w w w . r b o . o r g . b r
Original
article
Platelet-rich
plasma
(PRP)
applied
during
total
knee
arthroplasty
夽
João
Paulo
Fernandes
Guerreiro
a,∗,
Marcus
Vinicius
Danieli
a,
Alexandre
Oliveira
Queiroz
a,
Elenice
Deffune
b,
Rosana
Rossi
Ferreira
baUniort.eOrthopedicsHospital,SantaCasadeLondrina,Londrina,PR,Brazil
bHemocenterofBotucatu,FaculdadedeMedicinadeBotucatu(UNESP),Botucatu,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received22April2014 Accepted26May2014 Availableonline12March2015
Keywords:
Arthroplasty Knee Transfusion Platelet-richplasma Hemorrhage
a
b
s
t
r
a
c
t
Objective:To evaluate the efficacy of platelet-rich plasma regarding healing, pain and hemostasisaftertotalkneearthroplasty,bymeansofablindedrandomizedcontrolledand blindedclinicalstudy.
Methods:Fortypatientswhoweregoingtoundergoimplantationofatotalkneeprosthesis wereselectedandrandomized.In20ofthesepatients,platelet-richplasmawasapplied beforethejointcapsulewasclosed.Thehemoglobin(mg/dL)andhematocrit(%)levelswere assayedbeforetheoperationand24and48hafterwards.TheWomacquestionnaireand averbalpainscalewereappliedandkneerangeofmotionmeasurementsweremadeup tothesecondpostoperativemonth.Thestatisticalanalysiscomparedtheresultswiththe aimofdeterminingwhethertherewereanydifferencesbetweenthegroupsateachofthe evaluationtimes.
Results:Thehemoglobin(mg/dL)andhematocrit(%)measurementsmadebeforethe opera-tionand24and48hafterwardsdidnotshowanysignificantdifferencesbetweenthegroups (p>0.05).TheWomacquestionnaireandtherangeofmotionmeasuredbeforethe opera-tionanduptothefirsttwomonthsalsodidnotshowanystatisticaldifferencesbetween thegroups(p>0.05).Thepainevaluationusingtheverbalscaleshowedthattherewasan advantageforthegroupthatreceivedplatelet-richplasma,24h,48h,oneweek,threeweeks andtwomonthsaftertheoperation(p<0.05).
Conclusions:Inthemannerinwhichtheplatelet-richplasmawasused,itwasnotshownto beeffectiveforreducingbleedingorimprovingkneefunctionafterarthroplasty,in compar-isonwiththecontrols.Therewasanadvantageonthepostoperativeverbalpainscale.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkdevelopedatSantaCasadeLondrina,PR,BrazilandattheHemocenterofBotucatuMedicalSchool(UNESP),Botucatu,SP,Brazil.
∗ Correspondingauthor.
E-mails:[email protected],[email protected](J.P.F.Guerreiro). http://dx.doi.org/10.1016/j.rboe.2015.02.014
Plasma
rico
em
plaquetas
(PRP)
aplicado
na
artroplastia
total
do
joelho
Palavras-chave:
Artroplastia Joelho Transfusão
Plasmaricoemplaquetas Hemorragia
r
e
s
u
m
o
Objetivos:Avaliar,pormeiodeumestudoclínico,randomizado,controladoecego,aeficácia doplasmaricoemplaquetasnacicatrizac¸ão,dorehemostasiaapósartroplastiatotaldo joelho.
Métodos: Foramselecionados40pacientesqueseriamsubmetidosaprótesetotaldojoelho erandomizados.Em20dessespacientesfoiaplicadooplasmaricoemplaquetasantes do fechamentoda cápsula articular. Foram feitas dosagensde hemoglobina (mg/dL) e hematócrito(%)nopré-operatório,após24e48horasdacirurgia.Foramaplicadoso ques-tionárioWomaceaescalaverbaldadoremedidasasamplitudesdemovimentodojoelho atéosegundomêspós-operatório.Aanáliseestatísticacomparouosresultadosafimde comprovarhaverdiferenc¸aentreosgruposemcadaumdosmomentosdaavaliac¸ão.
Resultados: Medidasdovalorda hemoglobina(mg/dL)ehematócrito (%) feitasno pré-operatório,após24e48horasdacirurgia,nãomostraramdiferenc¸assignificativasentre osgrupos(p>0,05).OquestionárioWomaceaamplitudedemovimentomedidano pré-operatórioeatéosdoisprimeirosmesestambémnãomostraramdiferenc¸asestatísticas entreosgrupos(p>0,05).Aavaliac¸ãodadorpormeiodaescalaverbalmostrouvantagem nogrupoqueusouoplasmaricoemplaquetasapós24e48horas,umaetrêssemanase doismesesdepós-operatório(p<0,05).
