REVISTA
PAULISTA
DE
PEDIATRIA
www.rpped.com.br
ORIGINAL
ARTICLE
Otitis
media
with
effusion
in
children
younger
than
1
year
Renata
Cantisani
Di
Francesco
a,∗,
Vivian
Boschesi
Barros
b,
Rafael
Ramos
baFaculdadedeMedicina,UniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil
bHospitaldasClínicas,FaculdadedeMedicina,UniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil
Received6April2015;accepted9August2015 Availableonline29January2016
KEYWORDS Otitismediawith effusion;
Infant; Riskfactors
Abstract
Objective: Todeterminetheprevalenceofotitismediawitheffusioninchildrenyoungerthan 1yearanditsassociationwiththeseasonoftheyear,artificialfeeding,environmentaland perinatalfactors.
Methods: Retrospectivestudy of184randomlyincludedmedicalrecordsfromatotal of982 healthyinfantsevaluatedforhearingscreeningtests.Diagnosisofotitismediawitheffusion wasbasedonotoscopy(amber-goldcolor,fluidlevel,handleofmalleusposition),typeB tym-panometriccurvesandabsenceofotoacousticemissions.Incompletemedicalrecordsorthose describingacuteotitismedia, upperrespiratorytractinfectionsontheassessmentdayorin thelast3months,neuropathiesandcraniofacialanomalieswereexcluded.Datasuchas gesta-tionalage,birthweight,Apgarscore,typeoffeedinganddaycareattendancewerecompared between children with and without otitis mediawith effusion through likelihoodtests and multivariateanalysis.
Results: 25.3%of184infantshadotitismediawithbilateraleffusion;9.2%hadunilateral.In infantswithotitismedia,thefollowingwereobserved:chronologicalageof9.6±1.7months; gestationalage>38weeksin43.4%andbirthweight>2500gin48.4%.Otitismediawitheffusion wasassociated withwinter/fall,artificialfeeding, Apgarscore<7anddaycareattendance. Themultivariateanalysisshowedthatartificialfeedingisthefactormostoftenassociatedto otitismediawitheffusion.
Conclusions: Otitismediawitheffusionwasfoundinaboutonethirdofchildrenyoungerthan 1yearandwasmainlyassociatedwithartificialfeeding.
©2015SociedadedePediatriadeSãoPaulo.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBYlicense(https://creativecommons.org/licenses/by/4.0/).
∗Correspondingauthor.
E-mail:[email protected](R.C.DiFrancesco).
http://dx.doi.org/10.1016/j.rppede.2016.01.003
PALAVRAS-CHAVE Otitemédiacom derrame; Lactente; Fatoresderisco
Otitemédiacomefusãoemcrianc¸asmenoresdeumano
Resumo
Objetivo: Determinar prevalênciadeotite médiacomefusãoem menoresdeum ano esua associac¸ãocomestac¸ãodoano,aleitamentoartificial,fatoresambientaiseperinatais.
Métodos: Estudoretrospectivocom184 prontuáriosincluídos deformarandomizada dentre 982lactentessaudáveisavaliadosparatestesdetriagemauditiva.Diagnósticodeotitemédia com efusão baseou-se em otoscopia (colorac¸ão âmbar-ouro, nível líquido,posic¸ão do cabo do martelo), curva timpanométrica tipo B e otoemissões acústicas ausentes. Excluíram-se prontuáriosincompletosouquedescreviamotitemédiaaguda,infecc¸õesdeviasaéreas super-iores nodia daavaliac¸ão ounosúltimostrês meses,neuropatiase anomaliascraniofaciais. Dadoscomoidadegestacional,pesoaonascimento,Apgar,tipodealeitamento,frequênciaà crecheforamcomparadosentrecrianc¸ascomesemotitescomefusãopormeiodetestesde verossimilhanc¸aeanálisemultivariada.
