Arq Neu ro p siq u iat r 2003;61(4):906-908
BRAINSTEM AUDITORY EVOKED RESPONSE
IN NORM AL TERM NEONATES
Laura M . F. F. Guilhot o
1, Virgínia S. Quint al
2, M aria T. Z. da Cost a
2ABSTRACT - Brainstem aud itory evoked resp onse (BAER) is a reliab le test for neonatal aud itory and neurological d ysfunction and it p erm its early d iag nosis and rehab ilitation. The p urp ose of this stud y is to d em onstrate latencies of BAER in norm al term neonates in ord er to ob tain reference values in a university hosp ital. BAER w as p erform ed in the second d ay of life in 47 norm al new b orns (25 m ale, 22 fem ale) w hich g estational ag es w ere hig her than 37 and low er than or eq ual to 40 w eeks that d id not p resent fam ilial history of d eafness. The exam w as p erform ed w ith 80 d BHL alternating p olarity 10/sec clicks p resented m onaurally. Tw o thousand stim ulus trials w ere averag ed and d up licated for each ear. Mean w ave latencies in m sec w as: I, 1.79 (SD 0.20); II, 2.88 (SD 0.28); III, 4.54 (SD 0.31); IV, 5.86 (SD 0.36); V, 6.75 (SD 0.38); inter-p eak latencies (IPL) I-III, 2.75 (SD 0.36); IPL III-V, 2.22 (SD 0.22); and IPL I-V, 4.97 (SD 0.43).
KEY WORDS: new b orn, evoked resp onses, b rainstem , norm ative values.
Potencial evocado auditivo de tronco cerebral em recém-nascidos normais a termo
RESUMO - O estud o d o p otencial evocad o aud itivo d e tronco cereb ral (PEA-TC) é um teste d iag nóstico útil d e d isfunção aud itiva e neurológ ica neonatal p erm itind o reab ilitação p recoce. O ob jetivo d este estud o é ob ter d ad os norm ativos d as latências d o PEA-TC em recém -nascid os norm ais a term o em hosp ital universitário. PEA-TC foi reg istrad o no seg und o d ia d e vid a em 47 recém -nascid os norm ais (22 fem ininos e 25 m asculinos) co m id a d es g est a cio n a is su p erio res a 37 e in ferio res o u ig u a is a 40 sem a n a s, q u e n ã o a p resen t a ssem anteced entes fam iliares d e d éficit aud itivo. O tem p o d e latência d e 2.000 estím ulos p rom ed iad os e um a rep licação foram estud ad os p ara cad a ouvid o, utilizand o-se clicks m onoaurais alternantes d e 80 d BHL a 10/s. A m éd ia em m iliseg und os d a latência d as ond as foi: I, 1,79 (DP 0,20); II, 2,88 (DP 0,28); III, 4,54 (DP 0,31); IV, 5,86 (DP 0,36); V, 6,75 (DP 0,38); latências interp ico (LIP) III, 2,75 (DP 0,36); LIP IIV, 2,22 (DP 0,22); e LIP I-V, 4,97 (SD 0,43).
PALAVRAS-CHAVE: recém -nascid o, p otencial evocad o, tronco encefálico, norm atização
Set o r d e Neu ro fisio lo g ia Clín ica d a Divisão d e Clín ica Méd ica1 e Un id ad e Neo n at al d a Divisão d e Clín ica Ped iát rica2 d o Ho sp it al Un
iversi-t ário d a Un iversid ad e d e São Pau lo (HU-USP), São Pau lo SP, Brasil.
Received 31 March 2003, received in fin al fo rm 11 Ju ly 2003. Accep t ed 5 Au g u st 2003.