Conclusões: Damaneiracomquefoiusado,oplasmaricoemplaquetasnãosemostrou efetivoparareduzirsangramentooumelhorarafunc¸ãodojoelhoapósaartroplastiaem comparac¸ãocomoscontroles.Houvevantagemnaescalaverbaldedorpós-operatória.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Totalkneearthroplastyisdeemedtobesuccessfulwhen com-pletetissuehealing,paincontrolandgoodjointfunctioning areachieved.1
Majorpostoperativebleedingfrequentlyoccurs.1,2By
min-imizing the bleeding, the need for transfusion is avoided andformationofhematomasandseromasthatmightcause pain,impairmentoftherangeofmotion,disordersofwound healingandprolongedhospitalstaysareprevented.2,3Blood
transfusion issubject tosideeffects, suchas immunologi-calreactionsandinfections.2,3Infectionsmayoccurdirectly
through contamination4 or through greater susceptibility
inducedbymeansofimmunomodulation.4Useofautologous
blood has not been shown to be a betteroption than the homologousblood thatisroutinelyused.1,5,6Inanattempt
toreducethebleeding,manysurgeonsremovethetourniquet fromthelimbbeforeclosingthejointcapsuleandwoundin ordertoachievehemostasis.However,thisnotonlyincreases thedurationoftheoperationbutalsodoesnotpresentproven efficacy.1,7–9Useoffibringlue,whichisproducedfromhuman
plasmaand,forthisreason,isalsosubjecttocontamination andimmunologicalreactions,haspresentedgoodresultswith regardtocontrollingbleeding,throughactingasahemostatic agent.10–13
Fromthegoodinitialresultsobtainedwithfibringlue,10–12
butbearinginmindtherisksofcross-contaminationandthe difficulty inobtainingthis agent,11 Whitmanet al. (1997)14
describedtheuseofconcentratesofautologousplateletsfor
improving the healing. Antibacterial and antifungaleffects havealsobeenobservedrecently.15
Since then, products containing growth factors derived from platelets havebeenusedunder thename of platelet-richplasma(PRP),inavarietyofsituationswithinmedicine anddentistry.12PRPisalsoknownasplatelet-enrichedplasma
(PeRP),platelet-richconcentrate(PRC)orautologousplatelet gel.12PRPhasbeenproducedbymeansofcentrifugationofthe
patient’sownblood,collectedminutesbeforethesurgery.2
ThegrowthfactorspresentinPRParecytosinesthatcome frombloodandarepartofthenaturalhealingprocess.This process can be modified and accelerated according to the concentration of these factors.15 These cytosines have an
importantroleinrelationtocellproliferation,chemotaxis,cell differentiationandangiogenesis.15
In2000,duringthecongressoftheAmericanAcademyof Orthopedics,Mooar etal.16 demonstrated the useof
autol-ogousplateletgelduringthepostoperativeperiodfollowing implantationoftotalkneeprostheses,forthefirsttime,with goodresults.
Startingin2006,studiesontheuseofPRPsubsequentto totalknee arthroplastyhavebeen published,showinggood results.1–3,17Inthesestudies,useofPRPresultedinlowerblood
loss,fewerbloodtransfusions,betterhealing,less postopera-tive pain and infection and shorterhospital stay.1–3,17 Two
randomizedprospectivestudiesonthistopichavebeen pub-lishedsofar.OneofthemdidnotshowanybenefitfromPRPin relationtothecontrols,18whiletheotherstudyshowedsome
Table1–Modelforthechartusedtogatherdataontheparametersanalyzedatthedifferentassessmenttimes,before andaftertheoperation.
Before 24hafter 48hafter 7daysafter 21daysafter 2monthsafter
Hb X X X
Ht X X X
ROM X X X X X X
Pain X X X X X X
WOMAC X X
Transfusion X X
Wound X X X X X
Hb,hemoglobin;Ht,hematocrit;ROM,rangeofmotionoftheknee;Pain,verbalpainscale;WOMAC,WesternOntarioandMcMasterUniversities Index19;Transfusion,evaluationofneedforbloodtransfusion;Wound,observationofanyabnormalitiesofhealing.
Thehypothesisofthepresentstudy wasthatuseofPRP wouldbeeffectiveforcontrollingpainandbleedingandwould improvethehealingaftertotalkneearthroplasty.
TheaimofthisstudywastoevaluatetheefficacyofPRP withregardtohealing,painandhemostasisaftertotalknee arthroplasty.
Sample
and
methods
Thiswasablindedrandomizedclinicalstudy.Theprojecthad beenapprovedbyourinstitution’sresearchethicscommittee. Fortypatientswithanindicationfortotalkneearthroplasty whowereattendedatourinstitution’soutpatientclinicwere selected.
Theinclusioncriteriawerethatthepatientneededtohave receivedexplanationsaboutthestudyandtopresent three-compartmentosteoarthrosis ofthe knee. They could beof eithersexandneeded tohaveanindicationfortotalknee prosthesis.
Patientspresentingthefollowingcriteriawereexcluded:major deformitiesthatwouldleadtomoreextensivebonecutsor soft-tissuerelease;inflammatorydiseases;orprevioussurgery onthekneetobeoperated.
