www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Acoustic
analysis
of
oropharyngeal
swallowing
using
Sonar
Doppler
夽
,
夽夽
Franciele
Savaris
Soria
a,∗,
Roberta
Gonc
¸alves
da
Silva
b,
Ana
Maria
Furkim
caFaculdadeAssisGurgacz,Cascavel,PR,Brazil
bUniversidadeEstadualdeSãoPaulo(UNESP),SãoPaulo,SP,Brazil cUniversidadeFederaldeSantaCatarina(UFSC),Florianópolis,SC,Brazil
Received25March2014;accepted27February2015 Availableonline17December2015
KEYWORDS
Deglutition; Elderly; Evaluation
Abstract
Introduction:Duringtheagingprocess,oneofthefunctionsthatchangesisswallowing.These alterations inoropharyngeal swallowingmay be diagnosedby methods that allow boththe diagnosisandbiofeedbackmonitoringbythepatient.Oneofthemethodsrecentlydescribed intheliteraturefortheevaluationofswallowingistheSonarDoppler.
Objective: Tocomparetheacousticparametersoforopharyngealswallowingbetweendifferent agegroups.
Methods:Thiswasafield,quantitative,study.ExaminationwithSonarDopplerwasperformed in75elderlyand72non-elderlyadultsubjects.Thefollowingacousticparameterswere estab-lished: initialfrequency, first peakfrequency,second peakfrequency;initial intensity,final intensity;andtimefortheswallowingofsaliva,liquid,nectar,honey,andpudding,with5-and 10-mLfreedrinks.
Results:Objective,measurabledatawereobtained;mostacousticparametersstudiedbetween adultandelderlygroupswithrespecttoconsistencyandvolumeweresignificant.
Conclusion: Whencomparingelderlywithnon-elderlyadultsubjects,thereisamodificationof theacousticpatternofswallowing,regardingbothconsistencyandfoodbolusvolume. © 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:SoriaFS,daSilvaRG,FurkimAM.AcousticanalysisoforopharyngealswallowingusingSonarDoppler.BrazJ
Otorhinolaryngol.2016;82:39---46.
夽夽Institution:FaculdadeAssisGurgacz,Cascavel,PR,Brazil.
∗Correspondingauthor.
E-mail:[email protected](F.S.Soria). http://dx.doi.org/10.1016/j.bjorl.2015.12.001
PALAVRAS-CHAVE
Deglutic¸ão; Idoso; Avaliac¸ão
Análiseacústicadadeglutic¸ãoorofaríngeautilizandoSonarDoppler
Resumo
Introduc¸ão:Duranteoprocessodeenvelhecimento,umadasfunc¸õesquesofremodificac¸ãoé adeglutic¸ão.Estasalterac¸õesnadeglutic¸ãoorofaríngeapodemserdiagnosticadaspormétodos quepermitemtantoodiagnósticoquantoomonitoramentoebiofeedbackaoindivíduo.Umdos métodosdescritonaliteraturarecentementeparaaavaliac¸ãodadeglutic¸ãoéoSonarDoppler.
Objetivo:Oobjetivo desse estudofoicomparar osparâmetrosacústicos dadeglutic¸ão oro-faríngeaentrefaixasetáriasdistintas.
Método: Estudodecampo, quantitativo. Oexame comoSonar Doppler foiaplicado em 75 idosose72adultos.Estabeleceram-seosparâmetrosacústicos:frequênciainicial,frequência doprimeiropico,frequênciadosegundopico,intensidadeinicial,intensidadefinaletempo, paraasdeglutic¸õesdesaliva,liquido,néctar,melepudim,comgolelivre,5mLe10mL.
Resultados: Obtiveram-sedados objetivos emensuráveis, apresentandosignificânciapara a maioriadosparâmetrosacústicosestudadosentreogrupodeidososeadultos emrelac¸ãoà consistênciaevolume.
