w w w . r b o . o r g . b r
Update
article
Infection
after
total
knee
replacement:
diagnosis
and
treatment
夽
Lúcio
Honório
de
Carvalho
Júnior
a,∗,
Eduardo
Frois
Temponi
b,
Roger
Badet
caAssociateProfessorintheDepartmentoftheLocomotorSystem,SchoolofMedicine,UniversidadeFederaldeMinasGerais,
MemberoftheKneeGroup,HospitalMadreTeresa,BeloHorizonte,MG,Brazil
bMemberoftheKneeGroup,HospitalMadreTeresa,BeloHorizonte,MG,Brazil cBoneJointCenterforHealthandSports,BourgoinJallieu,France
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received19December2012 Accepted29January2013
Keywords:
Anti-bacterialagents
Arthroplasty,replacement,knee Debridement
Infection
a
b
s
t
r
a
c
t
Infectionaftertotalkneereplacement(IATJ)isararecomplication.Itisassociatedwith increased morbidity andmortality increasing thefinal costs. Gram positive coccusand
Staphylococcuscoagulase-negativeandStaphylococcusaureusarethemostcommonisolated germs(>50%ofthecases).Conditionsrelatedtothepatient,tothesurgicalprocedureand eventothepostophavebeenidentifiedasriskfactorstoIATJ.Manycomplementary meth-odstogetherwithclinicalsymptomsareusefultoaproperdiagnosis.TreatmentforIATJ mustbeindividualizedbutgenerallyisacombinationofsystemicantibiotictherapyand surgicaltreatment.Prosthesisexchangeinoneortwostagesisthefirstchoiceprocedure. Debridementwithprosthesisretentionisanoptioninacutecaseswithstableimplantsand antibioticsensiblegerms.
©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Infecc¸ão
em
artroplastia
total
de
joelho:
diagnóstico
e
tratamento
Palavras-chave:
Antibacterianos Artroplastiadojoelho Desbridamento Infecc¸ão
r
e
s
u
m
o
Infecc¸ãoapósartroplastiatotaldojoelho(IATJ)écomplicac¸ãoincomum.Estáassociadaa aumentodamorbimortalidadeedoscustosdeinternac¸ão.Cocosgram-positivos,sobretudo
Staphylococcuscoagulase-negativeeStaphylococcusaureus,sãoosgermesmaiscomumente iso-lados(>50%detodososcasos).Condic¸õesligadasaopaciente,aoprocedimentocirúrgicoe mesmoaopós-operatóriotêmsidoidentificadascomofatoresderiscoparaIATJ.Váriossão osmétodoscomplementaresquesesomamàinvestigac¸ãoclínicaparaodiagnóstico infec-ciosoemelhorcaracterizac¸ãodoquadro.OtratamentoparaaIATJdeveserindividualizado,
夽
StudyconductedattheHospitalMadreTeresa,BeloHorizonte,MG,Brazil.
∗ Correspondingauthorat:HospitalMadreTeresa,Av.RajaGabaglia1002,Gutierrez,BeloHorizonte,MGCEP30430-142,Brazil.
E-mail:[email protected],[email protected](L.H.deCarvalhoJúnior).
2255-4971/$–seefrontmatter©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
masgeralmenteenvolveacombinac¸ãodaantibioticoterapiasistêmicacomotratamento cirúrgico.Atrocadoimplanteemumoudoisestágioséoprocedimentodeescolha. Desbri-damentocomretenc¸ãodapróteseéopc¸ãoemcasosagudos,comimplantesestáveisecom germessensíveisaosagentesantimicrobianos.
©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Infectionaftertotalkneearthroplasty(TKA)isatopicofgreat interestfororthopedistsandinfectologists.Alternatives for diminishingthe TKAinfection ratehave longbeen sought, giventhat theseratescontinuetobebetween0.4%and2% afterprimaryarthroplastyandbetween3.2%and5.6%after revision arthroplasty.1–5 Long-termfollow-up has shown a
periprostheticinfectionrateof1.55%overthefirsttwoyears afterTKAand0.46%peryearafterthisperiod,untilthetenth year.6,7TKAisaprocedureperformedworldwide,with600,000
surgicalproceduresperyearintheUSAandameansurvival rateof95%over15years.8–10Kurtzetal.10predictedthatthere
wouldbeanincreaseinthedemandforTKAof673%by2030. AlthoughtheTKAinfectionratemayseemlow,thenumber ofsuchinjuriestendstoincreasewithincreasingnumbersof procedures.
Clinicalcomplicationsandincreasedcostsassociatedwith TKAinjurieshavebeenofgrowingconcern.Themortalityrate amongpatientsovertheageof65yearswhowereawaitinga surgicalprocedurefortreatingTKAinfectionhasrangedfrom 0.4%to1.2%,andbetween2%and7%amongpatientsaged over80years.11ThemeancostoftreatingTKAinfectionshas
beenestimatedas50,000dollarsperpatientand250million dollarsperyear,intheUnitedStates.12,13
The microorganisms most commonly encountered in TKAinfectionculturesarecoagulase-negativeStaphylococcus
(30–43%)andStaphylococcusaureus(12–23%),followedby con-tamination due to mixed flora (10%), Streptococcus (9–10%), Gram-negativebacilli(3–6%)andanaerobicbacilli(2–4%).No germisisolatedinaround11%ofthecases.14,15
Thisreviewhadtheaimofdiscussingthediagnosisand treatmentofpatientswithaconditionofTKAinfection.