Thepatientswereadvisedthat,forinclusioninthestudy, theyneededtosignthefreeandinformedconsentstatement (Appendix1).
Definitionofthegroups
Theexperimentalgroup(20patients)underwent implanta-tionofatotalkneeprosthesisandreceivedanintra-articular applicationofPRP.
Thecontrolgroup(20patients)underwentimplantationof atotalkneeprosthesiswithoutreceivinganyintra-articular applicationofPRP.
Theindividualsweredividedbetweenthetwogroups ran-domlybymeansofadraw.Thepatientswerenotinformed regardingthe grouptowhich theybelongedand remained totallyunawareofthisinformationuntiltheendoftheproject.
Data-gathering
Data-gathering(Table1)beforeandaftertheoperation com-prisedthefollowing:
1. Serum hemoglobin (Hb) and hematocrit (Ht) tests per-formed before the operation and 24 and 48h after the operation.Theneedfortransfusionwasevaluated. 2. Clinical examination of range of motion and pain. For
this,goniometryandaverbalpainscale(scoresbetween 0 and 10, such that 0 was free from pain and 10 was the worst pain) were used at the following times after the operation: 24–48h, seven days, 21 days and two months. Any abnormalities ofwoundhealingwere also noted.
3. Toevaluatekneefunctioningbeforetheoperationandtwo monthsaftertheoperation,theWOMACinstrumentwas used,initsversiontranslatedandvalidatedforuseinthe Portugueselanguage19(Appendix2).
The surgical technique was the one established in the current literature,withmedialpatellar accessand applica-tionofPRPtotheentireexposedportionofthejoint,inthe casesselectedforthis(Figs.1–6).Alltheprocedureswere per-formedbythesamesurgeon,usingthesameinstrumentsand implantedmaterial.
Fig.2–PRPimmediatelybeforeapplication.
Fig.3–ApplicationofPRPtothejointcavity.
Postoperativeprotocolused
1. During thehospitalstay, the followingwasusedas an analgesic:1gofdipyroneintravenouslyevery sixhours and100mgtramadolhydrochlorideeveryeighthours;
Fig.4–ApplicationofPRPtothejointcavity.
Fig.5–Closureofthejointcapsule.
2. Patientswithpainscoredasmorethansevenontheverbal painscalereceived4mgofmorphineintravenouslyevery fourhours;
3. After discharge from hospital, the patients were pre-scribed 1g of dipyrone orally every six hours if pain occurred, and 50mg of tramadol hydrochloride orally everysixhoursif thepain continuedevenaftertaking dipyrone;
4. Allthe patientsreceivedprophylaxisagainstdeep vein thrombosiscomprising a dose of 40mg of enoxaparin subcutaneously,24–48hafterthesurgery,andtheywere prescribed10mgofrivaroxabandaily,forafurther10days athome;
Fig.6–Closureoftheskinandsubcutaneoustissue.
wasinduced,followedby1gofcefazolineveryeighthours for48h;
6. Thedressingwaschangedatthehospitalonthesecond dayaftertheoperation,beforedischargefromthe hos-pital,intheoutpatientclinicontheseventhdayandat homeevery dayuntilthestitcheswereremovedonthe 21stday;
7. The patients used a walking frame for 21 days, with full weight-bearing from the second postoperative day onwards;
8. Physiotherapywasstartedwhilethepatientwasstillin hospitalandwascontinueduntilthesecond postopera-tivemonthaftertheoperation;
9. Radiologicalexaminationswereperformedontheknees duringtheimmediatepostoperativeperiodandinthe out-patient clinicofSantaCasa attheoutpatientvisit two monthsaftertheoperation;
10. Theparametersevaluatedatthereturnvisitswereas fol-lows:painandsymptomsrelatingtotheknee;rangeof motion;satisfaction;andlimbalignmentand function-ing(abilitytowalk,useofsticks,useofstairsandramps, sittingdownandstandingup,etc.).
PreparationofthePRP
ThePRPwaspreparedbyaprofessionalwithskillsandtraining forthisprocess.
Asampleof20mLofbloodwascollectedfromeachpatient in5mLvacuumtubescontaining10%sodiumcitratefor anti-coagulation.Thetubeswerecentrifuged(Fanem®)at1200rpm for 10min, at room temperature in a centrifuge of radius 6.5cm.Theresultfromthiscentrifugationenabledseparation ofthreecomponents:redcells(bottomofthetube),whitecells (thinlayerontopoftheredcells)andplasma(toplayer)(Fig.7).
Fig.7–Plasmabeingremoved.