Conclusão:Verificamosquehámodificac¸ãodopadrãoacústicodadeglutic¸ão,tantoemrelac¸ão àconsistênciaquanto avolume dobolo alimentar,quandocomparados adultosidososenão idosos.
©2015Associac¸ãoBrasileira deOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicadopor ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Theworld’selderlypopulationisincreasingconsiderably;in 2025,itwillexceedthenumberofchildren.Therefore,such individualsdeservetheattentionofinterdisciplinary health-care teams; these professionals need toacquire a better understanding of theaging process andits impactonthe individual’shealth,aimingmainlyat improvingthequality oflifeofthispopulation,aswellasproposingmeasuresto preventpossibleclinicalcomplications.1,2
During the aging process, one of the functions that changesisswallowing.Swallowingdisordersassociatedwith aging can be conceptualized as presbyphagia.3 However,
swallowing disturbances caused by neurological and/or structuraldiseasesarecalled dysphagia;boththese disor-dersandpresbyphagiamayresultinchangesoftheclinical condition of the patient,4,5 possibly with changes in the
oral,pharyngeal, andesophagealphasesofswallowing.In theoralandpharyngeal phasesanincrease inthetimeof bolustransmissionoccurs,andthesameisobservedinthe esophagealphase,whichisassociatedwithahighfrequency ofnon-propulsivecontractions.6,7
These changes in oropharyngeal swallowing may be diagnosed by methods that allow for both diagnosis and biofeedbackmonitoring, andthus aidintreatment. These methods include video fluoroscopy, nasal endoscopy, and cervicalauscultation.8,9
Anothermethodrecentlydescribedintheliteraturefor theevaluationofswallowingistheSonarDoppler,whichmay becomeavaluabletestfor assessingswallowing,asitisa painless, noninvasive,and inexpensive test that does not exposethepatienttoradiation.10---12
This study aimed to compare the acoustic parame-ters of oropharyngeal swallowing between different age groups.
Methods
This research was conducted in two stages. In the first step,aquestionnaire(RiskScreeningProtocolfor Swallow-ing) that contained questions related to risk factors for dysphagia wasadministered(Appendix1).Volunteerswho presented risk factors for dysphagia were excluded (with neurological disease, head and neck structural changes, expositiontoradiotherapyand/orchemotherapy,andthose with swallowing complaints). In total, 189 questionnaires wereadministered;147individualswereselectedand par-ticipated in the second stage of the research, and were divided into two groups. Group I (GI) consisted of 75 healthyelderlypeople,aged>60years,withameanageof 71 years.GroupII (GII) consisted of72 healthyadult sub-jectsaged between18 and 59years, withamean age of 42years.
In the second phase, the participants were submitted tothe evaluation of oropharyngealswallowingwithSonar Doppler. The assessment followed the protocol proposed bySantosandMacedo-Filho,10 withmodificationsregarding
specifications of consistency. The protocol classifies the swallowing of saliva, liquids, and pastes. In the present study, the classification of the National Dysphagia Diet Guidelines(2002)13proposingliquid,nectar,honey,and
pud-dingwasused,withtheadditionofsalivaswallows(Fig.1). All study subjects received the same food consistency during theprocedure, dividedintodry swallowing(saliva) andliquid,nectar,honey,andpuddingswallowing,using vol-umes in the sequence described: 5mL-, 10mL-, and free swallows. In the sequence described, four swallows were required:firstly,salivaswallowing,followedbyfree-,5 mL-and10mL-swallowsofeachconsistency.
TheconsistencieswerepreparedwiththeNutillis®
Figure1 Classificationofconsistencies---NationalDysphagiaDietGuidelines(2002).
gums,manufacturedbySupport®)andofferedimmediately
afterpreparation,accordingtotherecommendationsofthe NationalDysphagiaDietGuidelines.13
In theprocessofcapturing swallowingsounds bySonar Doppler,the subjecttestedremainedin a seatedposition andwithafreeneck.Thetransducerwasplacedinthe lat-eralregionofthetracheaimmediatelybelowthecricoidon therightside,andthetransducerbeamwaspositionedto formanangleof30---6014(Fig.2).