Risk
and
prevention
factors
TKAinfectionhasbeencorrelatedwithanumberofrisk fac-tors: diabetes, malnutrition, smoking,use ofsteroids, poor controloveranticoagulation,obesity,cancer,alcoholism, uri-narytractinfections,multiplebloodtransfusionsandrevision surgery.Thecurrentguidanceisthatsuchfactorsshouldbe identifiedandmultidisciplinaryinterventionshouldbe imple-mented before performing any procedure, with the aimof gettingthepatientintoabettercondition.16
Use of antimicrobialprophylaxis, care in preparing the patient’sskinbeforetheoperationanduse oflaminarflow in surgical theaters have reduced the intraoperative con-taminationrates.Fortyyearsago,forevery10patientswho underwentTKA,onewoulddevelopinfection.17,18
Malinzaketal.19reportedthattheinfectionratewas0.51%
among8494hipandkneearthroplastyprocedures.Theyfound thattheriskfactorsforinfectionwereobesity,earlyageand diabetesmellitus.Patientswithbodymassindexgreaterthan 40 and those withdiabetes presenteda 3.3 and 3.1 times greaterchanceofTKAinfection,respectively.Glycemic con-trolhasbeenatopicgreatlydiscussed.Thebenefitsofrigorous control,bothbeforeandaftertheoperation,werereportedby Marchantetal.20andVandenBergheetal.21
Obesityisariskfactorandisalsocorrelatedwithwound complications, as demonstrated byWiniarsky et al.,22 ina
studyinwhich22%oftheobesegroupofpatientspresented infectionofthesurgicalwoundandhigherprevalenceofdeep infection.Obesityisnotnecessarilysynonymouswith nutri-tion,andevaluatingtransferrin,albuminandleukocyteshas beenimportantinthesecases.
Persistence of drainage during the postoperative period and woundcomplications are alsofactors associatedwith infection.Galatetal.23reportedthatthe infectionratewas
higherinthegroupofpatientsinwhomtherewashematoma formation. This was also reported by Parvizi et al.,24 who
indicatedthattheinfectionratewashigherincaseswith per-sistentdrainagethroughthesurgicalwoundandinpatients whopresentedRNI>1.5.
Clinical
presentation
and
diagnosis
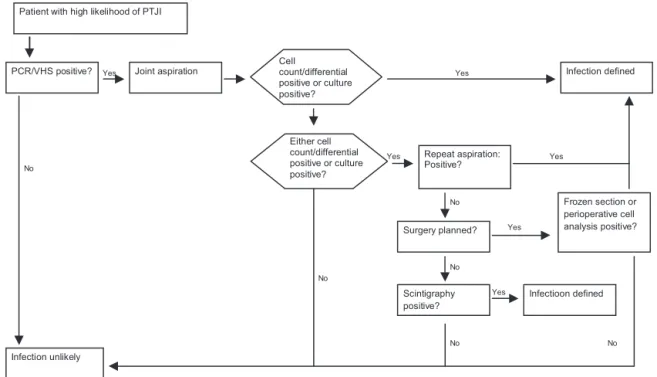
TheevaluationandmanagementofpatientswithTKA infec-tionshouldfollowalogical,clearandreproduciblesequence. The American Academy of Orthopedic Surgeons (AAOS) has developed clinical practice guidelines for this process (Figs.1–3).
TKAinfectionscanbetemporallydividedintothreetypes: acute(lessthanthreemonths),subacute(threeto24months) and chronic (>24 months).25,26 The time period analyzed
relatestothestartoftheinfectiousconditionandis impor-tant indetermining the treatment. The first two formsof presentation are linked to the surgical procedure and the last to bacteremia, generally relating to the skin, teeth or genitourinary tract.27 Acuteinfections are characterizedby
pain,edema,heat,erythemaandfever,commonlycausedby virulent germs suchasS.aureusand Gram-negativebacilli. Patientswithsubacuteconditions(coagulase-negative Staphy-lococcusandP.acnes)usuallyhavesignsandsymptomsthatare non-evidentandmaypresentpersistentpain,implant loos-eningorboth,whichmakesasepticlooseningadifferential diagnosis.14Thechronicconditionhasvariablepresentation,
High likelihood of infecon One or more symptoms, and at least one or more: 1) Risk factor OR
2) Clinical examinaon OR
3) Early loosening of an implant (detected on radiograph) Low likelihood of infecon Pain or joint sffness and none of the items below:
1) Risk factor OR 2) Clinical examinaon OR
3) Early loosening of an implant (detected on radiograph) Symptoms Risk factors - literature Risk factors
-consensus
Clinical examinaon
Others
1- Joint pain 2- Joint sffness
1- Previous joint infecon
2- Superficial infecon 3- Obesity
4- Duraon of surgery > 2.5 h
5- Immunosuppression
1- Recent bacteremia (< 1 year)
2- Metachronic infecon 3- Skin disorders 4- Drugs with
intravenous acon 5- Acve infecon
at other site 6- Recent
infecon or colonizaon by Staphylo MRSA (< 3 years)
1- Edema, reddening and heat 2- Fistula
associated with surgical site
1- Early loosening of implant (< 5 years), detected on radiograph
Fig.1–Stratificationoftheriskfactors.
