w w w . r b o . o r g . b r
Original
Article
Amputation
after
failure
or
complication
of
total
knee
arthroplasty:
prevalence,
etiology
and
functional
outcomes
夽
,
夽夽
Alan
de
Paula
Mozella
a,∗,
Idemar
Monteiro
da
Palma
a,
Alberto
Ferreira
de
Souza
b,
Guilherme
Ornellas
Gouget
b,
Hugo
Alexandre
de
Araújo
Barros
Cobra
caOrthopedistattheKneeSurgeryCenter,InstitutoNacionaldeTraumatologiaeOrtopedia,RiodeJaneiro,RJ,Brazil
bResidentPhysician(R3)inOrthopedicsandTraumatologyatInstitutoNacionaldeTraumatologiaeOrtopedia,RiodeJaneiro,RJ,Brazil
cOrthopedistandHeadoftheKneeSurgeryCenter,InstitutoNacionaldeTraumatologiaeOrtopedia,RiodeJaneiro,RJ,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received21May2012 Accepted3July2012
Keywords:
Postoperativecomplications Amputation
Arthroplastykneereplacement
a
b
s
t
r
a
c
t
Objective:Identify theetiologyand incidence,as welltoassess functionaloutcomesof patients,undergoinglower limbamputationafterfailureor complication oftotalknee arthroplasty.ThesepatientsweretreatedattheCenterforKneeSurgeryattheNational InstituteofTraumatologyandOrthopedics(INTO),during theperiod ofJanuary2001to December2010.
Methods:Thepatientswereinterviewedandtheirchartswereretrospectivelyanalyzedto evaluatetheirfunctionaloutcome.
Results:Theincidenceofamputationduetofailureorcomplicationoftotalknee arthro-plastywas0.41%in2409cases.Recurrentdeepinfectionwasthecauseofamputationin81% ofcases,beingStaphylococcusaureusandPseudomonasaeruginosathemostfrequentgerms. Vascularcomplicationsandperiprostheticfractureassociatedtometaphysealboneloss werealsocausesofamputation.Inourstudy,44%ofamputeespatientswereusingorthesis and62.5%havehadtheabilitytowalk.
Conclusion:Incidenceof0.41%,beingthemaincauserecurrentinfection.Thefunctional outcomeislimited,andthefittingachievedin44%ofpatientsandonly62.5%areambulatory. ©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
Pleasecitethisarticleas:dePaulaMozellaA,daPalmaIM,deSouzaAF,GougetGO,deAraújoBarrosCobraHA.Amputac¸ãoapósfalha oucomplicac¸ãodeartroplastiatotaldejoelho:incidência,etiologiaeresultadosfuncionais.RevBrasOrtop.2013;48:406–411.
夽夽
StudyconductedattheKneeSurgeryCenter,InstitutoNacionaldeTraumatologiaeOrtopedia,RiodeJaneiro,RJ,Brazil.
∗ Correspondingauthorat:PraiadoFlamengo,66,BlocoB,Sala1313,RiodeJaneiro,RJ,Brazil.CEP22210-030.
E-mail:[email protected](A.d.P.Mozella).
2255-4971/$–seefrontmatter©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
Amputac¸ão
após
falha
ou
complicac¸ão
de
artroplastia
total
de
joelho:
incidência,
etiologia
e
resultados
funcionais
Palavras-chave:
Complicac¸õespós-operatórias Amputac¸ão
Artroplastiadojoelho
r
e
s
u
m
o
Objetivo: Identificar aetiologia e aincidência da amputac¸ãodomembroinferiorapós falhaoucomplicac¸ãodaartroplastiatotaldejoelhoeavaliarosresultadosfuncionaisdos pacientestratadospeloCentrodeCirurgiadeJoelhodoInstitutoNacionaldeTraumatologia eOrtopedia(Into)entrejaneirode2001edezembrode2010.