The equipmentusedwasaportableultrasonic detector (DF-4001model; Martec;Fig.3).A single-crystal,flat disk transducerprovidedtheDopplerinterface(Fig.4).Contact gel was usedon the transducer tofacilitate skin contact (Fig.3).Ultrasoundfrequency(byDopplereffect)wasset at 2.5MHz;output,10mW/cm2;soundoutput power,1W.
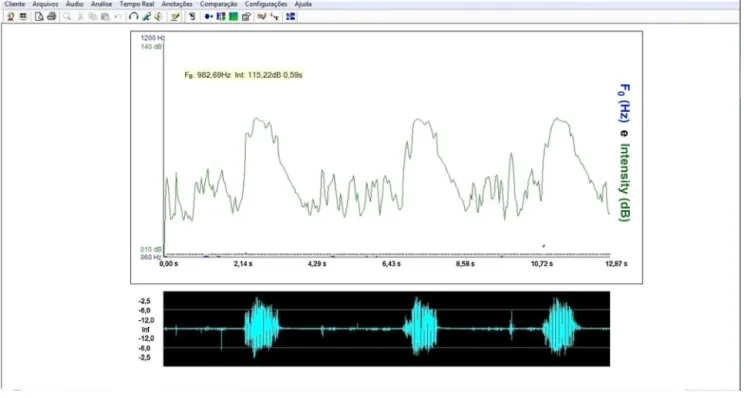
Theequipmentwasconnectedtoacomputer(Fig.3). For the acoustic analysis of the sound signal captured bythesonar,theVoxMetriasoftware(Fig.4)wasused.To capturesoundsignalsbythecontinuousDopplerequipment, themachine’svolumewasadjustedtoNo.3.Theintensity valueswereanalyzedwithalowerlimit=10dBandanupper limit=140dB.
The acoustic parameters studied followed the same parametersproposedbySantosandMacedo-Filho,10namely:
Figure2 Transducerplacementpositioninthepatient.
Initial frequency(IF)of soundsignal:definedasthefirst tracing of the sound wave, representing the onset of swallowing15;
Frequencyofthefirstpeak(F1P):definedasthefirstpeak observed onthesoundwave ofswallowing,representing laryngealelevation15;
Frequency of thesecond peak(F2P):defined asthe sec-ond peakofthe soundwave ofswallowing,representing cricopharyngealopening15;
Initialintensity (II):definedastheinitialintensityofthe acousticplottedlinerecordedbyDopplerduringthe begin-ningoftheswallowingevent.15 Theintensityvalueswere
analyzedwithalowerlimitof10dBandanupperlimitof 140dB.
Finalintensity(FI):definedastheendofthesecondwave peak recorded by Doppler during the swallowing event, obtainingtheamplitudeoftheaudiosignal.Itistheweak signal, associated with the descent of the larynx after swallowing.15 The intensity values were analyzed witha
lowerlimitof10dBandanupperlimitof140dB.
Acoustic time (T):defined asthe time intervalbetween thepointofapneaofdeglutition(FI)16topost-swallowing
glottalexpiratoryrelease(Fig.5).
Thestatisticalmethodsusedinthestudywerethe infer-ential technique and significance test. To analyze the significance of data obtained from acoustic parameters betweenelderlyandadultgroups ineach consistencyand in each volume, Student’s t-test--- equal variance of two
Figure4 Flatdisktransducer.
samples was used, and the significance level was set at 0.05.Inthestatisticalanalysis,acrossoverbetweenelderly (GI)andadult(GII)groups wascarriedout,comparingthe parametersproposedinthemethod.
ThisstudywasapprovedbytheResearchEthics Commit-tee,underNo.00061/2008.