Resultados: 25,3%dos184lactentesapresentavamotitemédiacomefusãobilateral;9,2% uni-lateral.Noslactentescomotitemédia,observou-seidadecronológica9,6±1,7meses;idade gestacional>38semanasem43,4%epesoaonascer>2.500gem48,4%.Otitemédiacomefusão foi associada ao inverno/outono, aleitamento artificial,Índice de Apgar<7 e atendimento à creche.Jáa análisemultivariadademonstrou queo aleitamentoartificial éo fatormais associadoàotitemédiacomefusão.
Conclusões: Aotitemédiacomefusãofoiencontradaemcercade1/3dosmenoresdeumano eprincipalmenteassociadaaoaleitamentoartificial.
©2015SociedadedePediatriadeSãoPaulo.PublicadoporElsevierEditoraLtda.Esteéumartigo OpenAccesssobalicençaCCBY(https://creativecommons.org/licenses/by/4.0/deed.pt).
Introduction
Otitismediawitheffusion(OME)isacommonchronic condi-tion and usually asymptomatic in children. OME is a risk factorforacuteotitismediaandforsleepdisorders,lossof appetiteandearpainandhaspsychosocialimpacts,which, inthelongterm,mayresultinbehavioral,1speechand lan-guagedevelopmentdisorders.2Itischaracterizedbymiddle earinflammation,whichisfilledwithafluid(effusion)and withnoclinicalsignsofinfection.3
Itsdiagnosisinnewbornsandinfantsisparticularly diffi-cultandinherenttothedifficultyofperformingtheotoscopy inthisagegroup,notonlybythesizeoftheearcanal,but alsoduetothepatient’slackofcooperation,thepresence of cerumen andthe difficulty in removing it.4 OMEoften goesundetectedandundiagnosedbecauseitdoesnothave asymptomaticpictureasimportantasacuteotitismedia. Itcanspontaneouslyoccurduetoreducedfunctionof the eustachiantubeor theresultofapreviousinfectious pro-cess,amongothers.5
The presenceofmiddle earsecretionandtheresulting decreasedmobilityofthetympanicmembraneconstitutea barriertosoundconductionanddamagethebaby’sauditory acuity.6 Itsmain sequelis auditoryand itsmainimpactis languageandcognitionimpairment.7
The difficulties of diagnosingOME duringthe firstyear of life make the disease be poorly studied and consider-ingitsconsequences,itisextremelyimportanttostudythe factors associatedwiththis age group, aswell asto bet-terunderstanditsevolution.Therefore,bettertherapeutic interventioncanbeachievedandpreventioncriteriacanbe bettertargeted.
Inthiscontext,theaimofthisstudy wastodetermine theprevalenceofotitismediawitheffusionduringthefirst yearoflifeanditspossibleassociationwiththeseasonofthe year,artificialfeeding,perinatalandenvironmentalfactors.
Method
ThisstudywasapprovedbytheInstitutionalReview Board ofHospital das Clínicas daFaculdade de Medicina deSão Paulo(1378/09).Thisisaretrospectivestudybasedonthe analysisofmedicalrecordsofinfantsbornatHC-FMUSP.
In2008duetotechnicalproblems,theneonatalhearing screeningwasinterruptedinourhospitalforapproximately eightmonths.Atotalof1800childrenwerenotsubmitted tothetests.Theywererecalledin2009and,ofthese,982 childrenaged1---12monthscamefortheassessment.
Recordsof20%ofthe982healthychildrenbetweenone and 12 months, who were recalled for neonatal hearing screening,wererandomlyselected(random.org)toassess theprevalenceofotitismediawitheffusion.Iftheselected subjectshowedanyoftheexclusioncriteriabelow,thenext subjectintherandomlistwasincludedandthus,184 chil-dren’srecordswereselected(Fig.1).