Reproducedwithmodificationsfrom“Thediagnosisofperiprostheticjointinfectionsofthehipandknee.Guidelineand evidencereport”.AdoptedbytheAmericanAcademyofOrthopedicSurgeonsBoardofDirectors,June18,2010.American
AcademyofOrthopedicSurgeons,2010;18(12):760–770(withpermission).
highorlowlikelihoodofinfection,whichisimportantforthe subsequentpropaedeutics.
After clinical and temporal characterization, laboratory testsformpartoftheinvestigationofinfections.C-reactive
protein(CRP)levelsanderythrocytesedimentationrate(ESR) are evaluated in patients with suspected TKA infection. CarvalhoJunioretal.28demonstratedthatCRPandESRreturn
to levels lower than the preoperative levels in 30 and 80
Patient with high likelihood of PTJI
PCR/VHS positive? Joint aspiration
Cell count/differential positive or culture positive?
Infection defined Yes
Either cell count/differential positive or culture positive?
Yes
Yes Repeat aspiration: Positive?
Infection unlikely No
No
Surgery planned?
Scintigraphy positive?
Infectioon defined Yes
No No
No
Frozen section or perioperative cell analysis positive? Yes
Yes
No
Fig.2–AlgorithmformanagingpatientswithahighlikelihoodofinfectionfollowingTKA.
Patient with low likelihood of PTJI
PCR/VHS positive?
Joint aspiration
Cell
count/differential positive or culturepositive?
Infection defined
Yes
Either cell count/differential positive or culture positive?
Yes
Yes Repeat aspiration:
Positive?
Infection unlikely
No
No
Surgery planned?
Observe and reevaluate in 3 months
No
No Frozen section or
perioperative cell analysis positive?
Yes Yes
No
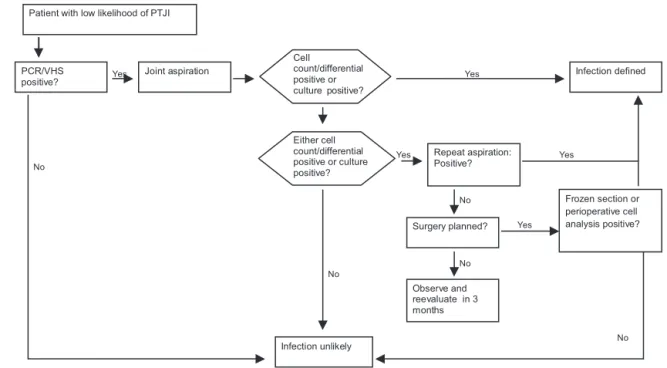
Fig.3–AlgorithmformanagingpatientswithalowlikelihoodofinfectionfollowingTKA.
Reproducedwithmodificationsfrom“Thediagnosisofperiprostheticjointinfectionsofthehipandknee.Guidelineand evidencereport”.AmericanAcademyofOrthopedicSurgeons,2010;18(12):760–770(withpermission).
days,respectively,afternon-complicatedTKA.Piperetal.29
reportedthatthecutoffvaluesforCRPandESRwere14.5mg/L and 19mm/h, respectively, for diagnosing TKA infection. Anotherimportantlaboratorytoolforthediagnosishasbeen interleukin6(IL-6).Arecentmeta-analysisshowedthatthe diagnosticaccuracywasbestusingIL-6 values,followedby CRP,ESRandleukocytecounts.30Othermarkers(alpha-1
gly-coproteinacidandprocalcitonin)haveemerged,althoughstill withoutapplicabilitywithinclinicalpractice.
Imagingexaminationscanalsobeusedtocomplementthe evaluation,butarenotessentialfordiagnosingtheinfection, nor dothey rule it out.Simple anteroposterior and lateral radiographsare useful when evaluated comparatively with previous images.31 Periosteal reactions, component
migra-tion and osteolysis are signs of possible involvement of infection.Bonescintigraphy,computedtomography,magnetic resonanceimagingand PETscansmay alsobeused, while respectingtheirindicationsandobjectives.Scintigraphyusing technetium-99mhashighsensitivitybutlittlespecificityfor infection,andmaygivefalsepositiveresultsforuptooneyear aftertheprimaryprocedure,becauseofboneremodeling.32
Usingleukocytesmarkedwithindium-111,accuracyof81% hasbeenachievedindiagnosingTKAinfection.33TheAAOS
hasrecommendedthattriphasicbonescintigraphyshouldbe usedincaseswithahighlikelihoodofTKAinfectionfollowing negativecultures.Tomographyallowsbettercontrastbetween normal and infected tissues, but the presence of artifacts causedbymetallimitsitsuse.Withtechnicalmodifications, magneticresonance imagingmaybeusefulformakingthe diagnosis,particularlyincasesinvolvingthefemoralimplant. PETscanshaveshownaccuracyof77.8%indiagnosing infec-tion,withsensitivityof90%andspecificityof89.3%.34–36In
theinvestigativeprocess,aspirationofsynovialfluidfromthe jointisimportant.Itshouldbeanalyzedinthelaboratoryto
quantifythetotalleukocytecountandthepercentof polymor-phonuclearleukocytes.Countsgreaterthan3000leukocytes per microliter withneutrophils countsof atleast 60% are considered to be the criteria for diagnosing subacute or chronicinfection.Culturingtheaspiratehastheobjectiveof identifyingthegermandestablishingitssensitivitypattern. UseofGramhasnotbeenindicatedbecauseofitslow sensi-tivityandspecificity.37–39Parvizietal.40demonstratedthatthe
colorimetrictestfordetectingleukocyteesteraseinthe syno-vialfluidishighlysensitiveandspecificfordiagnosingTKA infectionandalsohasthebenefitsofprovidingaresultintwo minutesandhavinglowcost.
