.9347 0.0044
VAS,visualanalogscale;DG,dietgroup;CG,controlgroup.
A significant improvement was observed in VAS in the DGonday30whencomparedtothefirstdayofthestudy (p=0.0002)andwhencomparedtotheCG(p=0.0044).The resultsareshowninTable5.
Discussion
Themajorityoftheassessedcases(82.4%)belongedtothe
femalegender,similarlytowhatisfoundintheliterature.
Hormonalchangesin womenbetweenthefourth andfifth
decadesoflifemarktheonsetofclimatericperiod,whose
manifestationsmayincludewaterretentionandmetabolic
andanxietydisorders.4,21---23 Inthisagegroup,GMDactsas
amigrainetriggerandcanalsoberesponsiblefortriggering
posturaldisorders.21,24
Anamnesis is crucial for the diagnosis of dizziness of
metabolicorigin,includingGMD.Thecharacteristicsfound
in this sample do not differ fromthose in the literature;
themostprevalentsymptomwasfloating-typedizzinessin
70.5%ofpatients,followedbyimbalancein60%ofcases.4
Theglucosetolerancetestisconsideredthemost
impor-tant diagnostic tool in the assessment of patients with
dizzinessandGDM.6,25,26Whenthemostfrequentlyobserved
alterationsareevaluated,thepresentresultsarenot
dissim-ilarfromthosefoundintheliterature,andhyperinsulinemia
wasthemostcommonabnormality,observed in76.47%of
cases.10,21,27,28 Clinicaltrialshave shownthatthe
fraction-ateddietwithglucoserestrictionplaysanimportantrolein
thetreatmentofpatientswithGMD.1,29,30Therefore,itwas
decideduseadietthatwasfractionatedeverythreehours,
togetherwithglucoserestriction.
The literature reports the importance of the placebo
effect in clinical studies that propose the validationof a
certain treatment.31,32 Approximately 35% of cases show
a positive placebo response, because they generate
bio-logicalphenomenathatmimicpharmacologicaleffects.33,34
Theplacebowasintentionallyadministeredtobothgroups
so that patients would feel treated and followed by the
researcher. This fact allows oneto exclude the diet as a
potentialplacebo, andinstead considerthatthe dietwas
thefactorresponsiblefortheimprovementofthepatients
assessedintheDG.Interestingly,evenwhenexplainingitto
theresearchsubjects,onlyoneofthemquestionedtheuse
ofapillcontainingnotherapeuticeffect.
Atbaseline,abetternumericperformanceinC4ofthe
DGwhencomparedtotheCG(p=0.042)wasobserved.At
the end of the study, the difference found between the
groups at baseline increased to a highly significant value
(p=0.0002).Thevaluescanbeattributedtoimprovement
investibular-visualintegrationafterthediet.Therewasa
significantimprovement inthe DGvaluesonthe 30thday
whencomparedtothefirstmeasurementofC5atbaseline
(p=0.0015). StillinC5,thebettervestibularperformance
oftheDG(p=0.0028)whencomparedtotheCG(p=0.9804)
canbeclearlyobservedonthe30thdayofthestudy.Asfor
C6,animprovementwasalsoverifiedregardingthevalues
observedonthe30thstudydayintheDG(p=0.0024).
InrelationtotheCS,theDGresultsonthe30thdayof
thestudywere higherthanthemeasures obtainedonthe
firstday(p=0.0002),astheywerealsohigheronthe30th
daywhencomparedtotheCG(p=0.0002).
Theresultsdemonstratebetterposturalperformancein
theDGattributedtotheeffectofdietonvestibularfunction
ofthesubjects.Thus,thisstudyreproducedthefindingsof
Bittaret al.(2004),4 whousedCDP todocumentpostural
recoveryimprovementinpatientswithGMDsubmittedtoa
fractionateddietwithglucoserestriction.
The purpose of the VAS was to evaluate the
self-perception of symptom discomfort and quantify their
subjectiveevolutionasaresultofthefolloweddiet.31,35A
significant improvementwas observedregarding the level
of discomfort only in DG patients after 30 days of diet
(p=0.0002),aswellascomparedtotheCG(p=0.0044)in
thesameperiod.Therefore,itcanbeinferredthatthediet
hadapositiveinfluenceontheself-perceptionofdizziness.
Conclusion
Mobileposturography,CS,andVASshowedsignificantly
bet-tervaluesinpatientssubmittedto30daysoffractionated
andglucose-restricteddietwhencomparedtotheControl
Group.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.FukudaY.Insulina,receptordeinsulinaeglucagon.In:Fukuda Y,editor.Ac¸úcar:amigoouvilão?SãoPaulo:Manole;2004.p. 59---66.
2.Rask-MadsenC,King GL.Mechanisms of disease: endothelial dysfunctionininsulinresistanceanddiabetes.NatClinPract EndocrinolMetab.2007;3:46---56.
3.LustigRH,SchimidtLA,BrindisCD.Thetoxictruthaboutsugar. Nature.2012;482:27---9.
