Artigo Original
Kátia de Freitas Alvarenga1 Leticia Cristina Vicente1 Raquel Caroline Ferreira Lopes1 Luzia Maria Pozzobom Ventura1 Maria Cecília Bevilacqua1 Adriane Lima Mortari Moret1
Descritores
Eletroisiologia Audiologia Potenciais evocados auditivos Implante coclear Percepção da fala Plasticidade neuronal
Keywords
Electrophysiology Audiology Evoked potentials, auditory Cochlear implantation Speech perception Neuronal plasticity
Correspondence address:
Kátia de Freitas Alvarenga Departamento de Fonoaudiologia da Faculdade de Odontologia de Bauru da Universidade de São Paulo
Alameda Dr. Octávio Pinheiro Brisola, 9-75, Bauru (SP), Brazil, CEP: 17012-901. E-mail: [email protected]
Received: 05/28/2013
Accepted: 10/25/2013
Study carried out at the Universidade de São Paulo – USP – Bauru (SP), Brazil. (1) Universidade de São Paulo – USP – Bauru (SP), Brazil.
Financial support: National Council for Scientiic and Technological Development (CNPq).
Conlict of interests: nothing to declare
in children presented with sensorineural hearing loss
following cochlear implantation: a longitudinal study
Desenvolvimento do potencial evocado auditivo cortical
P1 em crianças com perda auditiva sensorioneural após o
implante coclear: estudo longitudinal
ABSTRACT
Purpose: To assess the characteristics of P1 component in children presented with pre-lingual hearing loss, users of cochlear implants, and correlate them with speech perception performance. Methods: Ten children presented with pre-lingual sensory neural hearing loss using cochlear implants participated in this research. The cortical auditory evoked potential research was carried out with the /da/ speech stimulus, presented in free ield, in three moments: at cochlear implant activation, with three and six months following activation. The Infant-Toddler Meaningful Auditory Integration Scale was used to verify the speech perception. Results: The correlation of the three moments of the test with the latency and the amplitude of P1 component through analysis of variance were observed. The comparison of latency and amplitude of P1 in each assessment moment was performed with Tukey’s test. Wilcoxon and t-test showed that the score on the Infant-Toddler Meaningful Auditory Integration Scale increased signiicantly with the time of cochlear implant use, nevertheless with no correlation with the latency and amplitude of P1 component in the moments assessed, as demonstrated by Spearman’s and Pearson’s correlations. Conclusion: The latency and amplitude of P1 component diminish as the time of cochlear implant use increases. However, there was no correlation between its development and speech perception performance.
RESUMO
INTRODUCTION
In the irst years of life, an individual’s central auditory system goes through a sensitive period of development. Sensory deprivation, consequential of hearing losses, in this period can alter or prevent central auditory development(1), which prompts
cortical reorganization. In this scenario, auditory structures, initially responsible for auditory functioning, respond to other sensory stimuli, such as those of visual nature, for instance(2).
Alternatively, the introduction of auditory stimulation through electronic devices, such as cochlear implants, in indi-viduals with more accentuated hearing losses can partially or totally revert the effects of this sensory deprivation and redirect these structures to their primary function. Consequently, the development of auditory abilities, a prerequisite for oral lan-guage acquisition and production, is also enabled(3).
The changes that occur in central auditory pathways, after the activation of cochlear implants, can be veriied by means of electrophysiological procedures. The study of cortical auditory evoked potentials (CAEP) allows for the analysis of the responses of electrically stimulated central auditory structures, and it does not depend on a child’s attention span and behavioural responses. For this reason, it is a reliable measure of an individual’s matu-rational process and cortical auditory functioning.
The P1 component of CAEP has been most utilized in re-search because it is considered a biomarker of the maturation of the auditory system structures. Individuals using cochlear implants for a longer time show lower latency for the P1 com-ponent(4-7). In addition, the development of the P1 component
follows the same pattern as that of a child with typical hearing, but with delays in the maturational process(5,8). However, recent
studies have shown that the P1 component has quick effects fol-lowing the activation of cochlear implants, reaching normality values between three and eight months from the beginning of the use of this device(7, 9-12).
The time span of auditory sensory deprivation inluences the process of central maturation(7,9,13,14). Children who receive
cochlear implants after the sensitive period can present ab-normal cortical auditory responses, even after many years of auditory stimulation(9,14,15).