Foracutecases,countsofmorethan27,800leukocytesper microliter have presentedpositive predictive valueof94%, whileothermarkershavenotbeenshowntobeusefulbecause ofthenormalinflammatoryresponseoftheimmediate post-operativeperiod.41
Theculturingshouldbedoneforaerobicgerms,anaerobic germsandfungi,whichsufficienttimeallowedforobserving thegrowthofallofthese.Culturesonfistulouspassagesor swabsdonothaveanyvalue.
Duringthesurgery,atleastthreesamplesshouldbe col-lectedfromdifferentlocationsandpreferablyafterstopping the use of antibiotics. Studies have shown sensitivity of 60% with classical laboratoryculturingtechniques. Sonica-tion techniqueshaveincreasedthesensitivityto83.3%.25,42
Incasesofnegativeculturesbeforeorduringtheoperation, histological analysis can be performed, with perioperative frozen-sectionbiopsyorrepetitionofjointpunctureafteran intervalofsixweeks.
Patient with low likelihood of PTJI
PCR/VHS positive?
Joint aspiration
Cell
count/differential positive or culturepositive?
Infection defined
Yes
Either cell count/differential positive or culture positive?
Yes
Yes Repeat aspiration:
Positive?
Infection unlikely
No
No
Surgery planned?
Observe and reevaluate in 3 months
No
No Frozen section or
perioperative cell analysis positive?
Yes Yes
No
Fig.4– Algorithmfortreatingacuteorsubacuteprostheticinfection.
Combiningtheclinicalhistory,laboratoryalterationsand cultureresultsguidesandenablesidentificationofthe infec-tiouscondition.Inaround5–10%ofthecases,alterationsmay existthroughoutthepropaedeutics,butwithoutconfirmation fromculturing.Berbarietal.43reportedthatitwasimportant
thatthetreatmentshouldbeguidedinaccordancewiththe entireinvestigation,andnotjusttheresultsfromculturing. Inevaluating897casesofperiprostheticinfection,theyfound that7%ofthecaseshadfalsenegativecultures.Allofthese casesunderwentsurgicalordrugtreatmentwithafive-year successrateofgreaterthan70%.
Treatment
Theprimaryobjective intreating TKAinfectionisto eradi-catetheinfection.Painreliefandreestablishmentoffunction aresecondaryobjectives,butnolessimportant.Throughthe influenceoftheAmericanliterature,debridementwith reten-tion (D+R)and replacementina singleprocedure (1T) are usedless frequently.Inaddition,temporaryplacementofa spacercontainingantibiotics,followedbyreplacementwith thedefinitiveimplant(2T)44–46andsuppressiontherapy(ST),
hasalsobeen proposed.Segawaet al.definedfour clinical phasesofTKAinfectionthatareusefulforguidingthe treat-ment:I–infectionidentifiedatthetimeoftheprocedure;II –acutepostoperativeinfection;III–identificationsomeyears aftertheoriginalprocedure,comingfromadistantfocus;IV– chronicinfection.
Thesurgicaltreatmentsthatexist incasesofinfectious conditionsareD+R,1T,2T,resectionarthroplasty,arthrodesis, amputationandST.44Thechoiceofbesttreatmentdependson
thepatient’scondition,theconditionoftheimplantandthe germthatwasisolated.
D+Risagoodalternativeforpatientswithearly postop-erativeinfectiousstatesand acutehematogenicconditions,
providedthatthedurationofsymptomsisnomorethanthree weeks,theskincoverageconditionsareadequate,theimplant is stable and an antimicrobial agent with effective action is available. It has been recommended that initial venous antibiotictherapyshouldbeusedfortwotofourweeks,with conversion to oral medication after this period.46,47 Byren
etal.48demonstratedthattheinfection-freesurvivalrateafter
D+Rtreatmentwas82%,withafollow-upof2.3years. Fail-ure was associatedwith arthroscopic treatment,infections inrevisionproceduresandinfectionduetoS.aureus.Trebse etal.49appliedaD+Rprotocoltoaseriesof24patientswith
an86%successrateoverthreeyearsanddefinedthatthe fac-torsforagoodprognosiswerethepresenceofastableimplant, absenceoffistulascontiguouswiththeprostheticcomponent anddurationofsymptomslessthanthreeweeks.
Replacementinasingleprocedureisagoodoptionwhen there is good skin coverage, absence of comorbidities and infectionnotcausedbymultiresistantgerms.Jämsenetal.50
reportedthattheinfectioneradicationratesrangedfrom73% to100%over122monthsoffollow-upusingthisstrategy.
If thesecriteriaare notall fulfilled,thebestoption isto replacetheimplantintwoprocedures(2T).Inthesecases,a mobileorrigidjointspacermadeofpolymethylmethacrylate (PMM)shouldbeused.Thishastheobjectivesofkeepingthe softtissuesundertension,diminishingthe“deadspace”and enablinglocalreleaseofantibiotic.51,52Inthesecases,
Zim-merlietal.46recommendedthatthesecondprocedureshould
beperformedafterasshortatimeaspossible(twotofour weeks),whichdiminishesthecostsandthedurationof hospi-talstay.Haleemetal.51reportedthatthesuccessrateoverfive
yearsoffollow-upwas93.5%andover10years,85%.Macheras etal.52reportedthattheinfection-freesurvivalratewas91.1%
over12.1yearsoffollow-up.