Métodos: Osprontuários foramretrospectivamente analisadosparacoletados dadose entrevistaparaavaliac¸ãodoresultadofuncional.
Resultados: A incidênciade amputac¸ãoem decorrência de falhaou complicac¸ãoapós 2.409artroplastiastotaisdejoelhofoide0.41%.Infecc¸ãoprofundarecorrentefoicausade amputac¸ãoem81%doscasos.OsgermesmaisfrequentesforamStaphylococcusaureuse Pseu-domonasaeruginosa.Complicac¸õesvascularesefraturaperiprotéticaassociadaaperdaóssea metafisáriarepresentaramindicac¸ãoemmenornúmerodecasos.Emnossoestudo,44% dospacientesamputadosapresentam–seprotetizadose62.5%apresentavamcapacidade dedeambulac¸ão.
Conclusões: Incidênciade 0.41%eprincipalcausainfecc¸ãorecorrente.Oresultado fun-cionalélimitado,aprotetizac¸ãofoialcanc¸adaem44%dospacientesesomente62.5%são deambuladores.
©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Theconceptofimprovingjointfunctionthroughmodification ofitssurfacewasproposed byVerneuil1 in1860,bymeans ofinterpositionofsofttissuesforjointreconstruction.Inthis procedure,despitepainreductionandincreasedmobility,the jointstability achievedwas unsatisfactoryand gaverise to impairedfunctionalresults.
Today, total knee arthroplasty (TKA) is an effective
option, with a high success rate in treating cases of
advanceddestructionofthisjointcausedbyprimaryor sec-ondary osteoarthrosis. It provides considerable pain relief,
correction of deformities and improvement of limb
func-tion, and consequently better quality of life for these
patients.2,3
In medium and long-term clinical evaluations, several
authorshavedemonstratedgoodorexcellentresultsinmore than90%oftheirpatientswhoreceivedkneeprostheses.4–6In otherstudies,thedegreeofsatisfactionreportedbypatients hasbeenanalyzed,andthesereportshavecorroboratedthe satisfactorydata,withgoodorexcellentresultsinaround90% ofthepatients.7–9
Inseveralcentersaroundtheworld,thedurabilityofthese
implants withmaintenanceofjointadequate function has
beenshowntobegreaterthan92%,13–15yearsaftertheinitial surgery.8–12
Because of the satisfactory results, the increased life
expectancyamongthe populationandthebetterqualityof
lifethat issought, the numbers ofTKA procedures is cur-rentlyincreasing.In2002,intheUnitedStates,therewasa 5%increaseinthenumberofTKAsperformedinrelationto thepreviousyears.13Kurtzetal.14estimatedthatbytheyear
2030,thenumberofprimaryTKAprocedures performedin
thatcountrywouldincreaseby670%.
Insomecases,afterseveralyearsofdurabilityand ade-quatefunctioning,arthroplastymaypresentfailure.Insuch cases,revisionsurgerybecomesnecessary,and satisfactory clinicalresultsareoftenobtained.15,16Inothercases, arthro-plastymaypresentfailureorcomplicationsthataredifficult todealwith.
Recurrentinfectionatprosthesissites,cutaneousor vas-cular complications and significant loss ofbone stock are challenging problems that are difficult tosolve and which sometimes haveunsatisfactory results.In thesesituations,
arthrodesis and resection arthroplasty are management
optionsforlimbsalvage.However,insomecases,the
treat-ment may be unsuccessful and these patients become
candidatesforlimbamputation.
Materials
and
methods
The aims of this study were to identify the etiology and
incidenceoflower-limbamputationafterfailureofor com-plicationsfrom TKA,and toevaluatethe functionalresults
among patients treatedat the KneeSurgery Center of the
National Institute ofTraumatology and Orthopedics(INTO)
betweenJanuary2001andDecember2010.
Thisstudywassubmittedforevaluationandapprovalby theResearchEthicsCommitteeofINTOandwasconductedat theKneeSurgeryCenterofthisinstitution.