Moreover, individuals with poorer speech perception present atypical records concerning these potentials(16-18), thus
relecting abnormal or immature patterns in cortical activity(16).
Therefore, by studying the maturational process of the audi-tory system, with a focus on CAEP in children who received cochlear implants, it is possible to obtain important informa-tion that can aid in understanding the differences in the speech perception development observed among users of cochlear implants, and, consequently, relect upon the process of refer-ring individuals to this implantation, especially with regard to a child’s age at the time of the procedure.
The aim of this study was to analyze the characteristics of the P1 component in children with prelingual hearing loss, who received cochlear implants, and correlate them with speech perception development.
METHODS
The present study was approved by USP’s Ethics Committee, as per report number 181/2004. The patients’ legal guardians signed the Informed Consent prior to the conduction of the examination.
Ten children participated in this study. They met the follow-ing criteria: age range between 1 and 5 years, and use of co-chlear implants with profound bilateral prelingual sensory neu-ral hearing loss. Children with neurological alterations and/or compromised auditory nerves attested by magnetic resonance imaging were excluded from this study.
Chart 1 presents the sample’s characteristics in relation to etiology, age at the time of activation, model of the internal component, speech processor, and signal processing strategy.
We assessed the children by investigating the CAEP in three stages: at the moment of cochlear implant activation, at three months, and at six months after the implantation, ac-cording to the methodology used in a previous study carried out in our laboratory(19).
The assessment of the CAEP was performed with the Smart EP USB programme, by Intelligent Hearing Systems. The audi-tory potentials were registered on channel A, and the ocular and blinking movements, on channel B.
Chart 1. Description of the sample with regard to etiology, age at activation, internal component model, processor, and signal processing strategy
Patient Etiology Age at activation Internal component model Speech processor Signal processing strategy
1 Cytomegalovirus 3 y 1 m SONATA Ti100 Opus 2 FS4
2 Idiopathic 2 y 3 m Hires 90k Harmony Hires-P w/Fidelity 120
3 Genetic 2 y 6 m Hires 90k Harmony Hires-P w/Fidelity 120
4 Consanguinity 1 y 2 m Hires 90k Harmony Hires-P w/Fidelity 120
5 Genetic 4 y 3 m Hires 90k Harmony Hires-P w/Fidelity 120
6 Idiopathic 2 y 1 m Hires 90k Harmony Hires-P w/Fidelity 120
7 Consanguinity 2 y 5 m Hires 90k Harmony Hires-P w/Fidelity 120
8 Idiopathic 1 y 10 m SONATA Ti100 Opus 2 FS4
9 Idiopathic 3 y 1 m SONATA Ti100 Opus 2 FS4
10 Idiopathic 1 y 6 m SONATA Ti100 Opus 2 FS4
In channel A, the active electrode was positioned in Cz connected to the (+) input of the pre-ampliier, and the refer-ence electrode was positioned in the mastoid contralateral to the cochlear implant, connected to the (-) input. The ground electrode was placed in Fpz, connected to the ground position. In channel B, the active electrode was placed in the supraorbital position, contralateral to the cochlear implant connected to the (+) input of the pre-ampliier, and the reference electrode was placed in the infraorbital position on the same side, connected to the (-) input. With the electrodes disposed in this manner, we monitored ocular movement and delimited the rejection level used in each examination.
In order to register ocular and auditory evoked potentials, we utilized ECG disposable electrodes of the brand Meditracetm 200, with Tem 20TM conductive paste for EEG, set in place after the individuals’ skin was cleaned with Nuprep abrasive gel for ECG/EEG. The impedance level was maintained between 1 and 3 kΩ for the electrodes.
The auditory responses were registered in response to a /da/ speech stimulus in an intensity of 70 dB NA, applied in a previ-ous study(20). The [da] stimulus was extracted from the second
syllable of the word [da’da], produced by a male young adult with luid voice quality and recorded by means of a unidi-rectional microphone with the free programme Praat (www. praat.org) directly onto the computer board at a sampling rate of 22 kHz. The bandwidths were collected from the stable region of the formant frequencies (F1, F2, and F3). With these
values, we compiled a script in the Praat (version 4.2.31), and the syllable was resynthesized. The duration of the [da] syl-lable corresponds to 180 ms. The linguistic stimulus produced, previously manipulated and recorded in a CD, was inserted in unit C of the computer connected to the software, Smart EP USB, by Intelligent Hearing Systems.