Intact or minimally compromised
Compromised Abscess or fistula
Agents that are difficult to treat MRSA, GNB, MR
Enterococcus
Fungi
Single-stage exchange Drainage prolonged antibiotic
Patient’s general condition or surgical risk Debilitated, bedridden and not in a condition for other surgery
Comorbidites Immunodepressed Without functional improvement (without mobility)
Two-stage exchange Long interval (6 to 8 weeks)
Drainage with spacer Prolonged antibiotic
Suppression treatment with antibiotic for prolonged period
Removal of prosthesis without replacement Drainage Prolonged antibiotic
Two-stage exchange Long interval (2 to 4 weeks) Drainage with spacer Prolonged antibio_c Condition of
soft tissues
Modifying situations
Surgery
Removal of prosthesis
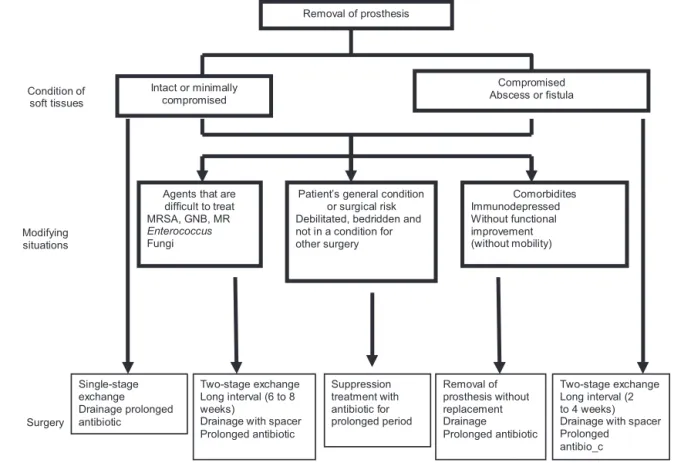
Fig.5–Algorithmfortreatinginfectionthatisnotqualifiedfordebridement+retention.
use)mightfunctionassitesforbacterialfixation(through for-mationofbiofilm),thereisnoconsensusregardingtheideal lengthoftimeforthespacertobekeptinuse.DellaValle53
suggestedthattheminimumtimeshouldbeeightweeks, pro-videdthataftertheendoftheinitialantibiotictherapy(six weeks),thevaluesfrominflammatorytestscontinuetoshow progressivereductionsoverthesubsequenttwoweeks.
Anotherpointthatisstillunderdiscussionisthemixture ofantibioticswiththePMManditsconcentration. Thereis nostandardizationofthequantityused.Empirically,10%of itsweighthasbeen used,whichrepresents4gofantibiotic foreach unit (40g).It is known that high doses of antibi-oticmayalterthe mechanicalpropertiesofthe spacerand makeiteasilybreakable.54Despitethis,Anagnostakosetal.55
reported that they used high doses of antibioticsin PMM, withoutmajorclinicalrepercussionsorsideeffects.Although manufacturedformulationsofPMMinassociationwith gen-tamicinandtobramycinexist,thedosageoftheseantibiotics inthemixturedoesnotreachthe10%mentionedabove.When theantibioticismixedinonthesurgicaltable,itispossible toaddtheantibiotictothemostexternallayerofthePMM andincreaseitsareaofcontactwiththebonesurface (place-mentasasurfacecoating).Thechoiceofantimicrobialagent dependsonthegermtobetreatedandthethermoresistance oftheagent, giventhatthe polymerization reactionofthe PMMwhenassociatedwithbariumisexothermic andmay interferewith the properties ofthe antibiotic. Gentamicin, tobramycin and vancomycin are good alternatives as ther-moresistantagents.56,57
In addition to surgical treatment, systemic antibiotic therapy should be maintained. It has been recommended that there should besix monthsof treatment forpatients with TKAinfection who present unfavorable skin coverage conditions.45,46 Theantimicrobialagentshould have
bacte-ricidal action, even against slow-growth germs or biofilm producers.Beforestartinganytreatment,thesusceptibilityof thegermshouldbetestedandalternativeregimensshouldbe discussed,giventhegrowinglevelsofresistance.57,58A
com-binationofrifampicinwithquinoloneshasbeenusedmost often,withgoodresultsinvitro,invivoandinclinicaltrials. Options such as linezolid, sulfamethoxazole-trimethoprim andminocyclinearepossible,althoughsofarnoclinical stud-ies forvalidating their use havebeen published. The best optionistodiscussthebestantimicrobialtherapyforeach casewiththehospitalinfectioncontrolcommittee.58,59
Ifthepatientisnotinasuitableclinicalconditionforthe newprocedure,STwithlong-durationantimicrobial medica-tion becomesthe bestoption. Inthese cases,the objective becomesoneofcontrollingtheacutemanifestations,rather than eradication ofthe infection.Arthrodesisand amputa-tion are options forimmunocompromisedpatients andfor those forwhom newarthroplastywould notimprove their function.59
UsingtheAAOSandZimmerlirecommendationsdescribed inFigs.4and5, Giulierietal.60 reportedthatthecurerate
was83%,whileTrampuzetal.,61Tsukayamaetal.,62Meehan
etal.63andBetschetal.64observedcureratesof90%,91%,89%
thoseoftheothersbecausetheyhadagreaternumberof2T procedures,withagreaternumberofcasesofadvances dis-easeormicroorganismsofgreatervirulence.Theriskfactors fortherapeuticfailureweredescribedaspolymicrobial infec-tionandinfectionduetoGram-negativebacilli,mycobacteria andfungi.