Results
There was no statistically significant difference between groups in the analysisof theinitial and final frequencies, eitherforthedifferentconsistenciesusedorthedifferent volumes(Tables1and2).Asignificantdifferencebetween
Table1 Comparisonbetweenelderly(GI)andadult (GII) groupsforinitialfrequency(IF).
Consistency Elderly group
Adult group
p-value
Dry 350.6Hz 578.2Hz 0.0000a
Liquid---DL 404.8Hz 567.4Hz 0.0000a
Liquid--- 5mL 556.8Hz 571.5Hz 0.19610 Liquid--- 10mL 473.1Hz 684.4Hz 0.0000a
Nectar--- DL 406.4Hz 616.7Hz 0.0000a
Nectar---5mL 566.1Hz 404.5 0.0000a
Nectar---10mL 489.7Hz 471.9Hz 0.1034 Honey---DL 416.4Hz 603.0Hz 0.0000a
Honey---5mL 560.1Hz 587.9Hz 0.0093a
Honey---10mL 429.1Hz 384.1Hz 0.0020a
Pudding---DL 412.8Hz 333.0Hz 0.0000a
Pudding---5mL 569.7Hz 555.3Hz 0.1097 Pudding---10mL 433.7Hz 342.3Hz 0.0000a
Student’st-test.
a Significantdifferencesatthe0.05significancelevel.
thegroupsanalyzedwasdetectedinallparametersofthe firstandsecondpeaksforthedifferentconsistencies,with fewexceptions(Tables3and4).
In most of the comparisons carried out on the ini-tial and final intensities, statistical significance among groupsandconsistencieswasobserved(Tables4and5).All comparisons were statistically significant for the time parameter(Table6).
Discussion
Becauseitisrelativelylowcost,theDopplerSonarcompares favorably with other tests, such as nasolaryngofibroscopy andvideofluoroscopy.Moreover,itisnotinvasive,doesnot requiresedation,ispainless,anddoesnotexposepatients toradiation.
Inthepresentstudy,specificcharacteristicsofthesound curvesevaluatedwithSonarDopplershowedthatthereare
Table2 Comparison between the elderly(GI) andadult (GII)groupsforfrequencyoffirstpeak(F1P).
Consistency Elderly group
Adult group
p-value
Dry 661.9Hz 509.1Hz 0.0001a
Liquid---DL 831.4Hz 916Hz 0.0000a
Liquid---5mL 832.3Hz 887.8Hz 0.0000a
Liquid---10mL 793.6Hz 1010.9Hz 0.0000a
Nectar---DL 779.8Hz 833.8Hz 0.0000a
Nectar---5mL 810.7Hz 799.0Hz 0.2416 Nectar---10mL 990.1Hz 1050.2Hz 0.0001a
Honey---DL 800.6Hz 897.1Hz 0.0000a
Honey---5mL 813.7Hz 819.5Hz 0.4761 Honey---10mL 890.0Hz 354.5Hz 0.0000a
Pudding---DL 791.8Hz 802.9Hz 0.4634 Pudding---5mL 828.2Hz 743.5Hz 0.0000a
Pudding---10mL 886.0Hz 891.2Hz 0.6159
Student’st-test.
a Significantdifferencesatthe0.05significancelevel.
Table 3 Comparison between theelderly(GI) and adult (GII)groupsforfrequencyofsecondpeak(F2P).