The procedure was conducted in free ield, with the acoustic box positioned at the child’s head level at a distance of 40 cm and azimuth 90°. We used a 30 W RMS power ampliier and a 50W RMS acoustic box on a tripod. An isolation transformer was installed in the ampliier’s passive signal input, with an impedance input of 440 Ω (impedance identical to that of the signal output of the earphones used in the Master Potential System) and output of 5 kΩ for the ampliier.
During the test, the children’s cochlear implants were functioning. The participants were comfortably seated in an armchair watching a video without any sound.
Upon observation of the presence of CEAP, the P1 compo-nent was identiied and analyzed according to its latency and amplitude. The registers were analyzed by two professionals with experience in electrophysiology; one of them was the researcher responsible for the procedure conduction. In the analysis, the second examiner had no access to any information concerning the children and the stages of assessment.
In order to verify the acquisition of the auditory abilities, we used the Infant-Toddler Meaningful Auditory Integration Scale, IT-MAIS(21). This scale consists of a 10-question structured
interview with the children’s parents or legal guardians focused on three areas of auditory development: (1) vocalization behav-iour; (2) sound alertness; and (3) attribution of meaning to the
sounds. For each question, there were ive choices, exempliied and scored as follows: Never (0), Rarely (1), Occasionally (2), Frequently (3), and Always (4), with a total score of 40 points converted into a percentage value.
The descriptive data analysis is presented through the aver-age, standard deviation, and minimum and maximum values. In the inferential analysis, we applied analysis of variance (ANOVA) and Tukey’s test, with the purpose of analyzing the correlation between the three stages of assessment and P1’s latency and amplitude. For the analysis of the results of the IT-MAIS, we used Wilcoxon’s and t-test. For the correlation of these indings with the latency and amplitude of the P1 component, we used Spearman’s and Pearson’s correlations.
The level of signiicance adopted was 5%.
RESULTS
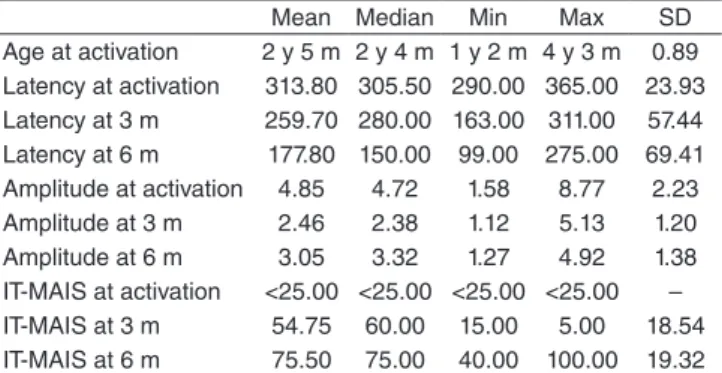
The descriptive analysis of the sample with regard to the children’s age at the moment of cochlear implant activation, latency and amplitude values of the P1 component, and the IT-MAIS score in the three stages of assessment is presented in Table 1.
Through the application of ANOVA, we found differ-ences in the latency (F=22,4; p=0,00) and amplitude (F=6,25; p=0,00) of the P1 component, according to the stage of assess-ment. Tukey’s test showed differences in P1’s latency values in the three assessment stages (Activation – three months; three – six months; Activation – six months). On amplitude, we observed differences in the component’s values in the following stages of assessment: Activation- 3 months; and Activation-six months (Table 2).
*Significant values (p≤0,05) – Tukey’s Test.
Table 2. Comparative statistical analysis of the component’s latency and amplitude at the three evaluation moments
3 months 6 months
Latency Activation 0,04* 0,00*
3 months – 0,00*
Amplitude Activation 0,00* 0,05*
3 months – 0,67
Table 1. Descriptive analysis of the sample with regards to the partici-pants’ age at cochlear implant activation, P1 latency (milliseconds), P1 amplitude (µV), and IT-MAIS score (%) in the three moments evaluated
Mean Median Min Max SD
Age at activation 2 y 5 m 2 y 4 m 1 y 2 m 4 y 3 m 0.89 Latency at activation 313.80 305.50 290.00 365.00 23.93 Latency at 3 m 259.70 280.00 163.00 311.00 57.44 Latency at 6 m 177.80 150.00 99.00 275.00 69.41 Amplitude at activation 4.85 4.72 1.58 8.77 2.23 Amplitude at 3 m 2.46 2.38 1.12 5.13 1.20 Amplitude at 6 m 3.05 3.32 1.27 4.92 1.38 IT-MAIS at activation <25.00 <25.00 <25.00 <25.00 – IT-MAIS at 3 m 54.75 60.00 15.00 5.00 18.54 IT-MAIS at 6 m 75.50 75.00 40.00 100.00 19.32
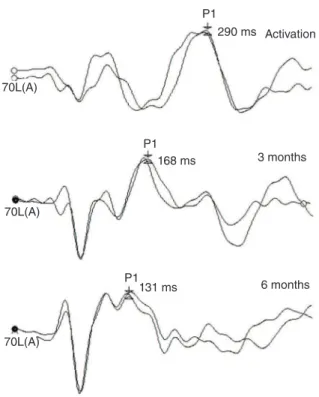
The P1 component of CAEP was identiied in all children in the three moments of assessment, with changes in morphol-ogy (Figure 1). The development of the P1 component in each individual is illustrated in Graph 1.
