ww w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Case
report
Intracerebral
hemorrhage
with
a
favorable
outcome
in
a
patient
with
childhood
primary
angiitis
of
the
central
nervous
system
Marco
Felipe
Silva
a,
Ana
Raquel
Feitosa
a,
José
A.
Paz
b,
Nádia
Emi
Aikawa
a,c,
Clovis
A.
Silva
a,c,∗aPediatricRheumatologyUnit,FaculdadedeMedicina,UniversidadedeSãoPaulo,SãoPaulo,SP,Brazil
bPediatricNeurologyUnit,FaculdadedeMedicina,UniversidadedeSãoPaulo,SãoPaulo,SP,Brazil
cDivisionofRheumatology,FaculdadedeMedicina,UniversidadedeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received20December2013 Accepted21May2014
Availableonline30November2015
Keywords:
Childhoodprimaryangiitis Centralnervoussystem Vasculitis
Intracerebralhemorrhage Stroke
a
b
s
t
r
a
c
t
Childhoodprimaryangiitisofthecentralnervoussystem(cPACNS)isarareinflammatory braindiseaseofunknownetiology.Ofnote,brainhemorrhagehasbeenrarelyreportedin cPACNSpatients,generallyassociatedwithadelayedclinicaldiagnosis,orwithadiagnosis onlyatnecropsy.WepresentthecaseofaboywithcPACNSthatpreviouslysufferedan ischemicstroke.Attheageof7yearsand10months,hepresentedasuddenandsevere headache,vomitingandreductioninconsciousnesslevel(Glasgowcomascale7),requiring prompttrachealintubation.Braincomputedtomographydemonstratedintraparenchymal hematomaintheright parieto-occipitallobeandasmallfocusofbleedingintheright frontallobe,vasogenicedema,herniationoftheuncusanda10mmdeviationtotheleft fromthemidline.C-reactiveprotein(9.2mg/dL)andvonWillebrandfactor(vWF)antigen (202%)wereelevated.Decompressivecraniotomywasperformedandmethylprednisolone andcyclophosphamidewereadministered.Oneweeklater,thepatienthadlefthemiparesis withoutothersequelae.Importantly,motordeficitshavebeenimprovingprogressively.Our casereinforcestheinclusionofthisvasculitisasadifferentialdiagnosisinchildrenand adolescentswithCNShemorrhage.
©2014ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Hemorragia
intracerebral
com
evoluc¸ão
favorável
em
paciente
com
angiíte
primária
do
sistema
nervoso
central
juvenil
Palavras-chave:
Angiíteprimárianainfância Sistemanervosocentral
r
e
s
u
m
o
Angiíteprimáriadosistemanervosocentraljuvenil(APSNCJ)éumadoenc¸ainflamatória cerebralraraedeetiologiadesconhecida.Hemorragiacerebraltemsidoraramente repor-tadaempacientescomAPSNCJ,geralmenteassociadacomatrasodiagnóstico,oucomum
∗ Correspondingauthor.
E-mail:[email protected](C.A.Silva). http://dx.doi.org/10.1016/j.rbre.2014.05.007
Vasculite
Hemorragiaintracerebral Acidentevascularencefálico
diagnósticosomentepornecrópsia.Relata-seumcasodeumpacientedogêneromasculino comAPSNCJequepreviamentesofreuumacidentevascularcerebralisquêmico.Aos7anos e10mesesdeidade,omeninoapresentousubitamentecefaleiaintensa,vômitosereduc¸ão doníveldeconsciência(escalade comadeGlasgow7),requerendo imediataintubac¸ão traqueal.Umatomografiacomputadorizadacerebraldemonstrouhematoma intraparen-quimatosonoloboparieto-occipitaldireitoeumpequenofocodesangramentonolobo frontaldireito,edema vasogênico,herniac¸ãodoúncuse umdesviode10mm dalinha médiaparaaesquerda.AproteínaC-reativa(9.2mg/dL)eofatorantígenodevon Wille-brand(202%)estavamelevados.Foirealizadaumacraniotomiadescompressiva,seguida pelaadministrac¸ãodemetilprednisolonaeciclofosfamida.Transcorridaumasemana,o pacienteapresentavahemiparesiaesquerda,semoutrassequelas.Édignodenotaqueo
déficitmotortemmelhoradoprogressivamente.Nossocasoreforc¸aainclusãodessa
vas-culitecomodiagnósticodiferencialemcrianc¸aseadolescentescomhemorragiadosistema nervosocentral.