Thepatients includedinthis study underwent
amputa-tion ofall or partofalower limbconsequent tofailure or complicationsafterconventionalprimaryTKA.Patientswho underwentamputationduetofailureoforcomplicationsfrom surgicalproceduresotherthankneeprosthesisimplantation wereexcluded.
The medical files were retrospectively analyzed in
arthroplasty, datewhenarthroplasty was performed,
dura-bility of the implant, surgical risk (ASA), postoperative
complications,TKAfailuremechanism,number of
reopera-tionsandtreatmentsforcomplicationsandtheamputation level.
The total number ofknee arthroplasty procedures
per-formedovertheperiodwasobtainedfromthecomputerized recordsofINTO.
Toevaluatethefunctionalresults,thepatientswere inter-viewedandwereaskedwhethertheywereusingaprosthesis,
whether theywere capableofwalking,what distancethey
were abletowalk andwhether someformofsupportwas
neededforwalking.
Results
Between January 2001 and December 2010, 2409 TKA
pro-cedures were performed. Among these cases, 10 patients
underwentamputationduetofailureorcomplications relat-ingtotheprosthesis,andthustheincidencepresentedwas 0.41%.
Overthecourseofthisperiod,atotalof16amputations
were performed atINTO asa consequenceoffailure ofor
complications from TKA. However,some of thesepatients
wereexcludedfromtheincidencecalculation,giventhatfour
amputationswereperformedonpatientswhohadundergone
primaryTKAatotherservicesandtwocaseshadreceivedthe primaryprosthesisbeforethestudyperiodstarted(Fig.1).
Amputation wasperformed on eightmale patients and
eightfemalepatients.Thepatients’meanageatthetimeof thisprocedurewas67.1years,witharangefrom53to80years. In11cases,therightkneewasoperatedandinfivecases,the
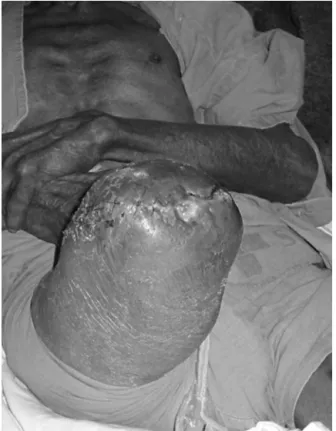
Fig.1–PatientamputatedduetoinfectionafterTKA.
leftknee.Primarygonarthrosiswastheindicationfora pros-thesisintenofthesepatients(62.5%),rheumatoidarthritisin three(18.75%)andpost-traumaticarthrosisinthree(18.75%). Inthisseries,intwocasestheamputationwasperformed
onpatientswhohadundergonerevisionofprimarysurgery
andpresentedimplantswithamajordegreeofconstriction ofnails.In14patients,thecomplicationsorfailuresoccurred beforeexchangingtheprostheticcomponents.In10patients,
arthrodesiswas performedas alimbsalvage measure, but
withunsatisfactoryresults.
Themeantimethatelapsedbetweentheprimary arthro-plastyandtheamputationwasapproximately4.5years,with arangefromonedayto12years.Themeanlengthof follow-upaftertheamputationwas6.7years,witharangefromtwo tonineyears.
Inaccordancewiththeanestheticriskcriteriaofthe Amer-icanSocietyofAnesthesiology(ASA),87.5%wereclassifiedas ASAIIand6.25%asASAIII,while6.25%didnotpresentany clinicalcomorbidities(ASAI).
Recurrentdeepinfection wasidentifiedasthemain
eti-ology for amputation following TKA. This occurred in 13
cases, which represented 81% of the sample. Acute
arte-rial occlusionwasidentifiedasthe causeofamputationin twocases(12.5%)andperiprostheticfractureassociatedwith metaphyseal bone loss (type III inthe classificationof the
Anderson OrthopedicResearch Institute, AORI)occurred in
onecase(6.5%).Theinfectionwasdiagnosedafter osteosyn-thesis(Table1).
