www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Assessment
of
the
light
intensity
of
otoscopes
utilized
in
teaching
hospitals
夽,夽夽
Vinicius
Ribas
Fonseca
a,b,
Giovana
Bittencourt
Basso
c,∗,
Mariana
Nagata
Cavalheiro
caDepartmentofOtorhinolaryngology,UniversidadePositivo,Curitiba,Paraná,PR,Brazil bDepartmentofOtorhinolaryngology,HospitalCruzVermelha,Curitiba,Paraná,PR,Brazil cDepartmentofMedicine,UniversidadePositivo,Curitiba,Paraná,PR,Brazil
Received19February2014;accepted15October2014 Availableonline21July2015
KEYWORDS Otoscopy; Otoscopes; Light
Abstract
Introduction:Toattainanaccurateotoscopicdiagnosis,afunctioning devicewithadequate capacitymustbeused.
Objective: Evaluatethelightintensityofotoscopes,comparingitutilizingthebatteriespresent atthemomentofcalibrationandafternewbatteriesweresupplied.
Methods:Cross-sectionalstudyofahistoricalcohort,whichassessed38otoscopes,measuring thelightintensitywiththebatteriespresentatthemomentofassessmentcomparedtothe intensitywithnewbatteries,aswellaschargeofthetestbatteriesandthenewbatteries.
Results:Themeanofthesumofnewbatteries’chargewas3.19V,andofthetestbatteries was 2.70V,representingadecreaseof18.02%incharge.Themeanluminositywiththenew batterieswas366.89lumens,whereasinthetestbatteriesitwas188.32lumens,representing adecreaseof83.75%inthelightintensity.Student’st-testwasappliedfordatacomparison, showingastatisticaldifferencebetweenthelightintensitywiththeoriginalbatteriesandthe newbatteries(p=0.0001;CI=0.95).
Conclusion: Therewasastatisticallysignificant differencebetweentheproportions oflight intensityintheotoscopes.Asmallvariationinbatterychargeresultsinagreatvariationin light.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽
Pleasecitethisarticleas:FonsecaVR,BassoGB,CavalheiroMN. Assessmentofthelightintensityofotoscopesutilized inteaching hospitals.BrazJOtorhinolaryngol.2015;81:479---84.
夽夽Institution:UniversidadePositivoandHospitalCruzVermelha,Curitiba,PR,Brazil.
∗Correspondingauthor.
E-mail:[email protected](G.B.Basso).
http://dx.doi.org/10.1016/j.bjorl.2015.07.006
Luz Introduc¸ão:Paraarealizac¸ãodeumdiagnósticootoscópicoprecisodeve-seutilizarumaparelho
funcionandocomumacapacidadeadequada.
Objetivo:Avaliaraintensidadeluminosadosotoscópioscomparandoaintensidadedaluzcom aspilhasencontradasnomomentodaaferic¸ãoecompilhasnovas.
Método: Estudodecoortehistóricacomcortetransversal,ondeforamanalisados38otoscópios, sendorealizadaaaferic¸ãodaqualidadeluminosacomapilhautilizadaecomparadocomuma pilhanova,eaaferic¸ãodacargadaspilhasnovaseemutilizac¸ãonomomentodoexame.
Resultados: Amédiadasomadascargasdaspilhasnovasfoide3,19V,eadaspilhastestesfoide 2,70V,representandodecréscimode18,02%nacargadaspilhas.Amédiadaluminosidadecom aspilhasnovasfoide366.89lúmens,ecomapilhatestefoide188.32lúmens,representando decréscimode83,75%naintensidadeluminosa.FoiaplicadootesteTparacomparac¸ãoentre osdados,ondepercebe-sediferenc¸aestatísticaentreaintensidadeluminosacompilhastestes enovas(p=0,0000;IC=0,95).