1800 children did not undergo newborn hearing screening in 2008 and were recalled in
2009
982 children aged 1 to 12 months underwent hearing screening
184 medical records Medical records of 20%
of the children were randomly selected (random.org)
Figure1 Patientselection.
the last threemonths or severe neurological disease and Apgar<5 at the fifth minute of life and/or craniofacial anomalies(e.g.,cleftpalate,trisomy21andothers)were excludedfromthisstudy.
Thefollowinginformationhadtobeincludedinthe medi-calrecord for thediagnosis of otitismedia witheffusion: otoscopywithcharacteristics ofotitismediawitheffusion and absent response in the transient evoked otoacoustic emissions test and type B tympanometry.8 The otoscopy should have three of the following criteria: loss of light reflex,thickening,amber-goldcolorduetomiddleear effu-sion, air-fluid level, more horizontal appearance of the handle of malleus and retraction pockets. The transient evokedotoacousticemissions---TOAE---wereperformedin allchildren using an Ero-scan device (MAICO®,Denmark),
comprisingthefrequencyrangefrom2000---4000Hz,atthe F1intensityof65dBNPS---F255dBNPSandimpedancetests withanInteracoustics AZ7manual impedanceaudiometer (1000Hzprobe,Interacoustic®,Denmark).
The following data on the past clinical history of the childrenwereobtainedfromthemedicalrecords:gender, gestationalage,birthweight,Apgarscoreatfiveminutes, breastfeedinganddaycareattendance.Positive breastfeed-ing wasconsidered for those children receiving exclusive breastfeeding during the assessment or who were exclu-sivelybreastfedforthefirstsixmonthsoflife.
TheStatisticalPackageforSocialSciences(SPSS)version 20.0 was used for the statistical analysis. The likelihood test was used to verify the differences in prevalence of otitismedia amongdifferent seasons of the year andthe chi-squaretestwasusedtoanalyzetheassociationofotitis mediawithothervariables.
Themultivariateanalysiswasusedtoanalyzethefactors associated with the presence of OME adjusted for con-foundingvariables.Differencesforp<0.050wereconsidered statisticallysignificant.Forthemultivariatelogistic regres-sion,the factors that were significantlyassociated in the univariateanalysiswereselected.
Results
Themedicalrecordsof184childrenwereanalyzed,witha meanageof9.6±1.7months.Table1showsthedistribution ofgender,age,gestationalageandbirthweight.Forty-five (24.5%)childrenhadotitismediawitheffusioninbothears and17 (9.2%) children hadit in one ear.A prevalence of otitiswitheffusionof33.7%wasfound.Otitiswitheffusion wasmorefrequentduringthefallandwinter(Table2).
Table 1 Gender, gestational age and birth weight distribution.
Category Frequency %
Gender
Female 91 49.2
Male 94 50.8
Age
≤6months 8 4.3 >6months 176 95.7
Gestationalage
>38weeks 78 42.4 27---34weeks 34 18.5 34---38weeks 72 39.1
Birthweight
<1500g 20 10.9 >2500g 89 48.4 1500---2500g 75 40.8
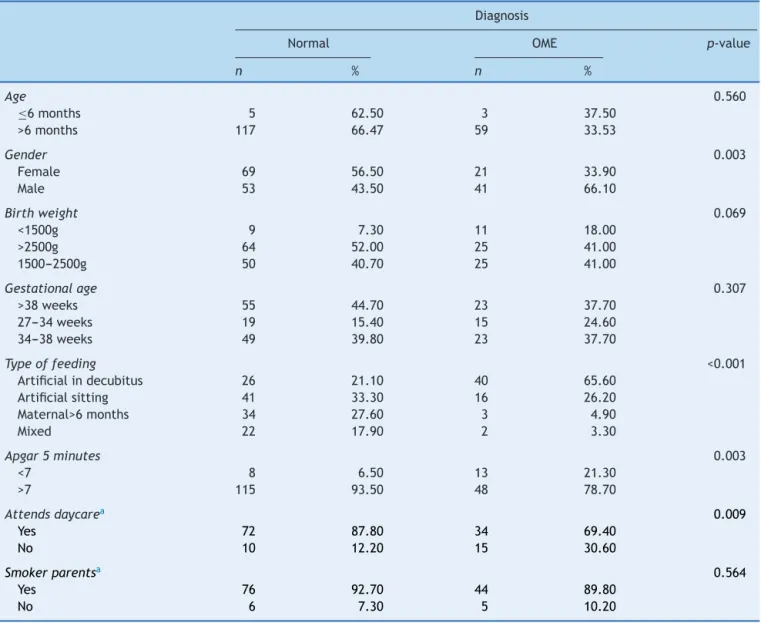
Table3showstheassociationofeffusioninthemiddleear withthemalegender;Apgarscoreatfiveminutes<7, artifi-cialfeedinganddaycareattendance.Age,gestationalage, birthweightandparentalsmokingwerenotassociatedwith OME.However,whenapplyingmultivariatelogistic regres-sion (Table4), it can beobserved that the most relevant factorassociatedwithotitismediawitheffusionisthetype ofbreastfeeding.