Extensiveskinnecrosiswasobservedintwocases. How-ever, inboth ofthem this complication occurred after the
infectiousconditionhadbeenproven.Amyocutaneousflap
wasneededinthecasesofbothpatients.
Inthepatientswhounderwentamputationdueto recur-rent infection,culturespresentedgrowth ofmorethanone bacterialagentin38%ofthecases.
ThemostprevalentgermwasStaphylococcusaureus,which wasidentifiedin54%ofthecultures.Methicillin-resistantS. aureuswasisolatedin31%.Methicillin-sensitiveS.aureus pre-sentedgrowthin23%ofthepatients.Pseudomonasaeruginosa wasidentifiedin38%oftheculturesandin31%itwas asso-ciatedwithanotherbacterialspecies.Acinetobacterbaumanii andKlebsiellapneumoniaewereidentifiedintwocases(15%), butwerenotverifiedasasingleagent.Serratiamarsenswas notedintwopatients(15%)andinoneasasingleinfectious agent.Proteusmirabiliswasnotedinonecaseofpolymicrobial infection(7.5%).
Themeannumberofsurgicalprocedurespriorto
ampu-tation was 6.8. When only the patients who underwent
amputationduetoinfectionwere takenintoconsideration, thenumberofpreviousproceduresrangedfrom3to22,with ameanof7.6.
Allofthepatientsunderwenttransfemoralamputation.In onecase,whichwasofvascularetiology,anamputationat tar-sometatarsaljointlevelwasinitiallyperformed,butbecause offailureinattemptstoperformthromboembolectomy,itwas necessarytoraisetheleveloftheamputation.Intwocases,it wasnecessarytoreviseandraisetheboneresectionbecause ofaninfectiousconditionintheamputationstump.
Over the course of the functional evaluations, three
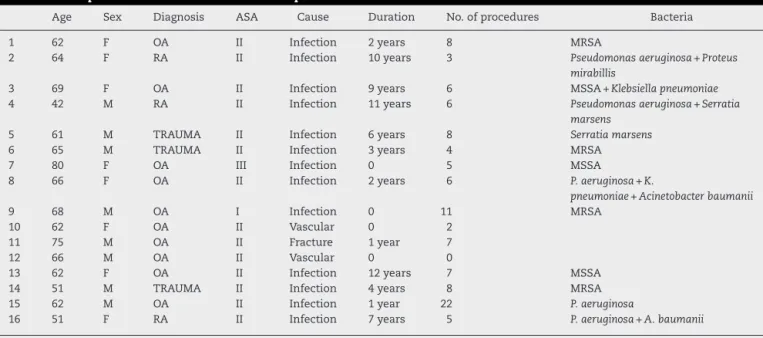
Table1–AmputationsduetofailureoforcomplicationsfromTKA.
Age Sex Diagnosis ASA Cause Duration No.ofprocedures Bacteria
1 62 F OA II Infection 2years 8 MRSA
2 64 F RA II Infection 10years 3 Pseudomonasaeruginosa+Proteus
mirabillis
3 69 F OA II Infection 9years 6 MSSA+Klebsiellapneumoniae
4 42 M RA II Infection 11years 6 Pseudomonasaeruginosa+Serratia
marsens
5 61 M TRAUMA II Infection 6years 8 Serratiamarsens
6 65 M TRAUMA II Infection 3years 4 MRSA
7 80 F OA III Infection 0 5 MSSA
8 66 F OA II Infection 2years 6 P.aeruginosa+K.
pneumoniae+Acinetobacterbaumanii
9 68 M OA I Infection 0 11 MRSA
10 62 F OA II Vascular 0 2
11 75 M OA II Fracture 1year 7
12 66 M OA II Vascular 0 0
13 62 F OA II Infection 12years 7 MSSA
14 51 M TRAUMA II Infection 4years 8 MRSA
15 62 M OA II Infection 1year 22 P.aeruginosa
16 51 F RA II Infection 7years 5 P.aeruginosa+A.baumanii
F,female;M,male;OA,osteoarthrosis;RA,rheumatoidarthritis;MRSA,methicillin-resistantStaphylococcusaureus.
datawereobtainedfromthelastfollow-upconsultation ana-lyzed.