Theplasmawasdecantedintoanothersteriletube,ofcapacity 10mL,andwascentrifugedagaininthesamemachineatthe samespeed,forfiveminutes.Attheendofthis centrifuga-tion,theupperplasmalayerthatwasobtained(accountingfor approximately50%)wasdiscardedbecauseofthesmall quan-tityofplatelets.Thelowerportion,whichwasrichinplatelets andwasnamedplatelet-richplasma,wasplacedinasterile Petridishinthesurgicalfield.Followingthis,itwasplacedina syringeforthesurgeontoapply.AproportionofthePRPfrom everyfifthpatientwasseparatedoutandsubjectedtoanalysis onthenumberofplatelets,inanautomaticcounter(ADVIA 120Siemens®).
Statisticalanalysis
For the variables Hb and Ht, the technique of analysis of variancewasused,inamodelofrepeatedmeasurementsin independentgroups,complementedbytheBonferroni multi-plecomparisonstest.20
Intheevaluationsontherangeofmotion,verbalpainscale and functioning,thenonparametric modelanalysisof vari-ancemodelofrepeatedmeasurementsinindependentgroups wasused,complementedbytheDunnmultiplecomparisons test.21
Results
Table2–Meanandminimumandmaximumvaluesfor age,sexdistributionanddurationofsurgeryamongthe patients.
PRPgroup Controlgroup Total
Numberofpatients 20 20 40
Age(years) 66.4(50–86) 71.6(55–81) 67.7
Sex(M/F) 6/14 8/12 14/26
Durationofsurgery (min)
90.7(80–105) 84.3(70–95) 86.8(70–105)
Transfusion 0 0 0
Table3–Plateletcountsbeforetheoperationandinthe PRPpreparation.
Plateletcounts Serum
plateletassay
Plateletassay onPRP
Patient1PRPgroup 316,000 950,000
Patient6PRPgroup 411,000 1,138,000
Patient11PRPgroup 223,000 777,000
Patient16PRPgroup 416,000 1,088,000
Intheplatelet counts,it wasfoundthat inthe casesof poorestyieldofplatelets,the numberwas twicethe initial quantitypresentinthe plasmaofthatpatient. Therewere somepatientsforwhomtheplateletcountafterthesecond centrifugationwasfourtimesasgreat(Table3).
Noneofthepatientsinthisstudyneededtohave trans-fusions. The criterion for transfusion used here was a
hemoglobin concentration of less than 7mg/dL in symp-tomaticpatientsduringthepostoperativeperiod.Therewere three patients who presented dehiscence of the operative woundandsuperficialinfection.Thesepatientsweretreated using dressings and oral antibiotics, and full healing was achievedinthesecases.TwoofthemwereinthePRPgroup. Therewerenocasesofthromboembolism.
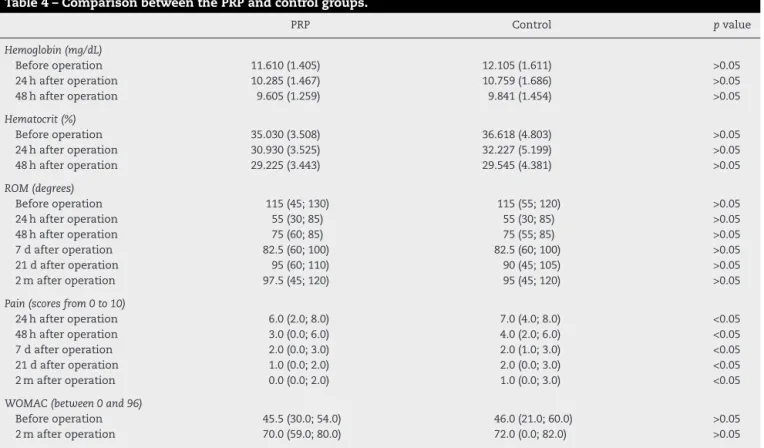
Table4showsthattherewerenostatisticallysignificant differences betweenthe groupswithregardto thepre and postoperativevaluesforthevariablesofhemoglobin, hema-tocrit,rangeofmotionorWOMACquestionnairescore.19In
thepainassessment,therewasasignificantadvantageinthe groupthatusedPRP.
Discussion
Variations in the ways of obtaining, preparing and apply-ingPRPcurrentlyconstitutealimitationonanycomparison betweenstudies.22ArecentsystematicreviewonPRPusein
chondrallesionsconsulted254citationsand,afterapplying rigorousexclusioncriteria,selected21forstudy.Evenso,10% ofthese didnot reportthe methodused forobtaining the PRPand28.6%didnotreporttheplateletconcentrationofthe preparation.23
In another study that evaluatesthis common variation betweenPRPpreparations,bloodsampleswerecollectedfrom eachoftheeightpatientsandtheseweresubjectedtothree differentcentrifugationmethods.Allofthesemethods con-siderablyincreasedthenumberofplateletsintheconcentrate,
Table4–ComparisonbetweenthePRPandcontrolgroups.