Consistency Elderly group
Adult group
p-value
Dry 870.1Hz 1005.5Hz 0.0000a
Liquid---DL 1054.9Hz 1043.9Hz 0.0697 Liquid---5mL 967.8Hz 1041.7Hz 0.0000a
Liquid---10mL 977.9Hz 1078.4Hz 0.0000a
Nectar--- DL 1042.3Hz 967.2Hz 0.0000a
Nectar--- 5mL 980.9Hz 978.6Hz 0.7994 Nectar--- 10mL 1155.4Hz 1102.8Hz 0.0000a
Honey---DL 1045.6Hz 1062.0Hz 0.0050a
Honey---5mL 974.6Hz 966.7Hz 0.2646 Honey---10mL 1087.5Hz 1045.0Hz 0.0000a
Pudding---DL 1046.0Hz 1032Hz 0.0191a
Pudding--- 5mL 976.3Hz 950.7Hz 0.0000a
Pudding--- 10mL 1029.4Hz 1038.4Hz 0.0260a
Student’st-test.
a Significantdifferencesatthe0.05significancelevel.
significantdifferencesintheswallowingpatternsofhealthy elderlysubjectscomparedtohealthynon-elderlyadults.
But it was not possible to compare the present data with that from other studies, because of the originality of this research. However, this study opens a reference databaseforfutureresearch,andprovidesnormalacoustic parametersforsoundwaves during swallowingintwo dif-ferentagegroups.
Intheelderlypopulation,somechangeswereobserved during swallowing. The elderly often have reduced func-tional reserves of various organs and systems, and this includeschangesinthephases ofdeglutition.Whenthese individualsarefreeof healthproblems, theymake useof compensatorystrategies, suchastheuse of strength dur-ingswallowingandincreasedtonguepressureintotheoral cavity,attemptingtoassistthepropulsionoffood.17---19
In agreement with the literature, this study identified ahigherincidenceof decreasedstrength, increasedtime,
Table4 Comparisonbetweenelderly(GI) andadult(GII) groupsforinitialintensity(II).
Consistency Elderly group
Adult group
p-value
Dry 34.8dB 52.4dB 0.0000a
Liquid---DL 38.6dB 5.3dB 0.0000a
Liquid---5mL 43.5dB 45.5dB 0.0611 Liquid---10mL 48.9dB 65.3dB 0.0000a
Nectar---DL 38.0dB 29.3dB 0.0000a
Nectar---5mL 44.0dB 32.6dB 0.0000a
Nectar---10mL 36.8dB 32.4dB 0.0000a
Honey---DL 38.1dB 54.2dB 0.0000a
Honey---5mL 44.5dB 40.3dB 0.0002a
Honey---10mL 41.4dB 44.1dB 0.0227a
Pudding---DL 38.2dB 38.2dB 0.8278 Pudding---5mL 44.9dB 42.5dB 0.1530 Pudding---10mL 36.7dB 36.2dB 0.7228
Student’st-test.
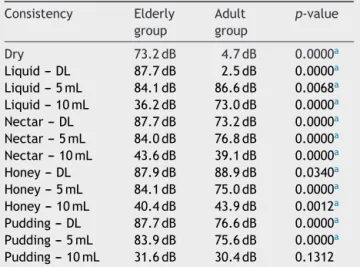
Table5 Comparison between theelderly(GI) andadult (GII)groupsforfinalintensity(FI).
Consistency Elderly group
Adult group
p-value
Dry 73.2dB 4.7dB 0.0000a
Liquid---DL 87.7dB 2.5dB 0.0000a
Liquid--- 5mL 84.1dB 86.6dB 0.0068a
Liquid--- 10mL 36.2dB 73.0dB 0.0000a
Nectar--- DL 87.7dB 73.2dB 0.0000a
Nectar---5mL 84.0dB 76.8dB 0.0000a
Nectar---10mL 43.6dB 39.1dB 0.0000a
Honey---DL 87.9dB 88.9dB 0.0340a
Honey---5mL 84.1dB 75.0dB 0.0000a
Honey---10mL 40.4dB 43.9dB 0.0012a
Pudding---DL 87.7dB 76.6dB 0.0000a
Pudding---5mL 83.9dB 75.6dB 0.0000a
Pudding---10mL 31.6dB 30.4dB 0.1312
Student’st-test.
aSignificantdifferencesatthe0.05significancelevel.
and a slower adaptation to different consistencies in the deglutition of the elderly, comparedto non-elderly adult subjects.20
The initial frequency (IF) and the initial intensity (II), which represent the beginning of swallowing,15 were less
intenseinelderlythaninadultsubjects---thatis,theformer grouppresentedlessmusclestrengthand/oradecreasein speedattheonsetofpharyngealphase.