Amongthe16patientswhounderwentamputation,only sevenwerefittedwithprostheses(44%).Allofthese individ-ualsweresaidtobeabletowalk,althoughwiththeexception ofonepatient, all ofthem requiredaids suchas apair of crutchesorawalkingframe.Twopatientswhohadbeenfitted withprosthesessaidthattheircapacitytowalkwaslimitedto theirhomes,whiletheotherfivesaidthattheywerecapable ofwalkingfordistancesgreaterthanablock(Table2).
Amongtheninepatientswhowerenotfittedwith
pros-theses (56%), six were incapable ofwalking and remained
restrictedtoawheelchair.Onepatientsaidthathewasableto walkaroundhishomewithhelp.Anothertwopatientswere capableofwalkingwithhelpfordistancesgreaterthanablock. Wedidnotidentify anystatistical relationship between age,thediagnosisthatcausedthefailureandmotivatedthe arthroplasty,andthefunctionalresultsfromfittingthe pros-thesisorfromwalking.
Discussion
Many differentstudies intheliteraturehavedealtwiththe maincomplicationthatcanoccurafterTKA.However,there arefewdataontheincidenceofamputationsduetofailures oforcomplicationsfromkneeprostheses.Outofmorethan 9000kneeprostheses assessed,Randet al.16described two cases(0.02%)ofinfrapatellaramputationrelatedtovascular insufficiency.
After performing 12,118 TKAs, Bengstonand Knutson17
studied357patientswhoevolvedwithdeepinfection.Inthis
sample,23patientshadtoundertransfemoralamputation.
Thus,theincidencefoundwas0.18%outofallthecasesand 6%whenonlytheinfectedarthroplastycasesweretakeninto consideration.Isiklaretal.10reportedanincidenceof0.18%, i.e.nineamputationsafter5045arthroplastyprocedures per-formed.InthestudybySierraetal.15on25patients,thecause oftheamputationwasrelatedtoprostheticreplacementof theknee,whichcorrespondedtoaprevalenceof0.14%.
Table2–Functionalresult.
Prosthesisuse Walking Aid Distance
1 No No:limitedtowheelchair
2 No No:limitedtowheelchair
3 No No:limitedtowheelchair
4 Yes Yes 2crutches >1block
5 Yes Yes 2crutches >1block
6 Yes Yes 2crutches >1block
7 No No:limitedtowheelchair
8 Yes Yes 2crutches >1block
9 Yes Yes No >1block
10 Yes Yes 2crutches Athome
11 No No:limitedtowheelchair
12 No No:limitedtowheelchair
13 Yes Yes Walkingframe Athome
14 No Yes 2crutches >1block
15 No Yes Walkingframe Athome
Inourseries,theincidencewas0.41%,i.e.10amputations after2409arthroplastyprocedures.However,wehaddifficulty inidentifyingamputationsamongourpatientsthattookplace atotherhealthcareunits,eitherasacomplicationfromTKA orduetounrelatedcauses.
InthestudybyIsiklaretal.,10deepinfectionwasidentified insevenoftheeightcasesofamputation.Datapresentedby Sierraetal.15identifiedinfectionasthemaincauseof amputa-tionafterTKA,whichoccurredin74%ofthepatients.Infection wasthemaincauseofamputationidentifiedinourseriesand occurredin81%ofthecases.