Discussion
Otitismediawitheffusionisthemostcommoncauseof hear-inglossinchildhood;itoccursmoreoftenduringtheperiod oflanguagedevelopmentandcanaffectit.1
Therehave been many studies on OME;however, they mostlyomitinfants or newborns.This condition isa com-moncauseof falsepositive resultinthe newbornhearing screeningtest.9
Inthisseriesofchildrenyoungerthanoneyear,OMEwas found in approximately a third of the children, similarly towhatwas foundby Marchantetal.10 However,in their series,70% of cases of otitis witheffusion occurred after recurrentepisodesofacuteinfection.11 Weexcluded data fromchildrenwithacuteotitismedia(AOM)intheprevious threemonthsbecauseitiscommonforfluidtopersistinthe
Table2 Prevalenceofotitismediawithotitiswitheffusion andseasonoftheyear.
Season Diagnosis Total Normal
n(%)
OME
n(%)
n(%)
Winter 44(57.9%) 32(42.1%) 76(100%) Fall 43(66.2) 22(33.8) 65(100%) Spring 25(89.3%) 3(10.7%) 28(100%) Summer 11(73.3%) 4(26.7%) 15(100%) Total 123(66.9%) 61(33.2%) 185(100%)
Table3 Middleeareffusionandassociationwithperinatalandenvironmentalfactors. Diagnosis
Normal OME p-value
n % n %
Age 0.560
≤6months 5 62.50 3 37.50 >6months 117 66.47 59 33.53
Gender 0.003
Female 69 56.50 21 33.90
Male 53 43.50 41 66.10
Birthweight 0.069
<1500g 9 7.30 11 18.00 >2500g 64 52.00 25 41.00 1500---2500g 50 40.70 25 41.00
Gestationalage 0.307
>38weeks 55 44.70 23 37.70 27---34weeks 19 15.40 15 24.60 34---38weeks 49 39.80 23 37.70
Typeoffeeding <0.001
Artificialindecubitus 26 21.10 40 65.60 Artificialsitting 41 33.30 16 26.20 Maternal>6months 34 27.60 3 4.90
Mixed 22 17.90 2 3.30
Apgar5minutes 0.003
<7 8 6.50 13 21.30
>7 115 93.50 48 78.70
Attendsdaycarea 0.009
Yes 72 87.80 34 69.40
No 10 12.20 15 30.60
Smokerparentsa 0.564
Yes 76 92.70 44 89.80
No 6 7.30 5 10.20
a Notallfileshaddataondaycarecenterattendanceandsmoker/nonsmokerparents.
Table4 Multivariateanalysisofperinatalandenvironmentalfactorsrelatedtootitismediawitheffusioninchildrenyounger than1year.