The IT-MAIS scores increased signiicantly with the time of use of the cochlear implant (Table 3), but there was no cor-relation with P1’s latency and amplitude in the three moments evaluated (Table 4).
3 months Activation
6 months 290 ms
168 ms
131 ms P1
P1 70L(A)
70L(A)
70L(A)
P1
Figure 1. Data obtained from investigating cortical auditory evoked potentials at the moment of activation of the cochlear implant, at three months and at six months after the procedure in a female patient who was 2 years and 6 months old at the time of activation
Patient 1 Patient 2 Patient 3 Patient 4 Patient 5 Patient 6 Patient 7 Patient 8 Patient 9 Patient 10 400
350
300
250
200
150
100
50
0
0 1 2 3
Age (years)
Lat
enc
y (ms)
4 5 6
Graph 1. Development of the P1 component for each individual at the three stages evaluated in comparison to minimum and maximum interval values of individuals with typical hearing
DISCUSSION
As the time of cochlear implant use lengthens, a de-crease in latency and amplitude of the P1 component is expected in children with prelingual sensory hearing loss(4-7, 9-12,15,22). Our findings corroborate those found in the
literature, given that the latency and amplitude decreased *Significant values (p≤0,05) – Wilcoxon’s Test (Activation – 3 months, and Activation – 6 months).
Table 3. Comparative statistical analysis of the IT-MAIS score at the three evaluation stages
IT-MAIS at 3 months IT-MAIS at 6 months
IT-MAIS at Activation 0.01* 0.01*
IT-MAIS at 3 months – 0.02*
Spearman’s Correlation (Act. 3 m and Act. 6 m), and Pearson’s Correlation (3–6m).
Caption: Lat. = Latency; Amp. = Amplitude; Act. = Activation; m = months Table 4. Statistical analysis of the correlation between the latency and amplitude of the P1 component and the IT-MAIS score at the three assessment stages
Lat. Act. 3 m
Lat. 3–6 m
Lat. Act. 6 m
Amp. At. 3 m
Amp. 3–6 m
significantly from one analyzed stage to the next (Table 2), which demonstrates the maturation of the auditory cortex through electric stimulation.
We observed immediate cortical response following the activation of the cochlear implants, as the P1 component was registered in all children. At this moment, the P1 component is characterized as a prominent positive peak that is gradually deined with the maturational process(4,13). This inding was
previously described in children with Auditory Neuropathy Spectrum Disorder, who used Hearing Aids (HA)(23).
A quick rate of P1 development following the activation of cochlear implants in children operated during the sensitive period, that is, up to three years and six months of age, has been described in literature. In these studies, the P1 component reached normal latency values between three and eight months after the implantation of the device(7,9,11,12). According to Graph
1, in the period of six months of cochlear implant use, the course of the maturational process of the auditory system occurred as expected, with the exception of patient 8, in whom there was no reduction in P1 latency in comparison to the second and third stages of the assessment. Upon further analysis of the patient’s history, we attested that the anatomic conditions found at the moment of surgery prevented cochlear implanta-tion in the ear determined initially. The doctors’ immediate conduct was to implant the device in the opposite ear, which later resulted in the lack of use of a HA in the ear contralateral to the cochlear implant.
In addition, three children presented P1 components with the expected latency for their chronological age despite the shorter time of auditory experience, which indicates quicker P1 development. Possibly, the stimulation of the cochlear implant during the sensitive period initiates an atypical and widespread pattern of activation of different cortical layers, resulting in a more rapidly decrease in latency than those found in children with typical hearing(12).
