Original Article
A CORROSION CAST STUDY OF RAM IFICATION PATTERN OF
PORTAL VEIN IN RIGHT LOBE OF HUM AN LIVER
Rajput AS *
1, Kumari S
2, M ishra GP
3.
ABSTRACT
Address for Correspondence: Dr. Ajay Singh Rajput , Assistant Professor, Depart ment of Anat omy, RIM S, Bareilly, Uttar Pradesh, India. 301, Eldeco Emperor, New Hyderabad, Lucknow, UP, India 226007. Phone : +918418995515 E-M ail: drasrajput [email protected]
Access this Article online
Quick Response code Web site:
* 1 Assistant Professor, Depart ment of Anat omy, RIM S, Bareilly, Uttar Pradesh, India.
2 Assistant Professor, Depart ment of Forensic M edicine & Toxicology, M ayo Inst it ute of M edical Sciences, Barabanki, Ut t ar Pradesh, India.
3 Associate Professor, Depart ment of Anat omy, Career Inst it ute of M edical Sciences and Hospitals, Ghaila, Lucknow, Uttar Pradesh, India.
Objectives: The aim of t he st udy w as t o know t he int rahepat ic ram ificat ion pat t ern of port al vein in right lobe of liver & it s var iat ions.
M et hods: 25 hum an fresh livers w ere obt ained aft er aut opsy and st udied by corrosion cast m et hod. Polym eric granules of but yl but yrat e w ere dissolved in acet one and 20% hom ogenous solut ion w as m ade. Solut ion w as inject ed int o port al vein and t he inject ed liver w as placed in 10 % form al saline for 24 hours at room t em perat ure (20°C) f or polym erizat ion of inf used but yl but yrat e solut ion. M acerat ion of liver t issue achieved by w hole-organ im m ersion in 1.8 N KOH solut ion at 68°C for 24 hrs. Each cast t hus obtained w as preserved in glycerin and det ails w ere st udied.
Results:The lengt h of t he right port al vein varies 0.5 t o 1.8 cm (1.2 cm ). The right port al vein bif urcat ed int o second order branches - right ant erior port al vein (RAPV) & right post erior port al vein (RPPV) in 87 % of t he cases, w hile t rif urcat ed in rest of 13 % of cases. The angle bet w een t he ant erior and post erior division ranged from 58°-95 °. Ant erio-superior (P8) branch show n t hree t ype of ram ificat ion - Bif urcat ion t ype (72 %), P8- one pedicle t ype (8 %) and P8- t rifurcat ion t ype (20%). Ant erio-infer ior (P5 m ax ) br anch show n t he t hree t ype of ram ificat ion pat t ern - P5 -com m on t ype (72 %), P5 – P8 ant erior t ype (28 %) but P5 – P8 post er ior t ype w as not observed. Right Posterior Portal Vein has shown t hree types of ram ification patt ern - Type I-Fan shaped (64%),Type II (28 %) & Type III-Trifurcat ion t ype (8%).
Conclusions: The findings of present st udy on hepat ic vasculat ur e have im m ense im port ance in t he field of hepat o-biliar y sur geries like hepat ic resect ion, segm ent ect om y and liver t ransplant at ion.
KEY W ORDS: Liver, Corrosion cast , Portal vein, Ram ificat ion, Right lobe.
