rev bras ortop.2015;50(6):739–742
w w w . r b o . o r g . b r
Case
report
Fungal
spondylodiscitis
due
to
Candida
albicans
:
an
atypical
case
and
review
of
the
literature
夽
Álynson
Larocca
Kulcheski
a,b,∗,
Xavier
Soler
Graells
a,b,
Marcel
Luiz
Benato
a,b,
Pedro
Grein
Del
Santoro
a,b,
André
Luis
Sebben
a,baOrthopedicsandTraumatologyService,HospitaldeClínicas,UniversidadeFederaldoParaná(UFPR),Curitiba,PR,Brazil
bHospitaldoTrabalhador,UniversidadeFederaldoParaná(UFPR),Curitiba,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received18August2014 Accepted14November2014 Availableonline18October2015
Keywords: Candidaalbicans Discitis Spinaldiseases
a
b
s
t
r
a
c
t
SpondylodiscitisduetoCandidaisararecomplicationfromhematogenicdissemination ofinfectioncausedbythisfungus.Wepresentanatypicalcaseofspondylodiscitiscaused bythisgermthatoccurredafterchestcontusionandprogressedwithnecrotizingfasciitis oftheanteriorregionofthechestandosteomyelitisofthesternum.Throughcontiguity, italsoaffectedtheupperthoracicspine.Thepatientevolvedwithneurologicalalterations andrecoveredsatisfactorilyafterappropriatetreatmentwithsurgicaldecompressionofthe spinalcordandspecificantibiotictherapy.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Espondilodiscite
fúngica
por
Candida
albicans
:
um
caso
atípico
e
revisão
da
literatura
Palavras-chave: Candidaalbicans Discite
Doenc¸asdacolunavertebral
r
e
s
u
m
o
A espondilodiscite por Candida albicans é uma rara complicac¸ão da disseminac¸ão hematogênica da infecc¸ão por esse fungo. Apresentamos um caso atípico de espondilodiscite por esse germe ocorrido após trauma contuso torácico que cursou com fasceíte necrotizante da região anterior do tórax, osteomielite de esterno e, por contiguidade,afetouacolunavertebraltorácicaalta.Opacienteevoluiucomalterac¸ão neu-rológicaerecuperou-sesatisfatoriamenteapóstratamentoadequadocomdescompressão medularcirúrgicaeantibioticoterapiaespecífica.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevierEditora Ltda.Todososdireitosreservados.
夽
StudycarriedoutattheOrthopedicsandTraumatologyService,HospitaldeClínicas,UniversidadeFederaldoParaná(UFPR)and HospitaldoTrabalhador,UniversidadeFederaldoParaná(UFPR),Curitiba,PR,Brazil.
∗ Correspondingauthor.
E-mails:[email protected],[email protected](Á.L.Kulcheski). http://dx.doi.org/10.1016/j.rboe.2015.10.005
740
rev bras ortop.2015;50(6):739–742Fig.1–Initialaspectofthesternumlesion.
Introduction
Spinalcordinfectionsare rareandcompriseapproximately 1% of bone infectious involvement.1 Most of these
infec-tionsareofpyogenicortuberculousorigin.Fungalinfections are increasing, but are still extremely rare and occur more as opportunistic infections in immunocompromised individuals.2 Despite the increased frequency, infection by
Candidaalbicansisnotcommon.3Wereportanunusualcaseof
thoracicspondylodiscitiscausedbyC.albicans.Theliterature wasreviewed,aimingtobetterunderstandingthesubject.