©2014ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Vasculitidesarecharacterizedbyinflammationandnecrosis ofendothelium.1Theycanaffectbloodvesselsofanyorgan
andsystem,includingthecentralnervoussystem(CNS).CNS vasculitismostoftenissecondarytoanunderlyingcondition, suchasinfectious,neoplastic,vascular,metabolicor inflam-matorydisorders,butitalsocanbeidiopathic.2,3
Ofnote,childhoodprimaryangiitisoftheCNS(cPACNS)is arareinflammatorybraindiseaseofunknownetiologythat occurs inpreviously healthy children. Ithas protean clini-calmanifestations,suchasseizures, cognitivedysfunction, behaviorchanges,headaches,neurologicdeficitsandstrokes.3
Ischemicstrokeseemstooccurmoreoftenthan hemor-rhagicevents,whichareseldomdescribedintheliterature. Asfarasweareconcerned,onlysevencaseswerereported regardinghemorrhagic strokeandcPACNS inthe literature, mostofwhichhaddelayedclinicalornecropsydiagnosis.1,4–8
We describe a patient with cPACNS and intracerebral hemorrhagesubmittedtopromptdrainageand immunosup-pressivetherapywithgoodprognosis.
Case
report
At the age of 7 years and 2 months, a boy presented
intenseheadacheduringabout5minuteswithspontaneous improvement.Inthe nexttwenty-four hours,hehadlabial commissure deviationto the rightside and left hemipare-sis,beinghospitalizedinanotherhospital.Laboratoryexams were:hemoglobin12.7g/L,hematocrit36%,whitebloodcell count10,300/mm3(neutrophils39%,lymphocytes52%,
mono-cytes 5%and eosinophils 4%),platelets 300,000/mm3, urea
30mg/dL(normalrange10-50),creatinine0.53mg/dL(normal range0.32-0.60),C-reactiveprotein(CRP)1.1mg/dL(normal< 5),erythrocytesedimentationrate(ESR)7mm/1sthour
(nor-malrange 0-20) and activated partialthromboplastin time 27.2 s, International NormalizedRatio (INR)1.1. Homocys-teinelevels were 5.5micromol/L(normal range 5-15),total cholesterol176mg/dL(normal<200),low-densitylipoprotein
cholesterol 112mg/dL (normal<100), high-density lipopro-tein cholesterol 49mg/dL (normal > 40) and triglycerides 79mg/dL(normal<150). Brainmagneticresonance imaging (MRI) showed ischemic areas in the right middle cerebral arteryterritory,characterizedbysubcorticalfociofrestricted diffusion in the nucleocapsular region, whereas carotid andvertebralmagneticresonanceangiography,conventional angiographyandcarotidDopplerultrasoundwere unremark-able, aswell ascerebrospinalfluidanalysis.Immunological tests were positive for antinuclear antibodies (ANA) 1:80 (finedense speckledpattern)and negativeforother serum antibodies:anti-doublestrandedDNA(anti-dsDNA),anti-Sm, anti-RNP,anti-Ro,anti-La,anticardiolipinIgM,anticardiolipin IgG,lupusanticoagulant,anti-2-glycoprotein-1and antineu-trophil cytoplasmicantibodies.Urinalysiswas normal, and blood culture was negative. Protein C (115%), protein S (126%) and factor VIII(87%)activities were withinthe nor-malrange.FactorVLeidenmutationandprothrombingene polymorphismwerebothabsent.Aspirin(5.0mg/kg/day)was introduced,andafter4monthsofrehabilitation physiother-apy, complete recoveryof the motor deficits was achieved and aspirin was withdrawn. At the age of 7 years and 8 months, he returned asymptomatic in an outpatient visit, bringing a new brain MRI that revealed encephalomala-cia in the right nucleocapsular region and leptomeningeal enhancementintheleftprecentralsulcus,leftcentralsulcus, rightoccipitalsulcus,sphenoid portionofthe rightSylvian fissureandinferioraspectofthecerebellarhemispheres, com-patible with CNS angiitis(Fig. 1). Prophylactic aspirin was reintroduced, andhewasreferred toourUniversity Hospi-tal. Atthat moment,the patient did nothave complaints. He hadnormal weightand heightdevelopment.Peripheral artery pulses were palpable, there was no claudication of extremities,andblood pressurewas99×65mmHg,without
differencesinthelimbs.Noright-leftshuntwasobserved dur-ingechocardiographywithmicrobubbles,CRPwas0.9mg/dL, and ESRwas11mm/1st hour.Atthe age of7years and 10
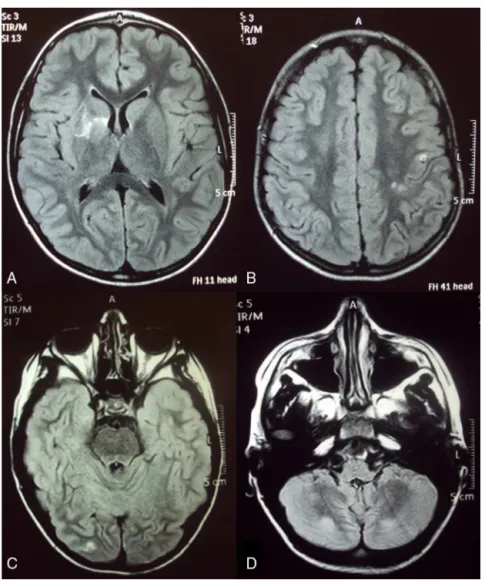
Figure1–MRIshowinggliosis(A),paramagneticcontrastenhancementintheleptomeningealcompartment(leftprecentral sulcus,leftcentralsulcus,rightoccipitalsulcus–BandC)andhyperintenselesionsinvolvinginferioraspectofthe
cerebellarhemispheres(D).