S.aureushasbeen thegerm mostfrequentlyisolated in postoperativeinfectionsinseveralinternationalcenters.18In eightcasesofamputationduetoinfection,Isiklaretal.10 iden-tifiedS.aureusinthreepatientsandS.epidermitisinfour.Our samplewasconcordantwiththereportsintheliterature:S. aureuswasisolatedin54%oftheculturesfrompatients ampu-tatedduetoinfection.
Cutaneouscomplicationssuchasextensivenecrosismay evolve withdeepinfection after TKAin uptoa quarterof thepatients,asreportedindifferentstudies.10,15Inourstudy, outofthe16patientswhounderwentamputation,twocases presentedcutaneousnecrosisafterdeepinfectionhadbeen diagnosed.
Vascular complications after knee arthroplasty are rare eventsandgenerallyhavecatastrophicresults.Smithetal.19 notedthattheprevalenceofcomplicationsduetovascular
causes wasbetween 0.03%and 0.17%.These usuallyoccur
inpatientswithpreviouslyundiagnosedatherosclerotic dis-easeand,amongthesecases,25–43%evolvewithamputation.
Inoursample,twopatientsneededamputationbecauseof
ischemiaofthelimbshortlyafteranarthroplastyprocedure. Periprostheticfracturing associatedwith bone loss that
compromisedthe metaphyseal bone(type III ofAORI
clas-sification) was identified as the initial event that led to
amputationin6.5%ofoursample(onecase).Weemphasize
thatinfectionofthesurgicalsitedevelopedaftertreatingthe fracture.InthestudybySierraetal.,15thiscauserepresented thelowestprevalenceofoccurrencesofamputationafterTKA. Thepatientsunderwentanaverageof6.8proceduresprior toamputation.Takingonlythecasesofinfection into
con-sideration, this mean roseto 7.6. However,the number of
previoussurgicalprocedurescouldbeashighas22,asfound inonecaseofinfectionfollowingTKA.Thesedatawere con-cordantwiththosepublishedbyIsiklaretal.10Nonetheless,
thesedataseemedhighincomparisonwiththemeanof2.8
proceduresprecedingamputationthatwas observedinthe
sampleofPringetal.20
Patientsundergoingtransfemoralamputationdueto com-plicationsfollowingarthroplasty presentlimited functional results,becauseofmultifactorialcauses.Inmostcases,these areelderlypatientswithmultiplejointinvolvementanda vari-etyofcomorbidities.Theenergyconsumptionforlocomotion ishigherthan innormalgait,and givesrise todifficulty in muscleandproprioceptiverehabilitation.
Inourstudy,44%oftheamputatedpatientswerefittedwith prostheses.ThisfindingisconcordantwiththestudybyPring etal.20However,itishigherthanwhatwaspresentedinthe seriesofSierraetal.,15whichdocumentedarateofonly20%, andthefindingsofIsiklaretal.,10whoreportedthat12.5%of
thepatientswerefittedwithaprosthesisafteramputation, followingTKA.
Pringetal.20 reportedthatonly30%ofthepatientswho underwentamputationwerecapableofwalkingregularly. Isik-laretal.10corroboratedthesedataandidentified35%oftheir sampleaswalkers.
Inourseries,62.5%ofthepatientsreportedthattheywere capableofwalking,althoughtheyneededanaid.Amongthe patients without aprosthesis, only33% reportedthat they were walkingregularly,whileinthegroupfittedwith pros-theses,allofthemwereclassifiedaswalkers.
Conclusions
Theincidenceofamputationconsequenttofailureor compli-cationsafter2409TKAprocedureswas0.41%.
The main cause of amputation was recurrent deep
infection, which occurred in 81% of the cases. Vascular
complications and periprosthetic fractures associatedwith metaphysealbonelosswerethecauseofamputationin12.5% and6.5%,respectively.
Onaverage,6.8surgicalprocedureswereperformedprior toamputation.