Case
report
Thepatient was a39-year-old homeless, chronic alcoholic maleindividual.HefelltwometerstothegroundinOctober 2012.Hewastreatedinatraumahospital,whereheshowed signs of septicshock, hyperemia and crackles in the ster-nalregion, with 10cm indiameter. Chest radiography and computedtomography(CT)showedpre-sternalsubcutaneous emphysemaandsignsofsternumfracture,andculminated withadiagnosis ofanterior chest wallnecrotizingfasciitis (Fig.1).Surgicaldebridementwasperformedinthisregion. Theresultoftheofsternumsofttissueculturewaspositivefor
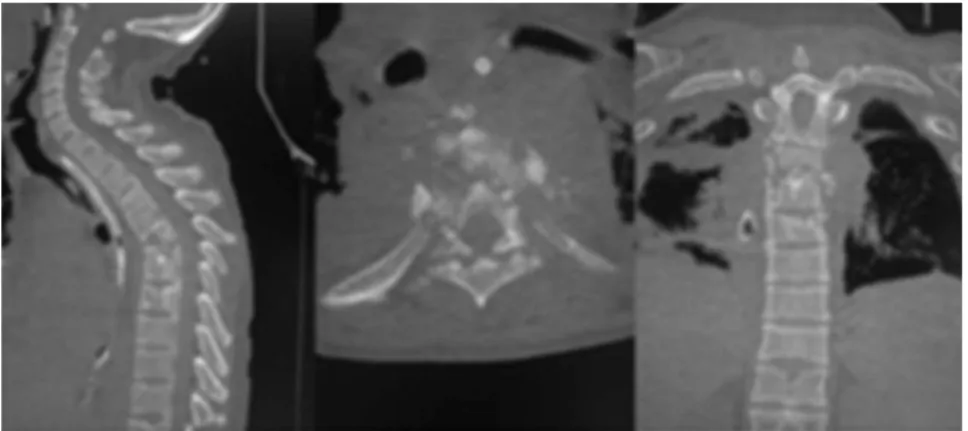
Fig.3–CobbangleinthepreoperativeperiodbetweenT2 andT7.
multisensitiveEscherichiacoliandtheresultofthesternalbone fragmentcultureforC.albicanswaspositive.Treatmentwith fluconazole(6mg/kg/day)andCiprofloxacin(400mg12/12h) wasstartedanddrugusewasscheduledforsixmonths, ini-tially intravenouslyand,afterclinicalimprovement,byoral route. Thepatient developed vertebral osteomyelitis signs, with decreasedheight ofthe vertebral bodiesand discs at thethoracicspinelevelsofT4–T5–T6(Fig.2).Thepatientwas paralyzed,withalteredsensitivityattheT4level,compatible withFrankelB.InitialCobbangleof68◦(Fig.3)wasobserved.
Thepatientunderwentthoracotomy,whichdisclosedaspinal abscessandalargeamountofpurulentsecretion.A corpec-tomywasperformedfromT4toT6withautologousiliacgraft replacementandcomprehensivespinaldecompressioninT4. There wasimprovementofpaincomplaintsinthethoracic spine,withfeverdisappearanceandimprovementtoFrankel
rev bras ortop.2015;50(6):739–742
741
Fig.4–postoperativeAPandprofileradiographies.
C.Atasecondprocedure,hewassubmittedtoposterior fix-ationandarthrodesiswithpediclescrewsatthelevelofthe thoracicspinefromT3toT7(Fig.4).
Postoperatively,heshowedimprovementof13◦of
kypho-sisintheCobbangleandremainedat55◦(Figs.4and5).After
eightmonthsofthediagnosis,thepatientshowed improve-mentoftheneurologicalleveltoFrankelDattheT4level. Uponassessmentat12monthsafterthefirstdiagnosis,the woundswerehealedandheshowedsignificantimprovement inthethoracickyphosis(Fig.5).Thepatientwaswell, com-municative,independentinrelationtoself-care,andmanaged toperformhisactivitieswithoutassistanceordifficulty. Dur-ing hospitalization the Oswestry Disability Index 2.0 was appliedpreoperatively andafterthe definitivesurgical pro-cedure.Preoperatively,hescored 70%and wasclassified as disabled.Postoperatively,theindexwas25%,whichshowed goodresultsinthepain/disabilityitem.
Discussion
Despitetheincreaseinthefrequencyoffungemia,infectionby C.albicansisalsoararecauseofspinalinfection.3Themain
riskfactorsare:priorantibiotictherapy,ICUstay,long-term catheteruse,corticosteroids,intravenousdrugs,transplants andchemotherapy.1,2,4,5Inourcase,thepatientwasalcoholic,
homelessandimmunocompromised.
ThemostcommonlocationofspondylodiscitisbyCandida isinthelumbarspine,andthepresenceofneurologicaldeficit isinfrequent.2
In2001,Miller6 described59casesofspinalinfectionby
Candida,33affectingthelumbarspine,17thechest,threethe cervicalandsixboththethoracicandlumbarspine.