Coefficientofregression Standarderror OddsRatio 95%confidenceinterval p-value Artificialfeeding −0.89 0.21 0.40 0.26---0.62 <0.001 Apgar −0.92 0.63 0.39 0.11---1.39 0.149 Daycarecenter 0.91 0.55 2.49 0.83---7.44 0.102
middleearafterthisepisode.Rosenfeldetal.2describeda resolutionrateof50%withinonemonth,60% withinthree monthsand75%atsixmonths.Thepresenceofmiddleear effusionformorethanthreemonthscharacterizesachronic conditionandisofgreatimportanceforthedevelopmentof hearingloss.6
OMEis a multifactorialdiseasedeterminedby environ-mental,socioeconomicandgeneticfactors.12
TherewasnoassociationofagewithOME,probablydue tothesmallsamplesize.Thehighnumberofchildrenwith lowbirthweightandgestationalagelessthan38weeksis
explainedby our hospital profile. It is a tertiary referral centerformotherswithhigh-riskpregnancies.
Onceagainitwasdemonstratedthatartificialfeedingis apredisposingfactor for otitis mediawitheffusion andit isthemostimportantfactor amongotherstatistically sig-nificantones. Childrenwhowerebreastfedfor morethan sixmonthsarelesspronetoOME,mainlythosewhodonot attenddaycarecenters.14Breastfeedingduringthefirstyear oflifehasaprotectiveeffectforthedevelopmentofOME, whichcorroboratesthemajorityofresearchers.15Thisfactis probablyrelatedtothepositioningofthehead,exposureto differentmicroorganisms,improved nutritionand antibac-terialorimmunologicalbenefitsofbreastmilk.15Thesupine positionwithoutelevationofthetrunkwasalsoassociated withOMEandisconsistentwithotherauthors.16
Children who attended daycare showed an increased prevalenceofOME;thesechildrenareexposedtoa diver-sityofviralandbacterialpathogens,inadditiontoincreased person-to-personcontact.17
We found no association between OME and parental smoking,whichdiffersfromotherstudiesthatindicatethat thisfactorcanincreasetwo-foldtheriskofdeveloping oti-tismedia. It should be noted, however, that this sample included a high number of parents who smoked, in both groups.18
Therewasalsonoassociationwithpretermdeliveryand lowbirthweight;however,alowerApgarscoreatfive min-utes was associated with OME. Children with low Apgar scoreshaveothercomorbiditiesnotstudiedinthisworkand mayhavebeendeprivedofmaternalbreastfeeding,19 even thoughweexcludedchildrenwithverylowApgarscores.
Thisstudyextendsthecurrentknowledgeonthe preva-lenceof OMEin childrenyoungerthanoneyear;however, ithaslimitations,suchastheretrospectiveanalysisandthe absenceof dataonhearing thresholds,requiring sophisti-catedteststhatareoftenperformedundersedation,which arenotcarriedoutinallchildrenatthehearingscreening protocol.Theexternalvalidityofthestudyisalsolimited, becauseof the totalnumber of 1800 children recalled to undergo the neonatal screening, only 982 were able to undergoallthetests.
This study demonstrates onceagain the importanceof breastfeeding as a protective factor for otitis with effu-sion and also the importance of routinely performing an otoscopyininfants,despitethedifficultytodoit,evenin asymptomatic children. This practicewould influence the therapeuticmanagementofOME,includingthereferralof thesechildrentothespecialist,inordertoquicklyrestore hearing,soimportantforspeechandlanguagedevelopment. The hearing loss in OME, although mild, can also lead to behavioralproblemssuchashyperactivityandinattention, schooldeficitsandcognitivedifficultieslaterinthechild’s life.1
Itcanbeconcludedthatmiddleeareffusionwaspresent inapproximatelyonethirdofinfantsyoungerthanoneyear andthefactor moststronglyassociatedwiththepresence ofotitismediawitheffusionwasartificialfeeding.
Funding
Fundac¸ão de Amparo à Pesquisa do Estado de São Paulo (FAPESP)Brazil.