Conversely,thefrequencyofthefirstpeak(F1P),which characterizeslaryngealelevation,15wasofgreaterintensity
intheelderlythanintheadultsubjects.Onehypothesisfor thismayberelatedtoadecreaseofsalivationintheelderly, withalowervolumeofsaliva.Therefore,elderlysubjects needmorestrengthtoaccomplishlaryngealelevation.
Theintensityforthesecondpeak(F2P),whichrepresents cricopharyngeal opening,15 was decreased in the elderly,
possiblyduetoamuscularslowingobservedinthis popula-tionforcarryingoutthisopening.21,22Theresultsonthefinal
Table6 Comparison between theelderly(GI) andadult (GII)groupsfortime(T).
Consistency Elderly group
Adult group
p-value
Dry 1.7s 0.2s 0.0000a
Liquid---DL 1.5s 0.3s 0.0000a
Liquid---5mL 1.4s 0.2s 0.0000a
Liquid---10mL 1.7s 1.6s 0.0000a
Nectar---DL 1.5s 1.2s 0.0000a
Nectar---5mL 1.4s 1.3s 0.0256a
Nectar---10mL 1.7s 1.5s 0.0040a
Honey---DL 1.5s 1.8s 0.0000a
Honey---5mL 1.4s 1.3s 0.0256a
Honey--- 10mL 1.7s 1.4s 0.0256a
Pudding---DL 1.7s 1.5s 0.0040a
Pudding---5mL 1.4s 1.3s 0.0256a
Pudding---10mL 1.6s 1.4s 0.0000a
Student’st-test.
aSignificantdifferencesatthe0.05significancelevel.
intensity (FI), which characterizes the laryngeal descent at the end of swallowing,15 may have occurred due to a
reduced laryngeal elevation found in senescent subjects, andthusthelaryngealdescentwouldbesmaller,requiring lessstrength.23
Asdescribedbyseveralauthors,theswallowingtimewas longerintheelderlyasaconsequenceofaslowerswallowing process,duetothecharacteristicsofpresbyphagia.22,24
Nostatisticallysignificantdifferencewasnotedbetween the groups during theprocess of swallowing liquids (with drink),but the frequency of thefirst peak(F1P) was less intensein theelderly. This findingmaybeexplainedby a decreaseinthedegreeoflaryngealelevation,pertinentto theagingprocess--- afindingthatparallelsthosedescribed intheliterature.25
Alldifferencesfound in this studybetween deglutition oftheelderlyandhealthyadultsareinagreementwiththe literatureaboutthispopulation,whichreportsaslowingof musclemovements,cricopharyngealsphincterand pharyn-gealclosuredysfunction,reducedlaryngealelevation,and anincreaseinswallowingtimeduringthedeglutitionprocess ofhealthyelderlypeople(thuswithpresbyphagia).26,27
In the aging process, there are differences in rela-tion to the events, and how these differences impact individuals.Thedevelopmentofswallowingtakesplace het-erogeneously,andanabilitytoadaptisthemainfeatureof ahealthyagingprocess;thismaybeonepossible explana-tionforthelackofsignificanceintheresultsbetweenthe elderlyandthenon-elderlyadults.20,28
Themultiplecharacteristicsofswallowingsoundsdepend directlyonthefoodconsistency:andanincreaseinfood con-sistencycausesdifficultyinthepreparationandorganization ofthefoodbolus,itsslowhandling,ejectiondifficulties,and adecreaseintheanteroposteriormovementofthetongue. Therefore,boththeconsistencyandvolumeoffood inter-fereintheswallowingprocess.11,29,30
Themainfeatureobservedintheelderlywasacurvewith smalleramplitudeandlongerdurationcomparedwithadult subjects. These data suggest that, in the elderly besides being slower, the swallowing process follows a broader morphofunctional accommodation in terms of mobility; however,theswallowingprocessiseffectiveandcompetent inthispopulation.