INTRODUCTION
Int ernat ional Journal of Anatomy and Research, Int J Anat Res 2014, Vol 2(4):791-96. ISSN 2321- 4287 DOI: 10.16965/ ijar.2014.551
Received: 30 Nov 2014
Peer Review : 30 Nov 2014 Published (O):31 Dec 2014 Accept ed: 13 Dec 2014 Published (P):31 Dec 2014 Internat ional Journal of Anat omy and Research
ISSN 2321-4287 w w w.ijmhr.org/ ijar.ht m
DOI: 10.16965/ ijar.2014.551
Liver is t he largest viscera in human body & it is essent ial for life, since it carries out most of met abolic funct ion necessary for homeost asis, digest ion and imm unit y. Recent ly it s vascular anat omy has gained even great er significance
Int J Anat Res 2014, 2(4):791-96. ISSN 2321-4287 it . M any aut hors [1-5] proposed liver segment al division but t he division proposed by Couinaud (1954)[1] w as w idely recognized. According t o Couinaud (1954)[1]t he liver is divided int o right & left lobes, lobe int o sect ors & sect ors furt her int o segments based on t hird order ramificat ion of port al vein and it s drainage.He report ed t hat port al vein branching appears first during t he em bryonic developm ent , w hile art eriobiliary branching follow s t he port al vein dist ribut ion. Also portal segmentation w as much simpler than t he art eriobiliary and port al vein duplicat ion of t he first -order branches found in 23.5% of liv-ers, w hile art erio-biliary duplicat ion of first -or-der branches is found in 50% , hence t o st udy t he port al vein ramificat ion yields bet t er ana-t omical sana-t udy of liver. Couinaud (1954) [1] de-scribed eight segment s. The right lobe of liver divided int o
-Ant erio-inferior (Segment V)
Ant erio-superior (Segment VIII)
Post erio-inferior (Segment VI)
Post erio-superior (Segment VII).
All t hese drained by right branch of hepat ic vein sit uat ed in right fissure.
Left lobe of liver divided int o
-Segment II (left lat eral)
Segment III (left paramedian)
Segment IV (left paramedian)
All t hese drained by left branch of hepat ic vein lying in left fissure.
Caudat e lobe : segment I – drained by middle hepat ic vein.
Each of t hese segm ent s has it s independent hepat ic venous drainage and t hird order branch of port al veins, w it h minimal anast omosis & a few var iat ions, m akes it s surgical resect ion possible. These segm ent s form t he basis of hepat ic resect ion as defined in t he var ious h ep at ic sur ger i es l i ke h epact ect o m y, segment ect omy & liver t ransplant at ion.
M ETHODS
The aim of t he st udy w as t o know t he int rahepat ic ram ificat ion pat t ern of port al vein in right lobe of l i ver & i t s vari at i on s. In t h e p resent st u d y, 25 hum an cadaver livers obt ained aft er aut opsy in
S. N M edical College, Agra during 2005 t o 2008.
The liver specimen w as removed en-bloc along w it h t he port ion of infer ior vena cava & all st ruct ures at port a hepat is remained int act. The specimen w as t horoughly w ashed in running tap w at er w it h gent le pressure t o squeeze out any residual blood or clot s present in port al vein or h epat i c v ein . Th e p o r t al v ei n w as t h en cannulat ed w it h glass canulae w it h lat ex t ubing on ot her end and t he liver gent ly perfused w it h physiologic saline t o flush t he organ. Af t er sut ure-ligat ion of ident ified leaks, drainage of t he saline solut ion done. Cases w it h hepat ic t r au m a, gr o ss li v er p at h ol o gy o r sign s o f decomposit ion w ere excluded from t he st udy.
Preparation of cast material: 20 grams of But yl but yr at e gr anules w er e m ixed w it h 100 m l acet one & cont inuously st irred t o m ake t hick homogenous solut ion of 20 % But yl but yrat e.
Infusion of cast material: Butyl but yrate solution w as inject ed at a const ant pressure int o t he port al vein unt il increase in resist ance felt due t o increase in pressur e w it hin t he vessel & solut ion could be felt on surface of liver. On av er age, 70 – 90 m l co lor ed so lut i on w as required for right lobe. There aft er t he cannula w as clamped w it h sut ure placed earlier or w it h art ery forceps. Aft er infusion, t he inject ed liver w as placed in 10 % Formal saline for 24 hours at room t emperat ure (20°C) for polymerizat ion of infused but yl but yrat e solut ion.
Corrosion of Parenchyma: M acerat ion of liver t issue achieved by whole-organ immersion in 1.8 N KOH solut ion at 68°C for 24 hrs. After 24 hours w hen t ot al macerat ion of w hole parenchyma occur, t he soft en parenchym a w as rem oved t horoughly by w ashing w it h slow running w at er and t he cast t hus obt ained cleaned t o remove any residual organic mat erial w it h fine probe & fine forceps. The cast s w ere t hen phot ographed & t he observat ions w ere not ed.