Conclusão:Houvediferenc¸aestatisticamentesignificativaentreaproporc¸ãodeintensidadeda luzdosotoscópios.Umapequenavariac¸ãodapilhaproporcionaumagrandevariac¸ãonaluz. ©2015Associac¸ãoBrasileira deOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicadopor ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Theotoscopeisamedicaldevicecommonlyusedinboth pri-marycareandhospitals.1Thefirstotoscopesweredesigned
forviewingtheearcanal,asapairoftweezers,similarto currentrhinoscopes.1
Otoscopy is the main focus of the otological physical examinationandshouldbeperformedwithanappropriate otoscope that offers a good light source, preferably with halogen light (white)so asnot interfere withthe normal color of the outer ear and the middle ear structures.2 It
shouldbe attached to a disposable or sanitized otoscope speculumandbeofanappropriatesizefortheearconduit tobeassessed.2
Adequate illumination of the tympanic membrane requiresspecialequipmentandanopenandcleanearcanal, butthe circumstances are rarely optimal.3 Approximately
one-third of physicians exchange the otoscope bulbs less oftenthanrecommended,andone-thirdofotoscopesdonot haveadequatelightingcapacity.3
Thereareinsufficientstudiesintheliteraturethathave evaluated the ideal luminosity for good diagnostic accu-racyor thathave assessedtheinfluence ofbattery power onthequalityof light.There isonly thestudy byBarriga etal.,carried out in1986, which evaluatedthe intensity oflightofotoscopes,takingintoaccountlampreplacement frequency.4
Thepresent studyaimedtoevaluatethelightintensity ofotoscopes inoutpatientclinics,offices, andemergency wardsofteachinghospitals,bycomparingtheintensityof lightwithbatteries foundatthemomentofmeasurement andwithfullychargedbatteries.
Methods
Thestudywascarriedoutwiththeauthorizationof Hospi-taldaCruzVermelha(Paraná,Brazil)andHospitalPequeno
Príncipe,wheredatacollectionwasconductedfromJune, 2013, to January, 2014. It was a historical cohort study withcross-sectionaldesign,andasitdidnotinvolvehuman beings, approval fromtheresearch ethicscommittee was notnecessary.
Selectionofstudysiteandthetypesofotoscopes
Two schoolhospitals were chosen toassess thequality of light ofotoscopes inplaceswithsituations believedtobe closetotheidealforsymptomaticpatientassessment.
Thisstudyevaluatednotonlytheotoscopesofthe institu-tions,butalsothosebelongingtothephysicianswhoagreed toparticipateinthestudyafterabriefexplanationofthe studyobjectives.
Thesamplecollectionsitesforassessmentwere:general outpatient clinic, emergency, otorhinolaryngology clinic, otorhinolaryngologyoffices,infirmary,andacademic outpa-tientclinicofbothhospitals.
Theinclusioncriteriawereassessedotoscopeswith halo-genlight, light-emittingdiodes(LED),commonlampbulb, oropticalfiber,poweredbyenergysuppliedbyconventional batteries.
The exclusion criteria included otoscopes powered by electricity or powersupply providedby rechargeable bat-teries,orthosewhoseownersrefusedtoparticipate.
A total of 38 otoscopes were assessed, of five differ-ent brands, Welch Allyn®, Missouri®, Piko®, Omni® and
Mikatos®, of which six belonged toHospital da Cruz
Ver-melha(Paraná,Brazil),withtheremainderbelongingtothe serviceprovidersoftheinstitutions.
Otoscopeluminosityandbatteryintensity assessment
Figure1 Darkbox.
batteriesboughtbytheresearchers,dependingonthetype ofotoscope,withcharge>1.5V.
The charge of the test batteries of the otoscopes to be assessed was evaluated before the measurement of light intensity through a calibrated voltmeter to deter-minethechargelevel.Additionally,thenewbatterieswith charge>1.5Vwereassessed,sothattheycouldbeverified asfullycharged.
Adarkboxwasconstructed(Fig.1),whichdidnotallow light to enter after being closed, so that the otoscope lightintensityassessmentcouldbestandardizedwithoutthe influenceofexternallight.