PRP Control pvalue
Hemoglobin(mg/dL)
Beforeoperation 11.610(1.405) 12.105(1.611) >0.05
24hafteroperation 10.285(1.467) 10.759(1.686) >0.05
48hafteroperation 9.605(1.259) 9.841(1.454) >0.05
Hematocrit(%)
Beforeoperation 35.030(3.508) 36.618(4.803) >0.05
24hafteroperation 30.930(3.525) 32.227(5.199) >0.05
48hafteroperation 29.225(3.443) 29.545(4.381) >0.05
ROM(degrees)
Beforeoperation 115(45;130) 115(55;120) >0.05
24hafteroperation 55(30;85) 55(30;85) >0.05
48hafteroperation 75(60;85) 75(55;85) >0.05
7dafteroperation 82.5(60;100) 82.5(60;100) >0.05
21dafteroperation 95(60;110) 90(45;105) >0.05
2mafteroperation 97.5(45;120) 95(45;120) >0.05
Pain(scoresfrom0to10)
24hafteroperation 6.0(2.0;8.0) 7.0(4.0;8.0) <0.05
48hafteroperation 3.0(0.0;6.0) 4.0(2.0;6.0) <0.05
7dafteroperation 2.0(0.0;3.0) 2.0(1.0;3.0) <0.05
21dafteroperation 1.0(0.0;2.0) 2.0(0.0;3.0) <0.05
2mafteroperation 0.0(0.0;2.0) 1.0(0.0;3.0) <0.05
WOMAC(between0and96)
Beforeoperation 45.5(30.0;54.0) 46.0(21.0;60.0) >0.05
2mafteroperation 70.0(59.0;80.0) 72.0(0.0;82.0) >0.05
butit wasseenthattherewasvariationinthe growth fac-torconcentrationsbetweenindividualsandbetweendifferent samplesfromthesameindividual.24
The PRP preparation in this study followed techniques thathadpreviouslybeendescribed.25,26Theplateletcounting
proved that high concentrations were produced (between twoandfour timesthelevel intheplasma).Inaddition to the plateletconcentrations, the typesofPRP canbe differ-entiated according to the concentration ofleukocytes and their formofactivation.22 In the present study,the
leuko-cyteswereseparatedfromthePRPthatwasobtained,andwe choseendogenousplateletactivation,i.e.donebymeansof thecollagenandother activationfactors ofthejoint cavity that was exposed.27 All the previous studies on
applica-tion ofPRP in casesofknee arthroplasty presented (when documented)platelet concentrations similar tothose used inthe presentstudy withleukocyte separation.1–3,17,18,28In
thesestudies,thePRP wasactivatedusingcalcified throm-bin,priortoapplication.Endogenousactivationbymeansof collagen shows a cytokine release pattern of longer dura-tion, of a more sustained nature than that of exogenous activation27 andforthisreason,itwasdoneinthepresent
study.Inthenaturalhealingprocess,the collagenexposed inthewoundedtissueisfrequentlytheinitialactivatorand generatesplateletadhesioninasinglelayeroveritself. Sub-sequently, there is superposition ofplatelets by means of the thrombin route. This manner, which is closer to the natural method of delayed activation, is functionally use-ful forensuring that growth factor release does not occur prematurely,i.e.beforecomplete formationofaprovisional scaffold.27
In2009,inthefirstrandomizedcontrolledstudyontheuse ofPRPincasesofkneearthroplastythatwaspublished,no benefitswereshown.18ThePRPusedwasactivatedbeforeits
applicationintheformofaspray,andthebleedingwas quan-tifiedthroughthedifferenceinhemoglobinvaluesfrombefore theoperationto24haftertheoperation.Asreportedearlier, endogenous activation may have ledto betterresults and, asconfirmedinthepresentstudy,therewasalsoanotable declineinhemoglobinandhematocritlevelsbetween24and 48haftertheoperation.
Inanother randomizedstudy inwhichPRP was usedin casesoftotalkneearthroplastywiththeaimofreducingthe bleeding,itsusedidnotmakeasignificantdifference,even thoughtherewasapositivedifferenceinrelationtothe post-operative bleeding.17 One of the possible reasons for this,
accordingtotheauthorsofthatstudy,wasthattheiruseof drainageaftertheoperationmighthaveledtolossofPRP.17
Forthisreason,wechosenottousedrainageinthepresent study.Nonetheless,wedidnotfindanystatistically signifi-cantresultsinrelationtobleeding.Anotherreasonthatwas pointedoutasapossiblecause oflackofstatistical signifi-canceintheresultsfromthatstudywasthesmallnumber ofpatients,whichmayhavebeenthesamelimitationasin thepresentstudy.Thisstudyalsoshowedthatthepainlevel waslower inthe groupthat usedPRP inthe postoperative evaluation.17
Inourstudy,the analysison pain,asshownbythe ver-bal pain scale, also showed that the group that used PRP had an advantage. This advantage,which was not shown
in the other variables analyzed, led to lower use of mor-phineinthisgroupduringthehospitalstay(onlyonepatient usedit,versusthreeinthecontrolgroup).Twomonthsafter the operation, another analysis on pain using the verbal scale stillshowedthatthe painlevelinthePRP groupwas better, althoughthis was provenin the pain and function questionnaire(WOMAC).Ithadalreadybeendocumentedin apreviousuncontrolledstudythatPRPhadapositiveeffect withregardtoimprovementofpostoperativepain.3PRPhas
a provenanti-inflammatoryeffectand hasbeen usedwith this functioninrelationto otherpathological conditions.29
This,therefore,mayexplaintheresultsfoundinthepresent study.