Thefunctionalresultwaslimited.Fittingofaprosthesis wasachievedin44%ofthepatients,and only62.5%ofthe patientswerecapableofwalking.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.VerneuilA.Delacréationd’unefaussearticulationpar sectionourésectionpartielledel’osmaxillaireinférieur, commemoyenderémedieral’ankylosevraieoufaussedela machoireinférieure.ArchGenMed.1860;15:174.
2.CoytePC,HawkerG,CroxfordR,WrightJG.Ratesofrevision kneereplacementinOntario,Canada.JBoneJointSurgAm. 1999;81(6):773–82.
3.SharkeyPF,HozackWJ,RothmanRH,ShastriS,JacobySM. InsallAwardpaper.Whyaretotalkneearthroplastiesfailing today?ClinOrthopRelatRes.2002;(404):7–13.
4.Font-RodriguezDE,ScuderiGR,InsallJN.Survivorshipof cementedtotalkneearthroplasty.ClinOrthopRelatRes. 1997;(345):79–86.
5.WeirDJ,MoranCG,PinderIM.Kinematiccondylartotalknee arthroplasty.14-yearsurvivorshipanalysisof208consecutive cases.JBoneJointSurgBr.1996;78(6):907–11.
6.RanawatCS,PadgettDE,OhashiY.Totalkneearthroplastyfor patientsyoungerthan55years.ClinOrthopRelatRes. 1989;(248):27–33.
7.ScuderiGR,InsallJN,WindsorRE,MoranMC.Survivorshipof cementedkneereplacements.JBoneJointSurgBr.
1989;71(5):798–803.
8.FehringTK,OdumS,GriffinWL,MasonJB,NadaudM.Early failuresintotalkneearthroplasty.ClinOrthopRelatRes. 2001;(392):315–8.
arthroplastyrevision.ClinOrthopRelatRes.2006;446: 45–50.
10.IsiklarZU,LandonGC,TullosHS.Amputationafterfailedtotal kneearthroplasty.ClinOrthopRelatRes.1994;(299):173–8. 11.IncavoSJ,WildJJ,CoughlinKM,BeynnonBD.Earlyrevisionfor
componentmalrotationintotalkneearthroplasty.Clin OrthopRelatRes.2007;458:131–6.
12.GioeTJ,KilleenKK,GrimmK,MehleS,ScheltemaK.Whyare totalkneereplacementsrevised?Analysisofearlyrevisionin acommunitykneeimplantregistry.ClinOrthopRelatRes. 2004;(428):100–6.
13.GonzalezMH,MekhailAO.Thefailedtotalkneearthroplasty: evaluationandetiology.JAmAcadOrthopSurg.
2004;12(6):436–46.
14.KurtzS,OngK,LauE,MowatF,HalpernM.Projectionsof primaryandrevisionhipandkneearthroplastyintheUnited Statesfrom2005to2030.JBoneJointSurgAm.
2007;89(4):780–5.
15.SierraRJ,TrousdaleRT,PagnanoMW.Above-the-knee amputationafteratotalkneereplacement:prevalence, etiology,andfunctionaloutcome.JBoneJointSurgAm. 2003;85(6):1000–4.
16.RandJA,PetersonLF,BryanRS,IlstrupDM.Revisiontotal kneearthroplasty.InstrCourseLect.1986;35:305–18. 17.BengtsonS,KnutsonK.Theinfectedkneearthroplasty.A
6-yearfollow-upof357cases.ActaOrthopScand. 1991;62(4):301–11.
18.FasciaDT,SinganayagamA,KeatingJF.Methicillin-resistant
Staphylococcusaureusinorthopaedictrauma:identificationof riskfactorsasastrategyforcontrolofinfection.JBoneJoint SurgBr.2009;91(2):249–52.
19.SmithDE,McGrawRW,TaylorDC,MasriBA.Arterial complicationsandtotalkneearthroplasty.JAmAcadOrthop Surg.2001;9(4):253–7.