With better comprehension of the pathogenesis of the disease and developmentofnew diagnostic and investiga-tivetechniques,better treatmentand managementofTKA infection will be achieved, with fewer complications and morbidity–mortality.
Final
remarks
AfterTKAinfectionhasbeendiagnosed,itstreatmentshould beindividualizedbutgenerallyinvolvesacombinationof sys-temicantibiotictherapywithsurgicaltreatment.Replacement oftheimplantinoneortwostagesisthepreferredprocedure. Debridementwithretentionoftheprosthesisisanoptionin acutecasesthathavestableimplantsandpresentgermsthat aresensitivetotheantimicrobialagents.
Conflicts
of
interest
Theauthorsdeclarethattherewerenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. MahomedNN,BarrettJ,KatzJN,BaronJA,WrightJ,LosinaE. EpidemiologyoftotalkneereplacementintheUnitedStates Medicarepopulation.JBoneJointSurgAm.2005;87:1222–8. 2. WilsonMG,KelleyK,ThornhillTS.Infectionasa
complicationoftotalknee-replacementarthroplasty.Risk factorsandtreatmentinsixty-sevencases.JBoneJointSurg Am.1990;72:878–83.
3. WindsorRE,BonoJV.Infectedtotalkneereplacements.JAm AcadOrthopSurg.1994;2:44–53.
4. HanssenAD,RandJA.Evaluationandtreatmentofinfection atthesiteofatotalhiporkneearthroplasty.InstrCourse Lect.1999;48:111–22.
5. BozicKJ,KurtzSM,LauE,OngK,ChiuV,VailTP,etal.The epidemiologyofrevisiontotalkneearthroplastyintheUnited States.ClinOrthopRelatRes.2010;468:45–51.
6. KurtzSM,OngKL,LauE,BozicKJ,BerryD,ParviziJ.Prosthetic jointinfectionriskafterTKAinthemedicarepopulation.Clin OrthopRelatRes.2010;468:52–6.
7. BerbariEF,HanssenAD,DuffyMC,SteckelbergJM,IlstrupDM, HarmsenWS,etal.Riskfactorsforprostheticjointinfection: case–controlstudy.ClinInfectDis.1998;27:1247–54.
8. RanawatCS,FlynnJrWF,SaddlerS,HansrajKK,MaynardMJ. Long-termresultsofthetotalcondylarkneearthroplasty.A 15-yearsurvivorshipstudy.ClinOrthopRelatRes.
1993;286:94–102.
9. RitterMA,BerendME,MedingJB,KeatingEM,FarisPM,Crites BM.Long-termfollowupofanatomicgraduatedcomponents posteriorcruciate-retainingtotalkneereplacement.Clin OrthopRelatRes.2001;388:51–7.
10.KurtzSM,LauE,SchmierJ,OngKL,ZhaoK,ParviziJ.Infection burdenforhipandkneearthroplastyintheUnitedStates.J Arthroplasty.2008;23:984–91.
11.FismanDN,ReillyDT,KarchmerAW,GoldieSJ.Clinical effectivenessandcost-effectivenessof2management
strategiesforinfectedtotalhiparthroplastyintheelderly. ClinInfectDis.2001;32:419–30.
12.MastersonEL,MasriBA,DuncanCP.Treatmentofinfectionat thesiteoftotalhipreplacement.InstrCourseLect.
1998;47:297–306.
13.SculcoTP.Theeconomicimpactofinfectedjointarthroplasty. Orthopedics.1995;18:871–3.
14.SteckelbergJM,OsmonDR.Prostheticjointinfections.In: WaldvogelFA,BisnoAL,editors.Infectionsassociatedwith indwellingmedicaldevices.3rded.Washington:American SocietyforMicrobiology;2000.p.173–209.
15.SegawaH,TsukayamaDT,KyleRF,BeckerDA,GustiloRB. Infectionaftertotalkneearthroplasty.Aretrospectivestudy ofthetreatmentofeighty-oneinfections.JBoneJointSurg Am.1999;81:1434–45.
16.ShirtliffME,MaderJT.Acutesepticarthritis.ClinMicrobiol Rev.2002;15:527–44.
17.NIHconsensusconference:totalhipreplacement.NIH consensusdevelopmentpanelontotalhipreplacement. JAMA.1995;273:1950–6.
18.LidgrenL.Jointprostheticinfections:asuccessstory.Acta OrthopScand.2001;72:553–6.
19.MalinzakRA,RitterMA,BerendME,MedingJB,OlberdingEM, DavisKE.Morbidlyobese,diabetic,younger,andunilateral jointarthroplastypatientshaveelevatedtotaljoint arthroplastyinfectionrates.JArthroplasty.2009;24Suppl. 6:84–8.