Dra. Laura M . F. Ferreira Guilhot o - Set or de Neurof isiologia Clínica da Divisão de Clínica M édica do HU-USP - Avenida Lineu Prest es 2565 - 05508-900 São Paulo SP - Brazil. E-mail: [email protected]
Brainstem auditory evoked response (BAER) reflects non-p rop ag ated , volum e-cond ucted events, w hich m anifest the sequential activation of auditory brains-tem nuclei and pathways1,2. A series of 5-7 waves can
be recorded and are related to the following regions of auditory pathway: wave I, segm ent of the eighth nerve close to the cochlea; wave II, intracranial por-tion of the eighth nerve close to the brainstem and cochlear nucleus in p ons; wave III, sup erior olivary com plex (pons); wave IV, m id and upper pons; wave V, lateral lem niscus (upper pons) or inferior colliculus (low m idbrain)3. It has been observed a progressive
decline in the latency of wave V and interpeak latency I-V from neonatal p eriod to around infancy4-6 and
childhood until achieving adult values. These evoked
responses though, m ay indicate som e physiological dysfunction in the auditory system up to the brainstem level. Since clinical sem iology is poor in neonates, this type of non-invasive tests m ay objectively evaluate the integrity of this pathway, as well the surrounding areas in the brainstem . It turns out to be a reliable test for auditory and neurological dysfunction at this age and it perm its early diagnosis and rehabilitation.
There are few rep orts of norm ative values of BAER in n eo n at al p erio d , esp ecially in d evelo p m en t n a-t io n s7-8. Th ere is a n eed t o h ave referen ce g u id es fo r
lab o rat o ries in every co u n t ry t o est ab lish a st an d ard ro u t in e o f in vest ig at io n .
Arq Neu ro p siq u iat r 2003;61(4-A) 907
t o o b t ain n o rm at ive d at a in a u n iversit y h o sp it al o f São Pau lo , Brazil, a cit y w it h 20 m illio n h ab it an t s.
M ETHOD
BAER w as p erfo rm ed b et w een 48 an d 96 h o u rs o f life in 47 n o rm al n ew b o rn s in t h e Un iversit y Ho sp it al o f t h e Un iversit y o f São Pau lo . No rm al n ew b o rn s (25 m ale, 22 fem ale) w ere evalu at ed , w it h ad eq u at e w eig h t fo r g est a-t io n al ag e (GA), w h ich w ere h ig h er a-t h an 37 an d lo w er t h an o r eq u al t o 40 w eeks (Du b o w it z). Th e p at ien t s p re-sented no fam ilial history (parents and siblings) of deafness and had fifth m inute Ap gar scores higher than 7 and nega-t ive ellu anega-t e an d Co o m b s reacnega-t io n s. Th e p anega-t ien nega-t s d id n o nega-t p resen t ed an y n eo n at al d ist ress w it h excep t io n o f m ild p h ysio lo g ical jau n d ice w it h o u t n eed o f p h o t o t h erap y.
Th e exam w as p erfo rm ed d u rin g sleep , aft er feed in g s in the m orning , using 80 d BHL clicks of alternating p olarity p resen t ed m o n au rally at a rat e o f 10/sec. A t o t al o f 2000 st im u lu s t rials w as averag ed an d d u p licat ed fo r each ear (an alysis t im e 10m sec, filt ers 100-3.000Hz).
RESULTS
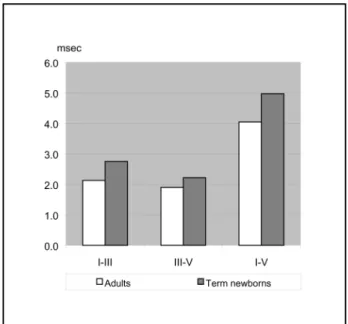
Th e m ean lat en cy t im e o f w aves I, II, III, IV, V an d t h e in t er-p ea k la t en cies (IPL) w ere m ea su red . Th e m ean o f t h e lat en cies in m illiseco n d s w as t h e fo llo -w in g : -w ave I, 1.79 (SD 0.20); -w ave II, 2.88 (SD 0.28); w ave III, 4.54 (SD 0.31); w ave IV, 5.86 (SD 0.36); w ave V, 6.75 (SD 0.38); IPL, I-III, 2.75 (SD 0.36); III-V, 2.22 (SD 0.22); an d fin ally I-V, 4.97 (SD 0.43).