Despite the pain controlproveninthis and other stud-ies,anotherrecentlypublishedretrospectivestudyontheuse of PRP inrelationto knee prostheses,with morethan 200 patientsandwithouttheuseofpostoperativedrainsalsodid notshowanyimprovementinbleeding.28Inthepresentstudy,
thebleedingwasmeasuredthroughthedeclineinhemoglobin levels,only24haftertheoperation.
IntwopatientsinthePRPgroupandinonlyoneinthe con-trolgroup,therewasdehiscenceofthesutureandsuperficial infection.Thus,wedidnotfindanyevidenceinrelationto anyantibacterialeffect15oranyadvantageinrelationto
heal-ingoftheoperativewound.Apreviousstudy demonstrated bacterialgrowthinPRP.30 Preparationofthis,outsideofthe
laminarflowhood,asdoneinthepresentstudy,mayfacilitate contamination.
Thelimitationsofthepresentstudyincludethesmall num-berofpatients,whichmayhaveinterferedwiththeresultfrom the statistical analysis. Another factor relates to the study design,whichallowedthesurgeontobeawareofthegroup towhichthepatientbelonged,atthetimeofperformingthe operation.Thelackofquantificationofthegrowthfactorsand thenumberofresidualleukocytesinthePRPsamplesisalso afactorthatmayhavelimitedthediscussionoftheresults obtained.
Conclusion
InthemannerinwhichPRPwasused,itwasnotshownto beeffectiveforreducingthebleedingorimprovingthe func-tioningofthekneeafterarthroplasty,incomparisonwiththe controls.Therewasanadvantageontheverbalscalefor post-operativepain.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
Appendix
1.
Free
and
informed
consent
statement.
Thisstudyhasthetitle“Platelet-richplasma(PRP)applied duringtotalkneearthroplasty”.
Dr.JoãoPauloFernandesGuerreiro,adoctorwithinthe clinicalstaffofIrmandadedaSantaCasadeLondrina,will conductaclinicalstudywithinthisinstitutionthat involvestotalkneearthroplastyon40patients,usinga currentlywell-establishedsurgicaltechnique.In20 patients,wewillapplyplatelet-richplasma(PRP)before closingthewound.PRPisasubstancemadefromasample ofthepatient’sownblood,collectedatthetimeofstarting theanesthesia.
Theobjectiveofthestudyistoanalyzethebenefitsthat PRPmightbringtowardcontrollingpainandbleedingand improvinghealing.
PRPisapartofhumanbloodthatcontainsalargequantity ofplatelets.Plateletsarecellsthatparticipateinblood coagulationwhenbloodcomesintocontactwithwounds. ThePRPusedinthisstudywillberemovedfromthesame patientduringanesthesia.
Regardingtherisksofthesurgery,theseincludeedema (swelling),bleeding(withpossiblebloodtransfusionduring oraftertheoperation)and/orhematoma;dehiscenceof thesurgicalwound(breakageofstitchesoropeningorthe surgicalwound);postoperativepain;jointstiffness (movementlimitation);anestheticaccidents;complex regionalpainsyndrome;venousthrombosisandits consequences(formationofacoagulumthatcauses obstructionoftheveins);temporaryordefinitivefunctional incapacity(inrelationtoactivitiesofdailyliving,work activities,sportsorotheractivities);superficialinfection; deepinfectionanditsconsequences(difficulttotreatand eradicate,withtheneedfornewhospitalizationsand surgicalinterventionsforcleaningandremovaloffixation materials,andprobablesequelaesuchasfunctional limitationorlossofthelimboperated);neurovascular injuries(injuriestonervesthatmaycompromisethe sensitivityandmovementofagivenregionofthebody and/orlimb;arteriallesionsthatmaycompromisethe bloodirrigationofagivenregionand/orlimb). Themeantimetakentoperformthesurgeryis 100minutes.
Evaluationswillbemadebymeansofphysical
examinationsduringthehospitalstay(generallyfortwo daysafterthesurgery)andthenatthefollowingtimes afterthesurgery:7,10and21days;2,6and12months; andannuallythereafter.Radiographsofthekneewillbe performed2,6and12monthsafterthesurgeryand annuallythereafter,inthesamewayasisdoneroutinely amongourpatients.
Duringthepostoperativeperiod,itiscommontohave somedegreeofpain,butthisimproveswiththemedication thatwillbeprescribed.Theremaybesomeswellingofthe knee,whichcanbetreatedwithmedicationsandice compresses.Slightbleedingmayalsooccuronthefirst days.Anyotherdoubtshouldbeclarifiedwiththedoctor.
