PDF EN Jornal Brasileiro de Pneumologia 2 15 english
Texto
Imagem
Documentos relacionados
Ousasse apontar algumas hipóteses para a solução desse problema público a partir do exposto dos autores usados como base para fundamentação teórica, da análise dos dados
ECG, computed tomography scan, TTE) that identify and describe the size, type and setting of the lesion and general assessment. In our case, the patient had a cardiac tamponade due
A computed tomography scan of the chest revealed a 4-cm mass with heterogeneous content and pleural extension to the level of the lingula, as well as two micronodules in
A computed tomography scan of the chest revealed atelectasis of the right upper lobe (caused by occlusion of the upper lobe bronchus) that extended up to the juxtacarinal portion of
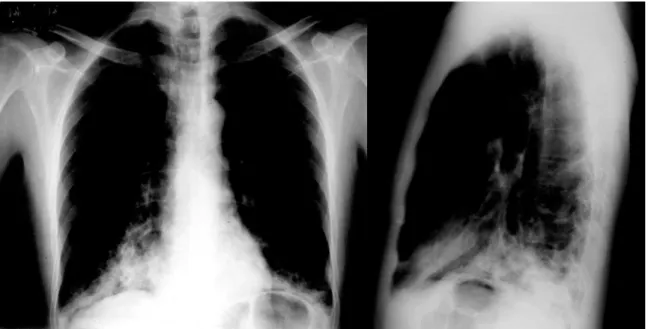
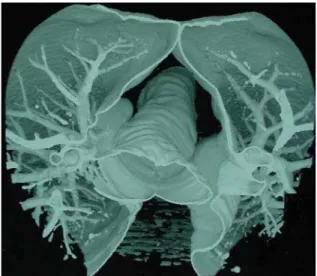
The working diagnosis was superior vena cava syndrome, and the patient was submitted to computed tomography of the chest, which revealed a mass in the anterior mediastinum, with
A computed tomography scan of the chest revealed a 4-cm mass with heterogeneous content and pleural extension to the level of the lingula, as well as two micronodules in
Computed tomography of the chest revealed consolidation with interposed cavitation in the right upper lobe.. Fiberoptic bronchoscopy revealed purulent fluid within
Food biotechnology, Food safety, Food quality and safety, Process Engineering, Life science Technology, Nutrition & Food science, Food and nutrition, Food quality, safety