RESULTS AND DISCUSSION
In all 25 cases, t here w as single por t al vein found. The t w o t ype of pat t ern w as observed in port al vein ramificat ion (first order branch)
vein in 23 of 25 cases (92%). It w as observed as t he commonest t ype by t he ot her aut hors also. [6-11]
ii. Trifurcat ion t ype - The main t runk of portal vein w as divided int o t hree branches – right ant erior port al vein (RAPV), right posterior portal vein (RPPV) & left port al vein. It w as observed in 2 of 25 cases (8%) in present st udy w hile observed by Yam ane [7] in 12% cases & by Ort ale [10]in 22.2% cases. In such cases, during right hepatect omy, bot h RAPV & RPPV should be ligated separately, as one of t hese branches can be mistaken for t he right portal vein. If one o f t h ese r em ain ed u n -li gat ed , sev er e hemorrhage can result . Type III (RPPV as first branch & RAPV & LPV as common t runk) w ere not found in any of t he case of our st udy as it was seen by Yamane [7] in (8% of t he cases). (Table – 1) Quadrificat ion & ot her rare variat ion w ere not observed in t he present st udy.
The lengt h of t he right port al vein ranged from 0.5 t o 1.8 cm in t he present st udy. The lengt h of t he ant erior branch of right port al vein (RAPV) varied from 0.5- 2.5 cm and t he lengt h of t he post erior branch of right port al vein (RPPV) varies from 1.0 – 2.4 cm. The lengt hs of t hese second order branches w ere st udied by very few scient ist & t hese w ere new observed findings of t he present st udy. (Table-2)
The angle bet w een RPV & LPV i.e. port al angle have t he range from 90 °– 170 °. It w as st at ed t hat t he RPV & LPV had obt use angle in most of the cases. The angle betw een Right portal branch & main portal trunk varies from 100 °– 170 ° while t he angle bet w een LPV & t he main t runk w as from 80 °– 130 °. These observat ions concluded t hat RPV w as more in t he line of main port al t runk. The angle bet w een t he RAPV & RPPV has range from 58°-95 °. In 7 of t he 25 cases ( 28 %) it has valve more t han 90° w hile it w as more t han 90° in 20 % of all t he cases as observed by Arora [11]. (Table-3)
The ramificat ion pat t ern of right port al vein as follow s:
In t he present st udy, in 20 of t ot al 23 cases (87%), t he right port al vein bifurcat ed int o right ant erior port al vein (RAPV) & right post erior port al vein (RPPV). While in remaining 3 of 23 cases (13%) t rifurcat ion t ype pat t ern w as
observed in w hich t he right port al vein w as divided int o t hree branches -right ant erior-superior vein (P8), right ant erior-inferior vein (P5) & right post erior port al vein (RPPV). This finding w as also ob ser v ed b y Gu p t a (1977)[ 6] (Table-4). In 2 of 25 cases PRV was absent as RAPV & RPPV direct ly originat ed from m ain portal vein (t rifurcat ion t ype) in t his st udy.
The right anterior port al vein usually ran, forming a gent le curve, t ow ard t he superior direct ion t o b eco m e t h e an t er i o -su p er i o r p o r t al vei n occupying t he superior region of t he ant erior – medial segment of right lobe of liver (Segment VIII). Su per io r ly, r ight ant er i or po r t al v ein continued as anterio-superior branch t o Segment VIII and know n as P8 branch of RAPV. According t o Yamane (1988)[7] t he Right anterior portal vei n bef or e r eachi ng t o segm ent VIII, has diverged int o various branches running t ow ard ant inferior direct ion t o supply t he ant erio-inferior segment (segment V). The diamet ers & numbers of branches diverging from t he right ant erior port al vein int o segm ent V & t heir ramificat ion sit es w ere variable. The ant erio-inferior branch having maximum diamet er w as given t he nam e P5 m ax branch of RAPV. The variat ion of ramificat ion of right ant erior port al vein (RAPV) as follow ed:
Ramification of anterio-superior (P8) branch f ro m RAPV: Ther e w er e t h r ee t y p e o f ramificat ion seen:
I. Bifurcat ion t ype : In 18 of 25 cases (72 %), t he right ant erior port al vein w hile running t ow ard t he superior dir ect ion split int o t w o m ajor branches for ant erio-superior segment , t hese branches w ere named as P8 – ant erior branch & P8 – post erior branch (bifurcat ion t ype).