Conflicts
of
interest
Theautorsdeclarenoconflictsofinterest.
Acknowledgements
ToFundac¸ãodeAmparoàPesquisadoEstadodeSãoPaulo (FAPESP)forthescientificinitiationgranttoVivianBoschesi Barros,Processn.2013/19538-0.
References
1.HallAJ,MawAR,SteerCD.Developmentaloutcomesinearly compared with delayed surgery for glue ear up to age 7 years:arandomisedcontrolledtrial.ClinOtolaryngol.2009;34: 12---20.
2.RosenfeldR,SchwartzSR,PynnonenMA,TunkelDE,HusseyHM, FicheraJS, et al. Clinicalpractice guideline: tympanostomy tubesinchildren.OtolaryngolHeadNeckSurg.2013;149Suppl. 1:S1---35.
3.NorthernJL,DownsMP.Otitemédia.In:NorthernJL,DownsMP, editors.Audic¸ãonaInfância.5thed.RiodeJaneiro:Guanabara; 2005.p.54---73.
4.CasselbrantML, MandelEM. Epidemiology. In: RosenfeldRM, Bluestone CD,editors.Evidence-based otitismedia. 2nd ed. Hamilton:BCDeckerInc.;2003.p.147---62.
5.Williamson I. Otitis media with effusion. Clin Evid. 2002;7:469---76.
6.RosenfeldR,CulpepperL,DoyleKJ,GrundfastKM,Hoberman A, Kenna MA,et al. Clinicalpractice guideline: otitismedia witheffusion. Otolaryngol Head Neck Surg. 2004;130 Suppl. 5:S95---118.
7.RoversMM.Theburdenofotitismedia.Vaccine.2008;26Suppl. 7:G2---4.
8.JergerJ.Clinicalexperiencewithimpedanceaudiometry.Arch Otolaryngol.1970;92:311---24.
9.Boone RT, Bower CM, Martin PF. Failed newborn hearing screensaspresentation forotitismediawitheffusion inthe newbornpopulation.IntJPediatrOtorhinolaryngol.2005;69: 393---7.
10.Marchant CD, Shurin PA, Turczyk VA, Wasikowski DE, Tuti-hasi MA, Kinney SE. Course and outcome of otitis media in early infancy: a prospective study. J Pediatr. 1984;104: 826---31.
11.Boudewyns A, Declau F, Vanden Ende J, Van Kerschaver E, DirckxS,Hofkens-VandenBrandtA, etal.Otitismediawith effusion:anunderestimated causeofhearinglossininfants. OtolNeurotol.2011;32:799---804.
12.CoticchiaJM,ChenM,SachdevaL,MutchnickS.Newparadigms inthepathogenesisofotitismediainchildren.FrontPediatr. 2013;1:52.
13.Brauer M, Gehring U, Brunekreef B, Jongste J, Gerritsen J, RoversM,etal.Traffic-relatedairpollutionandotitismedia. EnvironHealthPerspect.2006;114:1414---8.
14.Daly KA, Hoffman HJ, Kvaerner KJ, Kvestad E, Casselbrant ML, Homoe P, et al. Epidemiology, naturalhistory, and risk factors:panelreportfromtheninthinternationalresearch con-ferenceonotitismedia.IntJPediatrOtorhinolaryngol.2010;74: 231---40.
16.TullySB,Bar-HaimY,BradleyRL.Abnormaltympanographyafter supinebottlefeeding.JPediatr.1995;126:S105---11.
17.GreenbergD, HoffmanS, Leibovitz E,Dagan R. Acuteotitis mediainchildren:associationwithdaycarecenters--- antibac-terialresistance,treatment,and prevention.PaediatrDrugs. 2008;10:75---83.
18.CsákányiZ,CzinnerA,SpanglerJ,RogersT,KatonaG. Relation-shipofenvironmental tobaccosmoketootitismedia(OM)in children.IntJPediatrOtorhinolaryngol.2012;76:989---93.