Itiscriticaltocarryoutfurtherstudiesusingthis method-ology,butwiththeadditionofexaminationsusingimaging technology, in orderto standardizethe curvesand simul-taneouslyanalyze thesound andimage of theswallowing processwithspecificsoftware.
Inmost studieson acousticanalysisof deglutition,the relationship between acoustic findings and physiological events of theswallowingprocess cannotbe clarified.The structural and functional correlation of these twoevents may enable a more accurate diagnosis, aiding in more specific therapeutic approaches and also facilitating the standardizationoftheseacousticparametersofswallowing.
Conclusion
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Appendix
1.
Questionnaire1 1.Name:
2.Gender:
()Female ()Male
3.Age:
4.Previousdiseases:
5.Haveyoueverbeenexposedtochemotherapyand/or radiotherapy?
()YES ()NO
6.Haveyoueverbeentreatedforheadand/orneck conditions?
()YES ()NO
7.Doyouhaveanystructuralchangesofheadand/or neck?
()YES ()NO
8.Doyoufeeldifficultytoswallow?
()YES ()NO
9.Doyoufeelfatigueduringmeals?
()YES ()NO
10.Doyoucoughduringoraftermeals?
()YES ()NO
11.Doyouexperienceafeelingof‘‘wetvoice’’after meals?
()YES ()NO
12.Doyouexperienceafeelingoffoodstoppinginthe throat?
()YES ()NO
13.Doyouexperiencepainordiscomfortwhen swallowingfood?
()YES ()NO
References
1.Organizac¸ão Mundial Da Saúde. Missing Voices: Views of OlderPerson onElderAbuse.OMS/NMH/NPH/02.2.Genebra: Organizac¸ãoMundialdaSaúde;2002.p.2.
2.BiltonTL,CoutoEAB.Fonoaudiologiaemgerontologia.In: Fre-itasEV,PyL,editors.Tratadodegeriatriaegerontologia.Rio deJaneiro:GuanabaraKoogan;2006.p.118---79.
3.RuoppoloG,VerneroI,SchindlerA,DeVincentiisM.La pres-bifagia e lapedofagia: dalla normalità, alladevianza e alla patologia.ActaPhonLat.2007;29:3---4.
4.Steenhagen CHVA, Motta LB. Deglutic¸ão e envelhecimento: enfoquenasmanobrasfacilitadoras eposturais utilizadasna reabilitac¸ãodopacientedisfágico.RevBrasGeriatrGerontol. 2006;9:89---100.
5.GinocchioD,BorghiE,SchindlerA.Dysphagiaassessmentinthe elderly.NutrTherMetab.2009;27:9---15.
6.GuarinoHA,ZambottiN,BiltonTL.Achados videofluoroscópi-cos dadeglutic¸ãoem pacientesadultos eidososcom queixa de tosse. In: 16◦ Congresso Brasileiro de Fonoaudiologia.
Campos do Jordão: Sociedade brasileira de Fonoaudiologia; 2008.p.1---5.Availablefrom:http://www.sbfa.org.br/portal/ anais2008/anaisselect.php?op=PR&cid=381&tid=2 [accessed 25.11.09].
7.AchemS,DeVaultK.Dysphagiainaging.JClinGastroenterol. 2005;39:357---71.
8.BorrC,Hielscher-FastabendM,LückingA.Reliabilityand valid-ityofcervicalauscultation.Dysphagia.2007;22:225---34. 9.SetaH,HashimotoK,InadaH,SugimotoA,AboM.Lateralityof
swallowinginhealthysubjectsbyAPprojectionusing videoflu-oroscopy.Dysphagia.2006;21:191---7.