II. P8 - one pedicle t ype : in t he present st udy, in 2 of 25 cases(8%), single t runk (P8 - one pedicle t ype) t o t he ant er ior super ior segm ent of segment VIII w as t here as t he cont inuat ion of right ant erior port al vein.
III. P8 – t rifurcat ion t ype: In 5 of 25 cases(20%) , t he RAPV (P8 – t rifurcat ion t ype) t rifurcat ed t o give t hree branches in ant erio- superior direction for t he segment VIII.
Int J Anat Res 2014, 2(4):791-96. ISSN 2321-4287 observed by Arora [11]w ho has observed t he bifurcat ion patt ern only in 40% of t he cases. The present findings w ere more close t o t he Yamane & Ortale[7,10] ( Table – 5)
Ram ificat ion of Ant erio-inferior (P5 m ax ) branch from RAPV: There w ere t w o t ype of ramificat ion of ant erio-inferior (P5 max) branch seen:
i. P5 -common t ype: The t ype in w hich P5 max branch ramified on the proximal side of t he major port al vein of segment VIII . it w as observed in 18 of 25 cases (72 %).
ii. P5 – P8 ant erior t ype: P5 max branch ramified from P8 ant erior port al vein w as observed in 7 of 25 cases (28%). P5 – P8 post erior t ype w as not observed in t he present st udy. (Table -5)
Ram ification of Right Posterior Portal Vein (RPPV): RPPV originat ed from RPV or direct ly from port al t runk. It ramified int o number of t he branches t o supply post erio- superior (segment VII) & post erio- inferior (segment VI) segment . The number of t he branches varies from 1 t o 4. Thr ee t yp es o f r am if icat io n p at t er n w er e observed:
i. Fan shaped: It w as t he most common t ype of r am i f icat io n pat t er n ob ser v ed . Th e r i gh t post erior port al vein ran t ow ard t he post erior-superior direct ion as a cont inuous t runk w hile ram ifying int o several sm all branches like t he ribs of t he fan on a plane almost parallel t o t he post erior aspect of t he liver. Usually t he first branch w as given in inferior direct ion t o t he segm ent VI & rem aining t r unk divided int o superior & inferior major branches for post erio-superior ( P7) & post erio – inferior( P6) . This pat t ern w as observed in 16 of 25 cases (64%).
ii. Bifurcat ion t ype : The right post erior port al vein ran t oward t he posterior- superior direct ion & soon divided int o post erio- superior ( P7) & post erio – inferior( P6) branches. It w as observed in 7 of 25 cases (28 %).
iii. Trifurcat ion t ype: t he right posterior portal vein divided int o t hree br anches post erio-super ior ( P7), post erio – inferior( P6) & an int ermediat e branch w hich soon divided int o superior & inferior branches. It w as observed in 2 of 25 cases (8%). Comparat ive observat ions are show n in t he t able – 6.
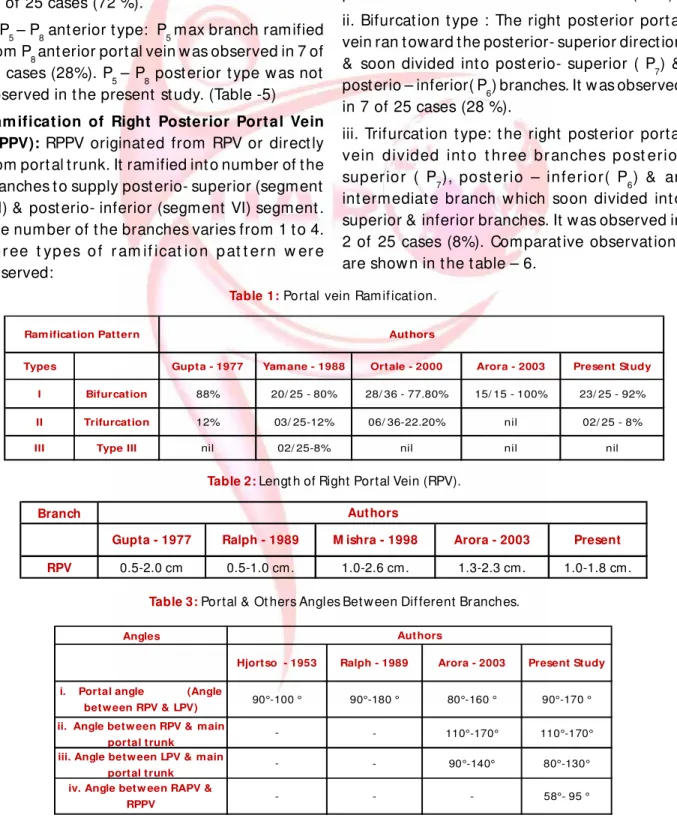
Table 1: Portal vein Ram if icat ion.