20.MarchantJrMH,ViensNA,CookC,VailTP,BolognesiMP.The impactofglycemiccontrolanddiabetesmellituson perioperativeoutcomesaftertotaljointarthroplasty.JBone JointSurgAm.2009;91:1621–9.
21.VandenBergheG,WoutersP,WeekersF,VerwaestC, BruyninckxF,SchetzM,etal.Intensiveinsulintherapyin criticallyillpatients.NEnglJMed.2001;345:1359–67. 22.WiniarskyR,BarthP,LotkeP.Totalkneearthroplastyin
morbidlyobesepatients.JBoneJointSurgAm.1998;80:1770–4. 23.GalatDD,McGovernSC,LarsonDR,HarringtonJR,Hanssen
AD,ClarkeHD.Surgicaltreatmentofearlywound complicationsfollowingprimarytotalkneearthroplasty.J BoneJointSurgAm.2009;91:48–54.
24.ParviziJ,GhanemE,JoshiA,SharkeyPF,HozackWJ,Rothman RH.Doesexcessiveanticoagulationpredisposeto
periprostheticinfection?JArthroplasty.2007;22Suppl.2:24–8. 25.TrampuzA,WidmerAF.Infectionsassociatedwith
orthopedicimplants.CurrOpinInfectDis.2006;19:349–56. 26.SchafrothM,ZimmerliW,BrunazziM,OchsnerPE.Infections.
In:OchsnerPE,editor.Totalhipreplacement.Berlin: Springer-Verlag;2003.p.65–90.
27.MaderazoEG,JudsonS,PasternakH.Lateinfectionsoftotal jointprostheses.Areviewandrecommendationsfor prevention.ClinOrthopRelatRes.1988;229: 131–42.
28.CarvalhoJuniorLH,SantosRL,Mendonc¸aCJA,CamposCT, AndradeMAP.Avaliac¸ãodavariac¸ãodatemperaturacutânea, proteínaCreativaevelocidadedehemossedimentac¸ãona artroplastiatotaldojoelhoprimária,isentadecomplicac¸ões. ActaOrtopBras.2006;14:161–4.
29.PiperKE,Fernandez-SampedroM,SteckelbergKE,Mandrekar JN,KarauMJ,SteckelbergJM,etal.C-reactiveprotein, erythrocytesedimentationrateandorthopedicimplant infection.PLoSOne.2010;5:e9358.
30.BerbariE,MabryT,TsarasG,SpangehlM,ErwinPJ,Murad MH,etal.Inflammatorybloodlaboratorylevelsasmarkersof prostheticjointinfection:asystematicreviewand
meta-analysis.JBoneJointSurgAm.2010;92:2102–9. 31.TiggesS,StilesRG,RobersonJR.Appearanceofseptichip
32.SmithSL,WastieML,ForsterI.Radionuclidebone scintigraphyinthedetectionofsignificantcomplications aftertotalkneejointreplacement.ClinRadiol.2001;56: 221–4.
33.HainSF,O’DohertyMJ,SmithMA.Functionalimagingandthe orthopaedicsurgeon.JBoneJointSurgBr.2002;84:
315–21.
34.ZhuangH,DuartePS,PourdehnadM,MaesA,VanAckerF, ShnierD,etal.Thepromisingroleof18F-FDGPETin detectinginfectedlowerlimbprosthesisimplants.JNucl Med.2001;42:44–8.
35.Ivan´cevi´cV,PerkaC,HasartO,SandrockD,MunzDL.Imaging oflow-gradeboneinfectionwithatechnetium-99mlabelled monoclonalanti-NCA-90Fab’fragmentinpatientswith previousjointsurgery.EurJNuclMedMolImaging. 2002;29:547–51.Erratumin:EurJNuclMedMolImaging 2002;29(6):835.
36.LarikkaMJ,AhonenAK,JunilaJA,NiemeläO,Hämäläinen MM,SyrjäläHP.Improvedmethodfordetectingknee replacementinfectionsbasedonextendedcombined 99mTc-whitebloodcell/boneimaging.NuclMedCommun. 2001;22:1145–50.
37.GhanemE,ParviziJ,BurnettRS,SharkeyPF,KeshavarziN, AggarwalA,etal.Cellcountanddifferentialofaspiratedfluid inthediagnosisofinfectionatthesiteoftotalknee
arthroplasty.JBoneJointSurgAm.2008;90:1637–43. 38.SchinskyMF,DellaValleCJ,SporerSM,PaproskyWG.
Perioperativetestingforjointinfectioninpatients
undergoingrevisiontotalhiparthroplasty.JBoneJointSurg Am.2008;90:1869–75.
39.DuffGP,LachiewiczPF,KelleySS.Aspirationofthekneejoint beforerevisionarthroplasty.ClinOrthopRelatRes.
1996;331:132–9.
40.ParviziJ,JacovidesC,AntociV,GhanemE.Diagnosisof periprostheticjointinfection:theutilityofasimpleyet unappreciatedenzyme.JBoneJointSurgAm.2011;93: 2242–8.
41.BedairH,TingN,JacovidesC,SaxenaA,MoricM,ParviziJ, etal.TheMarkCoventryAward:diagnosisofearly postoperativeTKAinfectionusingsynovialfluidanalysis. ClinOrthopRelatRes.2011;469:34–40.