10.SantosRS,Macedo-FilhoED.SonarDopplercomoinstrumento de avaliac¸ão da deglutic¸ão. Arquivos Int Otorrinolaringol. 2006;10:182---91.
11.Cagliari CF, Jurkiewicz AL, Santos RS, Marques J. Análise dos sons da deglutic¸ão pelo sonar Doppler em indivíduos normais na faixa etária pediátrica. Braz J Otorhinolaryngol. 2009;75:706---15.
12.BernardesTG[Dissertac¸ão]UsodosonarDopplercomo biofeed-back da deglutic¸ãoem pacientes com doenc¸a de Parkinson. Curitiba:(MestradoemDistúrbiosdaComunicac¸ão)--- Univer-sidadeTuiutidoParaná;2009.
13.NDD---NationalDysphagiaDietGuidelines.Standardizationfor optimalcare.Chicago:AmericanDieteticAssociation;2002. 14.TakahashiK, Groher ME, MichiK. Methodologyfor detecting
swallowingsounds.Dysphagia.1994;9:54---96.
15.HamletSL,NelsonRJ,PattersonRL.Interpretingthesoundsof swallowing:fluidflowthroughthecricopharyngeus.AnnOtol RhinolLaryngol.1990;99:749---52.
16.MckaigTN,StroudA.Thecomparisonofswallowingsoundswith simultaneouslyrecordedfluoroscopicimaging.In:Annual Meet-ingoftheDysphagiaSociety,vol.5.1996.p.31.
17.Kuhl V,Eicke BM,DieterichM, UrbanPP. Sonographic analy-sis oflaryngealelevationduring swallowing.JNeurol.2003; 250:333---7.
18.KaysS,RobbinsJ.Effectsofsensorimotorexerciseon swallow-ingoutcomes relativeto ageandage-relateddisease. Semin SpeechLang.2006;27:245---59.
19.Hind JA, Nicosia MA, Roecker EB, Carnes ML, Robbins J. Comparison ofeffortfulandnoneffortful swallowsinhealthy middle-aged and older adults. Arch Phys Med Rehabil. 2001;82:1661---5.
20.KendallKA,Leonard RJ,Mackenzie S.Commonmedical con-ditions in the elderly: impact on pharyngeal bolus transit. Dysphagia.2004;19:71---7.
21.ShethN,DinerWC.Swallowingproblemsentheelderly. Dys-phagia.1998;2:209---15.
22.DoddsWJ,StewartET,LogemannJA.Physiologyandradiology ofthenormaloralandpharyngealphasesofswallowing.AmJ Radiol.1990;154:953---63.
23.JonesB,DonnerMW.Normalandabnormalswallowing:imaging indiagnosisandtherapy.NewYork:Springer-Verlag;1991. 24.YoshikawaM,YoshidaM,NagasakiT,TanimotoK,TsugaK,
25.Leelamanit V,LimsakulC,Geater A. Synchronized electrical stimulation in treating pharyngeal dysphagia. Laryngoscope. 2002;112:2204---10.
26.FinielsH,StrubelD,JacquotJM.Deglutitiondisordersinthe elderlyepidemiologicalaspects.PresseMed.2001;30:1623---34. 27.Roy N, Stemple J, Merrill RM, Thomas L. Dysphagia in the elderly:preliminaryevidenceofprevalence,riskfactors,and socioemotional effects. Ann Otol Rhinol Laryngol. 2007;116: 858---65.
28.WilkinsT,GilliesRA,ThomasAM,WagnerPJ.Theprevalence ofdysphagiainprimary carepatients: aHamesNet Research Networkstudy.JAmBoardFamMed.2007;20:144---50. 29.TanureCMC,BarbozaJP,AmaralJP,MottaAR.Adeglutic¸ãono