When we com pare the results of the present study w ith th e valu es o b tain ed in h ealth y ad u lts w ith sim i-lar m et h o d o lo g y in o u r lab o rat o ry, w e o b served a clear d ecrease in lat en cy valu es in t h ese lat t er. Th e g reat est d iscrep an cy w as w ave V lat en cy, as w ell as in t er-p eak lat en cies, sh o w ed in Fig u res 1 an d 2, res-p ect ively.
DISCUSSION
Our results w ere sim ilar to other authors that stu-d iestu-d BAERs in n eo n at es9.
Severa l st u d ies9-12 o b served t h a t h ea rin g t h
re-sh o ld s (w ave V) o f n ew b o rn in fan t s d im in ire-sh w it h in creasin g ag e. In st ead , w ave I d o es n o t seem t o have the sam e velocity of decrease trough adult levels esp ecially w h en d ifferen t st im u lu s rat es are u sed13.
This fact probably reflects that m aturation of auditory p at h w ays m ay in vo lve d ifferen t m ech an ism s in cen -t ral an d p erip h eral areas14. St arr et al.15 h ave su g
-g est ed t h at p erip h eral ch an -g es m an ifest ed b y d e-crease o f w ave I lat en cy co u ld in clu d e im p ed an ce ch an g es in t h e m id d le ear, t h e m at u rat io n o f h ig h -freq u en cy sen sit ivit y o f t h e co ch lea o r ch an g es in t ran sd u ct io n b et w een h air cells an d t h e d en d rit es o f VIII n erve.
Central conduction could involve changes in nerve cond uction velocity associated with m yelination and / or chang es in synap tic efficiency at the various nuclei of the auditory pathway16. Maturation of hum an
cen-t ral au d icen-t o ry syscen-t em excen-t en d s in cen-t o ad o lescen ce, an d cert ain au d it o ry p ro cessin g skills su ch sp eech reco g -n it io -n h ave a p ro lo -n g ed t im e co u rse17.
BAER in neonates m ay b e ab norm al in cong enital d eafn ess, an o xia, cen t ral n ervo u s syst em in fect io n , t o xic st at es su ch as d u rin g an t ib io t ics t reat m en t , ja-u n d ice, in t rin sic b rain st em lesio n , sja-u ch as t ja-u m o rs, vascular p athologies (infarctions, hem orrhages, m al-fo rm at io n s) an d co m a3,18.
Beverly et al.19 fo u n d t h at BAER w ere n o t a g o o d
p ro g n o st ic in d icat o r o f fu t u re n eu ro d evelo p m en t al d isab ility or outcom e in neonatal p eriod . Salam y and
Fig 1. Normal new born and adult BAER mean lat ency values in our laborat ory.
908 Arq Neu ro p siq u iat r 2003;61(4-A)
Eld red g e20 h ave d em o n st rat ed a h ig h er risk o f BAER
ab n o rm alit ies in t h e n u rsery in n o rm al h earin g in -fan t s t h at h ad n eu ro lo g ical sig n s o r b rain an o m alies an d t h o se exp o sed t o co cain e in u t ero .
CONCLUSION
No rm a t ive BAER s t u d ie s in t e rm n e o n a t e s p erfo rm ed in u n iversit y h o sp it als are n ecessary t o est ab lish referen ce valu es fo r evalu at io n o f au d it o ry an d n eu ro lo g ic p ro g n o st ic fact o rs as w ell as t o early d iag n o se ch ild ren w it h risk o f au d it o ry d ysfu n ct io n .