Table 2: Lengt h of Right Portal Vein (RPV).
Branch
RPV 0.5-2.0 cm 0.5-1.0 cm. 1.0-2.6 cm. 1.3-2.3 cm. 1.0-1.8 cm.
Authors
Gupta - 1977 Ralph - 1989 M ishra - 1998 Arora - 2003 Present
Ram ification Pattern Authors
Types
I Bifurcation 88%
II Trifurcation 12% nil
III Type III nil nil nil
03/ 25-12%
Gupta - 1977 Yam ane - 1988 Ortale - 2000 Arora - 2003 Present Study
20/ 25 - 80% 28/ 36 - 77.80% 15/ 15 - 100% 23/ 25 - 92%
06/ 36-22.20% 02/ 25 - 8%
02/ 25-8% nil
Table 3: Portal & Ot hers Angles Bet w een Dif ferent Branches.
Angles
ii. Angle betw een RPV & main
portal trunk - 110°-170° 110°-170°
iii. Angle betw een LPV & main
portal trunk - 90°-140° 80°-130°
Ralph - 1989 Hjortso - 1953
i. Portal angle (Angle betw een RPV & LPV)
iv. Angle betw een RAPV & RPPV
-- - - 58°- 95 °
90°-100 ° 90°-180 ° 80°-160 ° 90°-170 °
Present Study Arora - 2003
Table 4: Right portal vein (RPV) Ram ificat ion.
I Bifurcation 88% 100% 100% 100% 87%
II Trifurcation 12% - - 13%
Ramification Pattern Authors
Types Gupta - 1977 Yamane - 1988 Ortale - 2000 Arora - 2003 Present Study
Table 5: Right ant erior portal vein (RAPV).
iii. - NA
Ramification Pattern Authors
Types
Ramification pattern of Anterio-superior branch (P8)
i. - 60%
Gupta - 1977 Yamane - 1988 Ortale - 2000 Arora - 2003 Present Study
One pedicle (major P8 )
02/ 25 - 8% 05/ 36 - 14%
02/ 25- 8%
iii. P5m ax -P8 posterior
type nil nil nil
Ramification pattern of Anterioinferior branch (P5) from RAPV
i. P5 max from
common P8
- 80%
ii. P5 m ax -P8 anterior
type - 10/ 25 -40% 20%
ii.
18/ 25 -72% 19/ 36 -52.8%
13/ 25 -52%
2/ 25 -8%
18/ 25 -72% 30/ 36 -83%
21/ 25 -84%
Bifurcation type
5/ 25 -20% 1/ 36 -2.8%
2/ 25 -8%
Trifurcation type
- 40%
16/ 36 -44.4% 7/ 25 -28%
Table 6: Right post er ior portal vein (RPPV).
I Fan type nil NA
Gupta -1977 Yamane -1988
7/ 25 -28%
4/ 36 -11.2%
3/ 25 -12% 02/ 25 -8%
Ortale -2000 Arora -2003 Present Study
16/ 25 -64% 16/ 36 -44.4%
13/ 25 -52%
II 100% NA
II Trifurcation type nil NA
Bifurcation (P7) & (P6) 09/ 25 -36% 16/ 36 -44.4%
Ram ification Pattern Authors
Types
Fig. 1: Corrosion cast of intrahepat ic ram ificat ion patt ern of port al vein; blue color – right lobe of liver & r ed color – left lobe of liver. Port al vein bifurcat ed int o RPV & LPV; RPV b if u r cat ed i n t o RAPV & RPPV. RAPV sh o w i n g b i f u r cat i o n i n t o an t e r i o -su p er i o r ( P8)& an t e r i o r -inf erior (P5 m ax com m on t ype); RPPV show ing Fan type ramification.