1.1.Therefore,werequestyourconsenttoincludeyouinour studyandweassureyouthanconfidentialitywillbemaintained. Wewillmakeuseofyourparticipationforthescientific
evaluationandpossiblepublicationofthisstudy,withinthe ethicalprinciplesthatmustguideresearchandourprofession. Wewouldalsoliketomakeitclearthatyourparticipation willnotimplyanyfinancialremuneration.Ifyourdonot wishtoparticipate,youarefreetooptout,bothatthe outsetorduringthecourseofthework,withoutany personallosses.
Ifyouhaveanyqueries,youcancontacttheresearcher directlythroughthistelephonenumber:(43)33770900.In anemergency,youcanseekassistanceattheorthopedic emergencyserviceofSantaCasadeLondrina,telephone: (43)33731671.
Youmayalsocontactthebioethicsandresearchethics committeeofIrmandadedaSantaCasadeLondrina, telephone:(43)33731643.
Wethankyouforyourvaluablecontribution.
Researcher’ssignature
IdeclarethatIhavebeeninformedaboutthestudyandI agreetoparticipate.
DATE:
Name
Signature
Appendix
2.
Western
Ontario
and
McMaster
Universities
Index
(WOMAC)
Category1–Severityofthepain(duringthelastmonth)in relationto:
Walking:()none()mild()moderate()severe Goingupstairs:()none()mild()moderate()severe Painatnight:()none()mild()moderate()severe Painwhenresting()none()mild()moderate()severe Whencarryingweights:()none()mild()moderate()severe Morningstiffness:()none()mild()moderate()severe Protokineticstiffness:()none()mild()moderate()severe
Category2–Levelofdifficultyincarryingoutthefollowing functions:
Goingdownstairs:()none()mild()moderate()severe Goingupstairs:()none()mild()moderate()severe Gettingupfromachair:()none()mild()moderate()severe Standingup:()none()mild()moderate()severe
Bendingtotheground:()none()mild()moderate()severe Walkingonalevelsurface:()none()mild()moderate()
severe
Shopping:()none()mild()moderate()severe Puttingsockson:()none()mild()moderate()severe Gettingoutofbed:()none()mild()moderate()severe Takingsocksoff:()none()mild()moderate()severe Lyingdownonabed:()none()mild()moderate()severe Gettingintoandoutofabath:()none()mild()moderate()
severe
Sittingdown:()none()mild()moderate()severe Sittingdownonandgettingupfromthetoilet: ()none()mild()moderate()severe
Carryingoutlightdomestictasks: ()none()mild()moderate()severe Carryingoutheavydomestictasks: ()none()mild()moderate()severe
Countingthepointsandcalculatingthescore:
Response“none”–4points;“mild”–3;“moderate”–2;and “severe”–0.
Totalnumberofpoints:
r
e
f
e
r
e
n
c
e
s
1. GardnerMJ,DemetrakopoulosD,KlepchickPR,MooarPA.The efficacyofautologousplateletgelinpaincontrolandblood lossintotalkneearthroplasty.Ananalysisofthe
haemoglobin,narcoticrequirementandrangeofmotion.Int Orthop.2007;31(3):309–13.
2. EvertsPA,DevileeRJ,BrownMahoneyC,
Eeftinck-SchattenkerkM,BoxHA,KnapeJT,etal.Plateletgel andfibrinsealantreduceallogeneicbloodtransfusionsin totalkneearthroplasty.ActaAnaesthesiolScand. 2006;50(5):593–9.
3. BerghoffWJ,PietrzakWS,RhodesRD.Platelet-richplasma applicationduringclosurefollowingtotalkneearthroplasty. Orthopedics.2006;29(7):590–8.
4. BoscoJA3rd,SloverJD,HaasJP.Perioperativestrategiesfor decreasinginfection:acomprehensiveevidence-based approach.JBoneJointSurgAm.2010;92(1):232–9. 5. BirkmeyerJD,GoodnoughLT,AuBuchonJP,NoordsijPG,
LittenbergB.Thecost-effectivenessofpreoperative autologousblooddonationfortotalhipandknee replacement.Transfusion.1993;33(7):544–51.
6. EtchasonJ,PetzL,KeelerE,CalhounL,KleinmanS,SniderC, etal.Thecosteffectivenessofpreoperativeautologousblood donations.NEnglJMed.1995;332(11):719–24.
7. HersekliMA,AkpinarS,OzkocG,OzalayM,UysalM,CesurN, etal.Thetimingoftourniquetreleaseanditsinfluenceon bloodlossaftertotalkneearthroplasty.IntOrthop. 2004;28(3):138–41.
8. JornLP,LindstrandA,Toksvig-LarsenS.Tourniquetreleasefor hemostasisincreasesbleeding.Arandomizedstudyof77 kneereplacements.ActaOrthopScand.1999;70(3):265–7. 9. ChristodoulouAG,PloumisAL,TerzidisIP,ChantzidisP,
MetsovitisSR,NikiforosDG.Theroleoftimingoftourniquet releaseandcementingonperioperativebloodlossintotal kneereplacement.Knee.2004;11(4):313–7.