It is known that the time length of auditory sensory de-privation that precedes the activation of cochlear implants considerably inluences the redirecting of structures of central auditory pathways toward their primary function. This could explain the variability of the component P1’s latency and amplitude, and, consequently, the interference with speech perception. After the period considered sensitive, the beneits of cochlear implantation in relation to speech perception tend to diminish with the advancing of an individual’s age at the moment of activation(3,9).
In this study, only one child received the cochlear implant after this period (patient 5, at 4 years and 3 months of age). However, we veriied that the development of the P1 compo-nent was similar to that of patients 1, 3, 7, 9, and 10. It is also possible to attest differences in this developmental process, probably justiied by the fact that the activation of cochlear implants is not the only determining factor, but also the quantity and the quality of auditory stimulation(24). This fact has already
been reported in studies on the development of auditory abili-ties considered as prerequisites for oral language acquisition and development. In those studies, the time of device use and
aspects related to the family and auditory rehabilitation are shown to have an impact on the beneits obtained through cochlear implants(24-27).
Previous studies have described the correlation between the P1 component and an individual’s performance in tests of auditory abilities, characterizing this component as a predic-tor of the development of speech audipredic-tory perception(16-18,28,29).
In this study, there was signiicant improvement in the individuals’ auditory abilities with the use of cochlear implants, assessed through the IT-MAIS questionnaire (Table 3), but no signiicant correlation with the latency and amplitude of the P1 component (Table 4). This inding, which diverges from other studies in the literature, can be justiied by the fact that the children in the present study had a maximum time of device use of six months. Moreover, the auditory abilities assessed through this questionnaire, although considered as initial stages in the process of audi-tory functioning development, are completely acquired ap-proximately only after one year of device use, represented by a score of 80 to 100%(30).
The results of this study corroborate other indings in the literature in the sense that the redirecting of central structures by means of cochlear implant stimulation can be followed after the period of sensory deprivation through the investigation of CAEP, which proved to be a procedure that can be applied in clinical practice. These indings can contribute to the guidelines for cochlear implantantion referrals in infants, thus directing public policies concerning auditory deiciency treatment. In ad-dition, we reafirm that surgeries performed in the ideal period are not suficient to guarantee an individual’s good performance with the use of cochlear implants, as therapeutic intervention and continuous patient monitoring are also necessary.
CONCLUSION
The latency and amplitude of the P1 component decrease as the time of use of cochlear implants increase. However, there was no correlation between its development and speech perception performance.
ACKNOWLEDGEMENTS
We would like to thank CNPq (National Council for Scientiic and Technological Research) for the inancial aid granted for the conduction of this study, and Professor José Roberto Pereira Lauris for assisting us with the statistical analysis.
REFERENCES
1. Northern JL, Downs MP. Audição na infância. Trad. Paulo AFD, Azevedo MF. Rio de Janeiro: Guanabara Koogan; 2005.
2. Gordon KA, Wong DD, Valero J, Jewell SF, Yoo P, Papsin BC, et al. Use it or lose it? Lessons learned from the developing brains of children who are deaf and use cochlear implantsto hear. Brain Topogr. 2011;24(3-4):204-19. 3. Martínez-Beneyto P, Morant A, Pitarch MI, Latorre E, Platero A, Marco J. Paediatric cochlear implantation in the critical period of the auditory pathway, our experience. Acta Otorrinolaringol Esp. 2009;60(5):311-7. 4. Jiwani S, Papsin BC, Gordon KA. Central auditory development after
long-term cochlear implant use. Clin Neurophysiol. 2013; 124(9):1868-80. 5. Eggermont JJ, Ponton CW, Don M, Waring MD, Kwong B. Maturational
delays in cortical evoked potentials in cochlear implant users. Acta Otolaryngol. 1997;117(2):161-63.
6. Singh S, Liasis A, Rajput K, Towell A, Luxon L. Event-related potentials in pediatric cochlear implant patients. Ear Hear. 2004;25(6):598-610. 7. Sharma A, Dorman MF, Kral A. The inluence of a sensitive period on
central auditory development in children with unilateral and bilateral cochlear implants. Hear Res. 2005;203(1-2):134-43.
8. Ponton CW, Don M, Eggermont JJ, Waring MD, Kwong B, Masuda A. Auditory system plasticity in children after long periods of complete deafness. Neuroreport. 1996;8(1):61-5.