42.HolinkaJ,BauerL,HirschlAM,GraningerW,WindhagerR, PresterlE.Sonicationculturesofexplantedcomponentsasan add-ontesttoroutinelyconductedmicrobiological
diagnosticsimprovepathogendetection.JOrthopRes. 2011;29:617–22.
43.BerbariEF,MarculescuC,SiaI,LahrBD,HanssenAD, SteckelbergJM,etal.Culture-negativeprostheticjoint infection.ClinInfectDis.2007;1–45:1113–9.
44.WestrichGH,SalvatiEA,BrauseB.Postoperativeinfection.In: BonoJV,McCartyJC,ThornhillTS,BierbaumBE,TurnerRH, editors.Revisiontotalhiparthroplasty.NewYork:
Springer-Verlag;1999.p.371–90.
45.LanglaisF.Canweimprovetheresultsofrevision
arthroplastyforinfectedtotalhipreplacement?JBoneJoint SurgBr.2003;85:637–40.
46.ZimmerliW,TrampuzA,OchsnerPE.Prosthetic-joint infections.NEnglJMed.2004;14–351:1645–54.
47.ZimmerliW,WidmerAF,BlatterM,FreiR,OchsnerPE.Roleof rifampinfortreatmentoforthopedicimplant-related staphylococcalinfections:arandomizedcontrolledtrial. Foreign-BodyInfection(FBI)StudyGroup.JAMA. 1998;20–279:1537–41.
48.ByrenI,BejonP,AtkinsBL,AngusB,MastersS,
McLardy-SmithP,etal.Onehundredandtwelveinfected arthroplastiestreatedwithDair(debridement,antibiotics, andimplantretention):antibioticdurationandoutcome.J AntimicrobChemother.2009;63:1264–71.
49.TrebseR,PisotV,TrampuzA.Treatmentofinfectedretained implants.JBoneJointSurgBr.2005;87:249–56.
50.JämsenE,StogiannidisI,MalmivaaraA,PajamäkiJ,Puolakka T,KonttinenYT.Outcomeofprosthesisexchangeforinfected kneearthroplasty:theeffectoftreatmentapproach.Acta Orthop.2009;80:67–77.
51.HaleemAA,BerryDJ,HanssenAD.Mid-termtolong-term followupoftwo-stagereimplantationforinfectedtotalknee arthroplasty.ClinOrthopRelatRes.2004;428:35–9.
52.MacherasGA,KaterosK,GalanakosSP,KoutsostathisSD, KontouE,PapadakisSA.Thelong-termresultsofatwo-stage protocolforrevisionofaninfectedtotalkneereplacement.J BoneJointSurgBr.2011;93:1487–92.
53.DellaValleCJ.Comunicac¸ãoPessoal.In:14◦Congresso
BrasileirodeCirurgiadoJoelho.2012.
54.KelmJ,RegitzT,SchmittE,JungW,AnagnostakosK.Invivo andinvitrostudiesofantibioticreleasefromandbacterial growthinhibitionbyantibiotic-impregnated
polymethylmethacrylatehipspacers.AntimicrobAgents Chemother.2006;50:332–5.
55.AnagnostakosK,WilmesP,SchmittE,KelmJ.Elutionof gentamicinandvancomycinfrompolymethylmethacrylate beadsandhipspacersinvivo.ActaOrthop.2009;80:193–7. 56.SpringerBD,LeeGC,OsmonD,HaidukewychGJ,HanssenAD,
JacofskyDJ.Systemicsafetyofhigh-doseantibiotic-loaded cementspacersafterresectionofaninfectedtotalknee arthroplasty.ClinOrthopRelatRes.2004;427:47–51. 57.AnderlJN,ZahllerJ,RoeF,StewartPS.Roleofnutrient
limitationandstationary-phaseexistenceinKlebsiella pneumoniaebiofilmresistancetoampicillinand
ciprofloxacin.AntimicrobAgentsChemother.2003;47:1251–6. 58.SchwankS,RajacicZ,ZimmerliW,BlaserJ.Impactof
bacterialbiofilmformationoninvitroandinvivoactivitiesof antibiotics.AntimicrobAgentsChemother.1998;42:895–8. 59.OsmonDR,BerbariEF.Outpatientintravenousantimicrobial
therapyforthepracticingorthopaedicsurgeon.ClinOrthop RelatRes.2002;403:80–6.
60.GiulieriSG,GraberP,OchsnerPE,ZimmerliW.Management ofinfectionassociatedwithtotalhiparthroplastyaccording toatreatmentalgorithm.Infection.2004;32:222–8.Erratum in:Infection.2004;32(5):309.
61.TrampuzA,CattelanC,FlückigerU,FreiR,ZimmerliW. Treatmentoutcomeofprostheticjointinfection:tenyear cohortstudy(1994–2003)[abstractK-883].In:Programand abstractsofthe45thinterscienceconferenceon
antimicrobialagentsandchemotherapy.Washington: AmericanSocietyforMicrobiology;2005.p.47.
62.TsukayamaDT,EstradaR,GustiloRB.Infectionaftertotalhip arthroplasty.Astudyofthetreatmentofonehundredandsix infections.JBoneJointSurgAm.1996;78:512–23.
63.MeehanAM,OsmonDR,DuffyMC,HanssenAD,KeatingMR. Outcomeofpenicillin-susceptiblestreptococcalprosthetic jointinfectiontreatedwithdebridementandretentionofthe prosthesis.ClinInfectDis.2003;1–36:845–9.