10.MatrasH.Effectofvariousfibrinpreparationson reimplantationsintheratskin.OsterrZStomatol. 1970;67(9):338–59.
11.GibbleJW,NessPM.Fibringlue:theperfectoperativesealant? Transfusion.1990;30(8):741–7.
12.DohanEhrenfestDM,RasmussonL,AlbrektssonT.
Classificationofplateletconcentrates:frompureplatelet-rich
plasma(P-PRP)toleucocyte-andplatelet-richfibrin(L-PRF). TrendsBiotechnol.2009;27(3):158–67.
13.LevyO,MartinowitzU,OranA,TauberC,HoroszowskiH.The useoffibrintissueadhesivetoreducebloodlossandtheneed forbloodtransfusionaftertotalkneearthroplasty.A
prospective,randomized,multicenterstudy.JBoneJointSurg Am.1999;81(11):1580–8.
14.WhitmanDH,BerryRL,GreenDM.Plateletgel:anautologous alternativetofibringluewithapplicationsinoraland maxillofacialsurgery.JOralMaxillofacSurg.
1997;55(11):1294–9.
15.SánchezM,AnituaE,OriveG,MujikaI,AndiaI.Platelet-rich therapiesinthetreatmentoforthopaedicsportinjuries. SportsMed.2009;39(5):345–54.
16.MooarPA,GardnerMJ,KlepchickPR,MooarPA.Theefficacyof autologousplateletgelintotalkneearthroplasty:ananalysis ofrangeofmotion,hemoblobin,andnarcoticrequirements. In:67thAnnualMeeting.AmericanAcademyofOrthopaedic Surgeons.2000.p.PE148.
17.HorstmannWG,SlappendelR,vanHellemondtGG,Wymenga AW,JackN,EvertsPA.Autologousplateletgelintotalknee arthroplasty:aprospectiverandomizedstudy.KneeSurg SportsTraumatolArthrosc.2011;19(1):115–21.
18.PeerboomsJC,deWolfGS,ColarisJW,BruijnDJ,VerhaarJA. Nopositiveeffectofautologousplateletgelaftertotalknee arthroplasty.ActaOrthop.2009;80(5):557–62.
19.FernandesMI[dissertac¸ão]Traduc¸ãoevalidac¸ãodo questionáriodequalidadedevidaespecíficopara
osteoartroseWomac(WesternOntarioMcMasterUniversities) paraalínguaportuguesa.SãoPaulo:UniversidadeFederalde SãoPaulo,EscolaPaulistadeMedicina;2003.Availablefrom: http://www.biblioteca.epm.br/
20.JohnsonRA,WichernDW.Appliedmultivariatestatistical analysis.6thed.NewJersey:Prentice-Hall;2007.
21.ZarJA.Biostatisticalanalysis.5thed.NewJersey: Prentice-Hall;2009.
22.DeLongJM,RussellRP,MazzoccaAD.Platelet-richplasma:the PAWclassificationsystem.Arthroscopy.2012;28(7):998–1009. 23.SmythNA,MurawskiCD,FortierLA,ColeBJ,KennedyJG.
Platelet-richplasmainthepathologicprocessesofcartilage: reviewofbasicscienceevidence.Arthroscopy.
2013;29(8):1399–409.
24.MazzoccaAD,McCarthyMB,ChowaniecDM,CoteMP,Romeo AA,BradleyJP,etal.Platelet-richplasmadiffersaccordingto preparationmethodandhumanvariability.JBoneJointSurg Am.2012;94(4):308–16.
25.MarxRE.Platelet-richplasma:evidencetosupportitsuse.J OralMaxillofacSurg.2004;62(4):489–96.
26.WeibrichG,KleisWK.CurasanPRPkitvs.PCCSPRPsystem. Collectionefficiencyandplateletcountsoftwodifferent methodsforthepreparationofplatelet-richplasma.ClinOral ImplantsRes.2002;13(4):437–43.
27.HarrisonS,VavkenP,KevyS,JacobsonM,ZurakowskiD, MurrayMM.Plateletactivationbycollagenprovidessustained releaseofanaboliccytokines.AmJSportsMed.
2011;39(4):729–34.
28.DiiorioTM,BurkholderJD,GoodRP,ParviziJ,SharkeyPF. Platelet-richplasmadoesnotreducebloodlossorpainor improverangeofmotionafterTKA.ClinOrthopRelatRes. 2012;470(1):138–43.
29.KhoshbinA,LerouxT,WassersteinD,MarksP,
TheodoropoulosJ,Ogilvie-HarrisD,etal.Theefficacyof platelet-richplasmainthetreatmentofsymptomaticknee osteoarthritis:asystematicreviewwithquantitative synthesis.Arthroscopy.2013;29(12):2037–48.