9. Sharma A, Dorman MF, Spahr AJ. A sensitive period for the development of the central auditory system in children with cochlear implants: implications for age of implantation. Ear Hear. 2002;23(6);532-9. 10. Sharma A, Tobey E, Dorman M, Bharadwaj S, Martin K, Gilley
P, et al. Central auditory maturation and babbling development in infants with cochlear implants. Arch Otolaryngol Head Neck Surg. 2004;130(5):511-6.
11. Dorman MF, Sharma A, Gilley P, Martin K, Roland P. Central auditory development: evidence from CAEP measurements in children it with cochlear implants. J Commun Disord. 2007;40(4):284-94.
12. Sharma A, Dorman MF, Spahr AJ. Rapid development of cortical auditory evoked potentials after early cochlear implantation. Neuroreport. 2002;13(10):1365-8.
13. Ponton CW, Eggermont JJ. Of kittens and kids: altered cortical maturation following profound deafness and cochlear implant use. Audiol Neurootol. 2001;6(6):363-80.
14. Sharma A, Dorman MF. Central auditory development in children with cochlear implants: clinical implications. Adv Otorhinolaryngol. 2006;64:66-88.
15. Sharma A, Dorman M, Spahr A, Todd NW. Early cochlear implantation in children allows normal development of central auditory pathways. Ann Otol Rhinol Laryngol Suppl. 2002;189:38-41.
16. Gordon KA, Tanaka S, Papsin BC. Atypical cortical responses underlie poor speech perception in children using cochlear implants. Neuroreport. 2005;16(18):2041-5.
17. Gordon KA, Tanaka S, Wong DDE, Papsin BC. Characterizing responses from auditory cortex in young people with several years of cochlear implant experience clinical. Neurophysiology. 2008;119:2347-62. 18. Kurnaz M, Satar B, Yetiser S. Evaluation of cochlear implant users’
performance using middle and late latency responses. Eur Arch Otorhinolaryngol. 2009;266(3):343-50.
19. Ventura LMP, Costa Filho OA, Alvarenga KF. Maturação do sistema auditivo central em crianças ouvintes normais. Pró-Fono. 2009;21(2):101-6.
20. Banhara MR. Potenciais auditivos de longa latência: N1, P2, N2, e P300, evocados por estímulo de fala em usuários de implante coclear [Dissertação]. São Paulo: Universidade de São Paulo; 2007.
21. Castiquini EAT, Bevilacqua MC. Escala de Integração Auditiva Signiicativa: procedimento adaptado para a avaliação da percepção da fala. R Soc Bras Fonoaudiol. 2000;4(6):51-60.
22. Sharma A, Martin K, Roland P, Bauer P, Sweeney MH, Gilley P, et al. P1 latency as a biomarker for central auditory development in children with hearing impairment. J Am Acad Audiol. 2005;16(8):564-73.
23. Sharma A, Cardon G, Henion K, Roland P. Cortical maturation and behavioral outcomes in children with auditory neuropathy spectrum disorder. Int J Audiol. 2011;50(2):98-106.
24. Flexer C. Cochlear implants and neuroplasticity: linking auditory exposure and practice. Cochlear Implants Int. 2011;12(Suppl 1):S19-21. 25. Geers A, Brenner C, Nicholas J, Uchanski R, Tye-Murray N, Tobey E.
Rehabilitation factors contributing to implant beneit in children. Ann Otol Rhinol Laryngol Suppl. 2002;189:127-30.
26. Moret AL, Bevilacqua MC, Costa OA. Cochlear implant: hearing and language in pre-lingual deaf children. Pro Fono. 2007;19(3):295-304. 27. Davidson LS, Geers AE, Blamey PJ, Tobey EA, Brenner CA. Factors
contributing to speech perception scores in long-term pediatric cochlear implant users. Ear Hear. 2011;32(1):19S-26S.
28. Cardon G, Sharma A. Central auditory maturation and behavioral outcome in children with auditory neuropathy spectrum disorder who use cochlear implants. Int J Audiol. 2013;52(9):577-86.
29. Alvarenga KF, Amorim RB, Agostinho-Pesse RS, Costa OA, Nascimento LT, Bevilacqua MC. Speech perception and cortical auditory evoked potentials in cochlear implant users with auditory neuropathy spectrum disorders. Int J Pediatr Otorhinolaryngol. 2012;76(9):1332-8.