Int J Anat Res 2014, 2(4):791-96. ISSN 2321-4287 Fig. 3: Co r ro sio n cast of in t r ah epat ic ram if i cat io n pat t ern of port al vein; blue color – right lobe of liver & red color – left lobe of liver. RPV bifurcat ed int o RAPV & RPPV. RAPV show ing bifurcat ion int o ant erio-super ior (P8) & ant er ior -inf er i or (P5 m ax com m on t ype); RPPV show ing Fan t ype ram if icat ion.
Fig. 4: Corrosion cast of intrahepat ic ram ificat ion patt ern of portal vein; red color – right lobe & left lobe of liver. RPV b if u r cat ed i n t o RAPV & RPPV. RAPV sh o w i n g bifurcat ion int o ant erio-superior (P8) & ant erior-inferior (P5 m ax com m on t ype); RPPV show ing bifurcat ion t ype r am if icat ion.
CONCLUSION
The present st udy w as direct ed t o know t he int rahepat ic ramificat ion pat t ern of port al vein & it s variat ions. The det ail of ramificat ion up t o t hird order branches of port al vein w as st udied in different hepat ic segment s w hich w as
Conflicts of Interests: None
REFERENCES
[1]. Couinaud C. Liver lobes and segm ent s: not es on t he anat om ical archit ect ure and surgery of t he liver. Presse M ed. 1954 M ay 5;62(33):709-12. French. [2] . Hjort sjo CH. The t opography of t he int rahepat ic
duct syst em s. Act a Anat (Basel) 1951; 11(4):599-615.
[3]. Elias H, Pett y D. Gross anat omy of the blood vessels and duct s w it hin t he hum an liver. Am J Anat . 1952 Jan; 90(1):59-111.
[4]. Healey JE Jr, Schroy PC. Anat omy of the biliary duct s w it hin t he hum an liver ; analysis of t he prevailing pat t ern of branching and t he m ajor variat ions of t h e b i l i ar y d u ct s. AM A Ar ch Su r g. 1 95 3 M ay;66(5):599-616.
[5]. Goldsm it h NA, Woodburne RT. The surgical anatomy per t aining t o liver r esect ion. Surg Gynecol Obst et . 1957 Sep;105 (3):310-8.
[6]. Gupt a SC, Gupt a CD, Arora AK. Sub-segm entat ion of t he hum an liver. J Anat . 1977 Nov;124 (Pt 2):413-23.
[7]. Yam ane T, M ori K, Sakam ot o K, Ikei S, Akagi M . Int rahepat ic ram ificat ion of t he port al vein in t he r ight and caudat e lobes of t he liver. Act a Anat (Basel) 1988; 133 (2):162-72.
[8] . Ralphe G. Surgical anat omy of t he liver. Surg. Clin. N. Am er. 1989;69:179-182.
[ 9] . M ishr a S, Reh okhi eya, Ajm an i M L, M u r t y OP. Segm ent al anat om y of h um an l iver b y special t echnique of vascular inject ion. Journal of Forensic M edicine and Toxicology.1998;25:5-9.
[ 10] .Or tale JR, Hum bert o C, Azevedo NF, Cast ro CM . Anat om y of t he int r ahepat ic ram ificat ion of t he port al vein in t he right hem i liver. Cells, Tissues, Organs. 2000; 166:378-387.
[11]. Arora. J, Kapur. V, Kakkar. A, Dixit . P. C. Ram ificat ion pat t ern of port al vein in r ight lobe of liver – A Co r ro sion Cast St u dy. J Anat . Soc. In dia 2003; 52(1);12-14.
observed in very few Indian st udies. Applicat ion of t he t hese det ail variat ions in t he ramificat ion pat t ern of port al vein w it h t he advancement in surgical t echnique involved in hepat ic resect ion & liver t ransplant at ion w ill revolut ionize t he ent ire approach in t he managem ent of liver disorders.
How to cite this article
:
Rajput AS, Kumari S, M ishra GP. A CORROSION CAST STUDY OF RAM IFICATION PATTERN OF PORTAL VEIN IN RIGHT LOBE OF HUM AN LIVER.Int J Anat Res 2014;2(4):791-796.