4.BittarRSM,BottinoMA,SimoceliL,VenosaAR.Labirintopatia secundáriaaosdistúrbiosdometabolismodoac¸úcar:realidade oufantasia?BrazJOtorhinolaryngol.2004;70:800---5.
5.PowersWH. MetabolicaspectsofMénière’sdisease. Laryngo-scope.1978;88:122---9.
6.ProctorCA,OakR.Abnormalinsulinlevelsandvertigo. Laryn-goscope.1981;91:1657---75.
7.LehrerJF,PooleDC,SeamanM,RestivoD,HartmanK. Identi-ficationandtreatmentofmetabolicabnormalitiesinpatients withvertigo.AnnInternMed.1986;146:1497---500.
8.KnightLC,SaeedSR,HradekGT,SchindlerRA.Insulinreceptors ontheendolymphaticsac:anautoradiographicstudy. Laryngo-scope.1995;105:635---8.
10.Rybak LP. Metabolic disorders of the vestibular system. OtolaryngolHeadNeckSurg.1995;112:128---32.
11.AgrawalY,CareyJP,SantinaCCD,SchubertMC,MinorLloydB. Diabetes,vestibulardysfunction,andfalls:analysesfromthe NationalHealthandNutritionExaminationSurvey.Otol Neuro-tol.2010;31:1445---50.
12.Kraft JR, Nosal A. Insulin values and diagnosis of diabetes. Lancet.1975;305:637.
13.AmericanDiabetesAssociation.Diagnosisandclassificationof diabetesmellitus.DiabetesCare.2010;33:62---9.
14.BaseviV,DiMarioS,MorcianoC,NoninoF,MagriniN.Comment on:AmericanDiabetesAssociationstandardsofmedicalcarein diabetes:2011.DiabetesCare.2011;34:11---61.
15.The Endocrine Society. Workupfor a hypoglycemic disorder. TheEndocrineSociety’s:clinical/guidelines.JClinEndocrinol Metab.2009;94:709---28.
16.Di Fabio RP. Meta-analysis of the sensitivity and specificity ofplatformposturography.ArchOtolaryngolHeadNeckSurg. 1996;122:150---6.
17.RuckensteinMJ,ShepardNT.Balancefunctiontesting:arational approach.OtolaryngolClinNorthAm.2000;33:507---18. 18.OwenBF.Whatcanposturographytellusaboutvestibular
func-tion?AnnNYAcadSci.2001;942:446---64.
19.Maxwell DL, Satake E. Research and statistical methods in communicationdisorders.Baltimore:Williams&Wilkins;1997. 20.MagalhãesMN,LimaACP.Noc¸õesdeprobabilidadeeestatística.
SãoPaulo:Edusp;2000.
21.Mangabeira-AlbernazPL,FukudaY.Glucose,insulinandinner earpathology.ActaOtolaryngol.1984;97:496---501.
22.Fonseca AS, Davidson SAV. Correlac¸ão entre tontura e disfunc¸õesdometabolismodaglicose.BrazJOtorhinolaryngol. 2006;72:367---9.
23.OiticicaJ,BittarRSM.Metabolicdisordersprevalenceinsudden deafness.Clinics(SãoPaulo).2010;65:1149---53.
24.SaccoS,RicciS,DeganD,CaroleiA.Migraineinwomen:therole ofhormonesandtheirimpactonvasculardiseases.JHeadache Pain.2012;13:177---89.
25.VexiauP,LegoffB,CathelineauG.Insulinandcortisolsecretion duringOGTTinpatientswithreactivehypoglycaemiawithor withoutclinicalsymptoms.HormMetabRes.1983;15:419---21. 26.SerraAP, Lopes KC, Dorigueto RS, Gananc¸a FF. Avaliac¸ão da
curvaglicoinsulinêmicanospacientescomvestibulopatia per-iférica.BrazJOtorhinolaryngol.2009;75:701---5.
27.LavinskyL, OliveiraMW,BassanesiHJ,D’AvilaC,LavinskyM. Hyperinsulinemiaandtinnitus:ahistoricalcohort.IntTinnitus J.2004;10:24---30.
28.Kim SH, Reaven GM. Insulin resistance and hypersuline-mia: you can’t have one without the other. Diabetes Care. 2008;31:1433---8.
29.Spencer JTJ. Hyperlipoproteinemia, hyperinsulinism and Ménière’sdisease.SouthMedJ.1981;74:1194---200.
30.Brun JF, Fedou C, Mercier J. Postprandial reactive hypo-glycemia.DiabetesMetab.2000;26:337---51.
31.CollocaL,PetrovicP,WagerTD,IngvarM,BenedettiF.Howthe numberoflearningtrialsaffectsplaceboandnoceboresponses. Pain.2010;151:430---9.
32.AvinsLA, CherkinDC,Sherman KJ,GoldbergH,PressmanA. Should we reconsiderthe routineuseof placebocontrols in clinicalresearch?Trials.2012;13:44.
33.Finness DG, Katchuk TJ, Miller F, Benedetti F. Placebo effects: biological, clinical and ethical advances. Lancet. 2010;375:686---95.
34.Benedetti F. The placebo response: science versus ethics and the vulnerability of the patient. World Psychiatry. 2012;11:70---2.