Acknow ledgments - The authors wish to acknowledge the helpful suggestions of Dr. Francisco J. C. Luccas, director o f t h e Neu ro p h ysio lo g y Sect io n o f Alb ert Ein st ein Ho sp i-tal, São Paulo, Brazil, as well the coop eration of technicians Elian e A. Ab reu an d Elian e Orn elas w it h t h e st u d y.
REFERENCES
1. Jew ett DL, Ro mano MN, W illisto n JS. Human aud ito ry evo ked potentials: possible brain stem components detected on the scalp. Science 1970;167:1517-1518.
2. Picton TW, Hillyard SA, Krausz HI, Galambos R. Human auditory evoked potentials: I. Evaluation of components. Eletroencephalograph Clin Neurophysiol 1974;36:179-190.
3. Chiappa KH. Brain stem auditory evoked potentials: interpretation. In Chiappa KH (ed). Evoked potentials in clinical medicine. New York: Raven Press, 1995:223-305.
4. Golstein PJ, Krumholz A, Felix JK, Shannon D, Carr RF. Brain stem-evoked response in neonates. Am J Obst Gynecol 1979;135:622-639. 5. Hecox K, Galambos R. Brain stem auditory evoked responses in human
infants and adults. Arch Otolaryngol 1974;99:30-33.
6. Salamy A, McKean CM, Buda FB. Maturation of contralateral brain-stem responses in preterm infants. Brain Res 1975;96:361-366. 7. Deorari AK, Garg R, Bisht MS, Ahuja GK, Paul VK, Singh M. Auditory
brain stem evoked response in normal neonates and infants. Indian Pediatr 1989;26:981-986.
8. Jiang Z D, Z hang L, Wu YY, Liu XY. Brainstem audito ry evo ked responses from birth to adulthood: development of wave amplitude. Hear Res 1993;68:35-41.
9. Gorga MP, Reiland JK, Beauchaine KA, Worthington DW, Jesteadt W. Auditory brainstem responses from graduates of an intensive care nursery: normal patterns of response. J Speech Hear Res 1987;30:311-318. 10. Despland PA, Galambos R. Use of the auditory brainstem responses
by prematures and newborns infants. Neuropädiatrie 1979;11:99-107. 11. Lary S, Briassoulis G, Vries L, Dubow itz L, Dubow itz V. Hearing threshold in preterm and term infants by auditory brainstem response. J Pediatr 1985;107:593-599.
12. Mo rgo n A , Salle B. A stud y o f brain stem evo ked respo nses in prematures. Acta Otolaryngol 1980;89:370-375.
13. Lina-Granade G, Collet L, Morgon A, Salle B. Maturation and effect of stimulus rate on brainstem auditory evoked potentials. Brain Develop 1993;4:263-269.
14. Salamy A, McKean CM. Postnatal development of human brainstem potentials during the first year of life. Electroenceph, Clin Neurophysiol 1976;40:418-426.
15. Starr A, Amille RN, Martin WH, Sanders S. Development of auditory function in newborn infants revealed by auditory brainstem potentials. Pediatrics 1977;60:831-839.
16. Ken-Dror A, Pratt H, Zeltzer M, Sujov P, Katzir J, Benderley A. Auditory brain-stem evoked potentials to clicks at different presentation rates: estimating maturation of pre-term and full-term neonates. Electroen-ceph Clin Neurophysiol 1987;68:209-218.
17. Ponton CW, Eggermont JJ, Kwong B, Don M. Maturarion of human central auditory system activity: evidence from multi-channel evoked potentials. Clin Neurophysiol 1999;111:220-236.
18. Hecox KE, Cone BC. Prognostic importance of brainstem auditory evoked responses after asphyxia. Neurology 1981;31:1429-1433. 19. Beverley DW, Smith IS, Beesley P, Jones J, Rhodes N. Relationship of
cranial ultrasonography, visual and auditory evoked responses with neurodevelopmental outcome. Dev Med Child Neurol 1990;32:210-222. 20. Salamy A , Eldredge L. Risk for A BR abnormalities in the nursery.