the right parieto-occipital lobe (Fig. 2) and a small focus ofbleedingintheright frontlobe,vasogenic edema,uncal herniationand a10mmdeviationfrom the midline tothe left. Decompressive craniotomy was promptly performed, and cerebral specimen was obtained for histopathological study.Methylprednisolonepulsetherapyforthreeconsecutive days (1.0g/day) was administered, followed by cyclophos-phamide500mg/m2ofbodysurface.Laboratorytestsshowed
hemoglobin13.1g/L,hematocrit39.7%,whitebloodcellcount 23,300/mm3(neutrophils88%,lymphocytes5%,monocytes6%
and 1%eosinophils),platelets 352,000/mm3, urea 23mg/dL,
creatinine 0.37mg/dL,ESR 8mm/1st hour, activated partial
thromboplastintime0.91s,andINRwas1.27.TheCRPwas ele-vated(9.2mg/dL),andvWFantigenwas202%(normalrange 50-160%).Newimmunologicaltestsfordetectionof anticardi-olipinIgM,anticardiolipinIgGandlupusanticoagulantwere persistentlynegativeinthreeoccasions.Biopsyrevealedlarge quantityofbloodclotscontainingseveralfragmentsof cere-braltissuewithgliosis,withnoevidenceofactivevasculitis. Afteraweekofhospitalization,hestillhadlefthemiparesis, but noother sequelae;hewas dischargedwithprednisone
2mg/kg/day.Onemonthaftertheneurosurgery,prednisone wastaperedto1.5mg/kg/day,andanewdoseof cyclophos-phamide500mg/m2wasadministered.ThevWFantigenwas
108%,andESR,5mm/1sthour.Importantly,motordeficitsare
progressivelyimproving,withverylightlefthemiparesisand lefthemianopsia,withoutapparentcognitivedysfunction.
Discussion
WedescribehereinacaseofcPACNSthatpresented hemor-rhagiceventwithafavorableoutcomeafterpromptdrainage andimmunosuppressivetherapy.TheassociationofcPACNS andhemorrhagicstrokehasbeenreportedonlyinsevencases intheliterature,mostlywithpooroutcomeassociatedwith deathorseveredisabilities.1,4–8
Figure2–Intraparenchymalhematomaintheright parieto-occipitallobe.
Ofnote,cPACNSisdiagnosedaccordingtoCalabrese crite-ria: acquired unexplained neuropsychiatric deficit, classic angiographicorhistopathologicfeaturesofCNSangiitisand no evidence of systemic vasculitis.3 Recently, it has been
proposedtwoclinicalsubdivisionsforthisdisorder:small ves-sel vasculitis (SV-cPACNS) or angiography-negative cPACNS andlargeandmedium-sizedvesselvasculitis,alsoknownas angiography-positivecPACNS.2
Approximately30%ofbiopsiesperformedinchildrenwith suspectedSV-cPACNSwerenegative.2Thefirstchoicetobrain
biopsyinthispopulationisinnon-dominantfrontallobe.The absenceofvasculitisobservedinthehistologicfindingsofour patientmightbeexplainedbyasampleofinadequate loca-tion atthe edgeofthe hematomawithconsequent gliosis predominance,probablyduetotheemergencyneurosurgical procedure.
MRIisanavailable tooltoidentifylesions ofactive SV-cPACNS.2 Although there is no pathognomonic radiologic
finding,patientswithangiography-negativec-PACNSusually exhibitmultifocal lesionsaffectingmorethan onecerebral vesselterritory.9Indeed,Benseler etal.reportedfour cases
ofbiopsy-confirmedSVc-PACNSandallofthepatientshad multifocalinjuriesinvolvingbothgrayandwhitematter,9
sim-ilarlyasobservedinthepresentcase.