In ourcase,the upperthoracicregionwas affected and therewasneurologicaldeficit,incontrasttotheliterature.This
742
rev bras ortop.2015;50(6):739–742conditionisusuallyinsidious.Themostusefulclinical find-ingispainintheaffectedarea,bothboneandparavertebral types.7Theparaplegiawasnoteworthyinourcase.An
asso-ciationwasobservedbetweenchest traumaandthe spinal injury,afactvalidatedbyliterature.8
WhenC.albicansaffectsthespine,itusuallycausesdisk narrowing,destructionoftheendplatesandthesubjacent ver-tebralbone.4Theseimagingfindingsareconsistentwithwhat
wefoundinourcase.
Theoptimized managementofspinalinfectionsby Can-didaremainsunclear.Casereportssuchasthisonehelpto increasetheexperienceinthemanagementandtreatmentof thisdisease.
Surgicaltreatmentisnotrequiredinspondylodiscitisby Candida. However, it should be performed in cases where thereisneurologicaldeficitandvertebralinstability.4,5Inthe
presentreport,the patienthadneurologicaldeficit(Frankel B)andvertebralinstability,characterizedbykyphosingofthe thoracicspine.
Clinical treatment is carried out with antifungal drugs, usingamphotericinBorfluconazole.Oneproposedtreatment consistsof 6–10 weeks ofAmphotericin BIV at a dose of 0.5–0.6mg/kg/day.9StudieshaveshownthatFluconazoleisas
effectiveasamphotericin,showinghighersafetyand tolera-bility.Inourinstitution,wechosetocarryoutthetreatment withfluconazole.
Studies have documented that diagnostic delay is common.10 That is attributed to the rare occurrence and
difficulty in cultivating the microorganisms. It has been suggestedthatadelay inthestart ofantifungaltherapy is associated with a worse outcome, particularly the neuro-logical one.10 Webelieve that our success was due to the
earlydiagnosisandconfirmationbybiopsyandthesternum bone culture, as well as the identification of spinal cord compression.Thetreatmentwaspromptlycarriedout with spinaldecompression,rapidmicrobiologicalresultsandstart ofspecificantifungaltreatment.
Spondylodiscitis by Candida should be considered in immunocompromised patients. The definitive diagnosis is
achievedthroughisolationofC.albicansinbloodorcultures. Theantifungaltreatmentoftenresultsinthe cure,evenin casesofdelayeddiagnosis.Whenthereisneurological insta-bilityordeficit,surgicaltreatmentshouldbeconsidered.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.GhanayemAJ,ZdeblickTA.Cervicalspineinfections.Orthop ClinNorthAm.1996;27(1):53–67.
2.BronerFA,GarlandDE,ZiglerJE.Spinalinfectionsinthe immunocompromisedhost.OrthopClinNorthAm. 1996;27(1):37–46.
3.JohnsonMD,PerfectJR.Fungalinfectionsofthebonesand joints.CurrInfectDisRep.2001;3(5):450–60.
4.GatheJCJr,HarrisRL,GarlandB,BradshawMW,WilliamsTW Jr.Candidaosteomyelitis.Reportoffivecasesandreviewof theliterature.AmJMed.1987;82(5):927–37.
5.AlmekindersLC,GreeneWB.VertebralCandidainfections.A casereportandreviewoftheliterature.ClinOrthopRelatRes. 1991;267:174–8.
6.MillerDJ,MejicanoGC.Vertebralosteomyelitisdueto Candidaspecies:casereportandliteraturereview.ClinInfect Dis.2001;33(4):523–30.
7.SmithAS,BlaserSI.Infectiousandinflammatoryprocessesof thespine.RadiolClinNorthAm.1991;29(4):809–27.
8.GraellsXS,ZaninelliEM,Collac¸oIA,NasrA,CecílioWAC, BorgesGA.Thoracicinjuriesandspinaltrauma:acomplex association.Coluna/Columna.2008;7(1):8–13.
9.RexJH,WalshTJ,SobelJD,FillerSG,PappasPG,DismukesWE, etal.Practiceguidelinesforthetreatmentofcandidiasis. InfectiousDiseasesSocietyofAmerica.ClinInfectDis. 2000;30(4):662–78.