Regarding clinical manifestations, SV-cPACNS has been reportedwithseizures,cognitivedysfunction,headachesand rarelywithintracranial hemorrhage.10 Large-and
medium-sizedvesselssubtypeshowspredominantlymotordeficitsand speechchanges,andpositiveangiographyisthefundamental toolforitsclassification.10
Interestingly,theinflammatorymarkers,suchasCRPand ESR,mayhelptoassessdiseaseactivity,althoughtheseexams may oscillateduring the disease course.The vWF antigen hasbeendescribedasareliablebiomarkerforpatientswith active systemic vasculitis. It is a plasma protein synthe-sizedbymegakaryocyticandanendothelialcellthatreaches higher levelsin thepresenceofdamaged or inflamed vas-cular endothelium.2,11 Moreover, increased levels of vWF
antigenwerereportedin65%ofc-PACNSpopulation. Remark-ably,theselevelsdecreasedsignificantlyaftertreatment,as observedherein.11
Additionaldetectionsofantiphospholipidantibodieswere prospectivelycollected,sincetheseantibodiesmayfluctuate duringthediseasecourse,reachingnon-detectablelevelsat theacutevascularevents.12
The early neurosurgical treatment in conjunction with immunosuppressant provided favorable outcome for our patient.Indeed,thetherapyforSV-cPACNSincludesinduction withglucocorticoidsandintravenouscyclophosphamide dur-ingthefirstsixmonthsandsubsequentmaintenancetherapy withmycophenolatemofetilfor18months.2,3
In conclusion, we reported a favorable prognosis in a SV-cPACNS patient with brainhemorrhage, reinforcing the inclusionofthesevasculitisasadifferentialdiagnosisin chil-drenandadolescentswithCNShemorrhage.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
ThisstudywassupportedbyFundac¸ãodeAmparoàPesquisa doEstadodeSãoPaulo–FAPESP(grant#08/58238-4toCAS), Conselho Nacional de Desenvolvimento Científico e Tec-nológico–CNPq(302724/2011-7toCAS),FedericoFoundation toCASandNúcleodeApoioàPesquisa“SaúdedaCrianc¸aedo Adolescente”daUSP(NAP-CriAd).Wethankthecolleaguesof IntensiveCareUnitofCentroMédicodeCampinas.
r
e
f
e
r
e
n
c
e
s
1.PistracherK,GellnerV,RieglerS,SchöklerB,ScarpatettiM, KurschelS.Cerebralhaemorrhageinthepresenceofprimary childhoodcentralnervoussystemvasculitis–areview.Childs NervSyst.2012;28:1141–8.
2.CellucciT,BenselerSM.Diagnosingcentralnervoussystem vasculitisinchildren.CurrOpinPediatr.2010;22:731–8. 3.IannettiL,ZitoR,BruschiS,PapettiL,UlgiatiF,NicitaF,etal.
Recentunderstandingondiagnosisandmanagementof centralnervoussystemvasculitisinchildren.ClinDev Immunol.2012;2012:698327.
4.GallagherKT,ShahamB,ReiffA,TournayA,VillablancaJP, CurranJ,etal.Primaryangiitisofthecentralnervoussystem inchildren:5cases.JRheumatol.2010;28:616–23.
5.GreenanTJ,GrossmanRI,GoldbergHI.Cerebralvasculitis:MR imagingandangiographiccorrelation.Radiology.
6. KumarR,WijdicksEF,BrownRDJr,ParisiJE,HammondCA. IsolatedangiitisoftheCNSpresentingassubarachnoid haemorrhage.JNeurolNeurosurgPsychiatry.1997;62: 649–51.
7. MatsellDG,KeeneDL,JimenezC,HumphreysP.Isolated angiitisofthecentralnervoussysteminchildhood.CanJ NeurolSci.1990;17:151–4.
8. NishikawaM,SakamotoH,KatsuyamaJ,HakubaA, NishimuraS.Multipleappearingandvanishinganeurysms: primaryangiitisofthecentralnervoussystem.Casereport.J Neurosurg.1998;88:133–7.
9. BenselerSM,deVeberG,HawkinsC,SchneiderR,TyrrellPN, AvivRI,etal.Angiography-negativeprimarycentralnervous systemvasculitisinchildren:anewlyrecognized
inflammatorycentralnervoussystemdisease.Arthritis Rheum.2005;52:2159–67.
10.CellucciT,TyrrellPN,SheikhS,BenselerSM.Childhood primaryangiitisofthecentralnervoussystem:identifying diseasetrajectoriesandearlyriskfactorsforpersistently higherdiseaseactivity.ArthritisRheum.2012;64:1665–72. 11.CellucciT,TyrrellPN,PullenayegumE,BenselerSM.von
Willebrandfactorantigen–apossiblebiomarkerofdisease activityinchildhoodcentralnervoussystemvasculitis? Rheumatology(Oxford).2012;51:1838–45.
12.CamposLM,KissMH,D’AmicoEA,SilvaCA.
Antiphospholipidantibodiesandantiphospholipidsyndrome in57childrenandadolescentswithsystemiclupus