AnIcel® lightmeter, calibratedtoa2000luxsensitivity
factor,haditsphotometeraffixedtooneoftheboxwalls; thephotometerwasmobileandcouldbemovedupwardor downward,asitwasfixedbyVelcro® strips.Thus,itcould
beplacedperpendicularly totheotoscopelight extremity atthetimeofmeasurement.
The otoscopes were mounted on a holderprepared to keepitstandingat4cmfromthebasisandperpendicularto thephotometercentralpointwitha3-mmmeanspeculum opening,accordingtotheotoscopemodel(Fig.2).
Aftertheotoscopewaspositioned,itwasturnedonand the box was closed, after which the light intensity was measuredbythelightmeter.Themaximummeasuredlight intensitywasrecorded.
Thisprocedurewasfirstperformedwithotoscopeswith thetestbatteriesandthenwiththenewbatteries,to deter-minetheproportioninpercentageoflightintensity inthe otoscopes with the test batteries, considering 100% light intensityfoundwiththenewbatteriesforeachtested oto-scope.Datawerecollectedbytworesearchers,whowere togetherduringallmeasurements,whichwereenteredinto aspreadsheetandsubmittedtostatisticalanalysis.
Statisticalanalysis
Thechargeintensityofthetestandnewbatteriesandthe proportionoflightintensityoftheotoscopeswerecompared
Figure2 Otoscopefixedatthebaseata4-cmdistanceand lightsourcedirectedtothecentralpointofthephotometer.
usingtheStudent’st-testforpaireddata,astheywere com-paredwiththeresultsofthesameotoscope,butwiththe differentbatteries,withap-value<0.05considered statis-ticallysignificant.
Results
All otoscopes assessed in this study used two non-rechargeablebatteriesfortheiroperation.Themeanofthe sum of the charges of the two new batteries was 3.19V, whereasthetwotestbatterieshadameanvalueof2.70V. Thisrepresentedan18.02%decreaseinthemeanchargeof thetwobatteries(Table1).
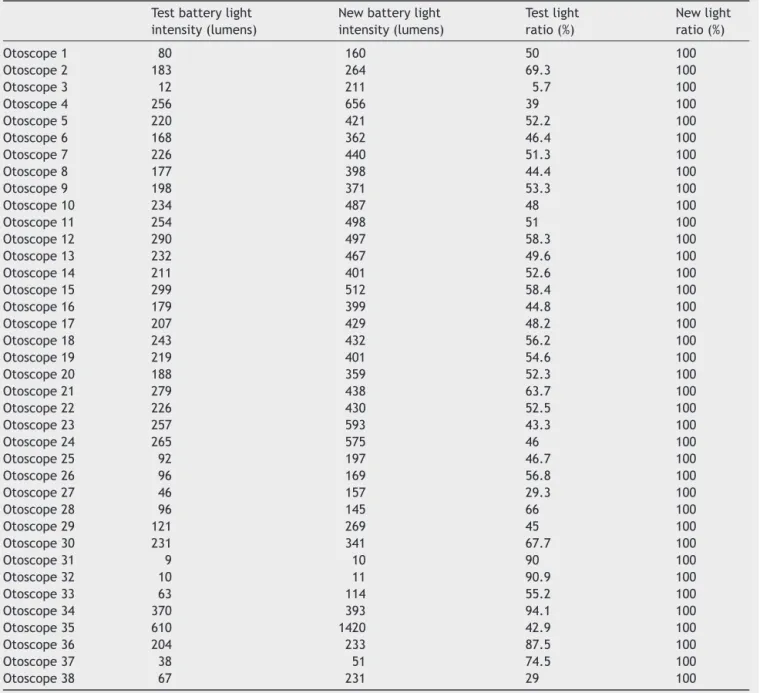
Themaximumlightcapacityineachotoscopewas indi-vidually assessed and the value measured with the new batteriesconsideredtobe100%.Themeanintensityofthe 38assessedotoscopeswas366.89lumens.Themean inten-sity achieved with the test batteries was 188.32lumens, whichshowsthatonaverage,theotoscopesfunctionedat 54.42%oftheirpotential(Table2).
Table1 Meanandstandarddeviationofthetotalcharge ofbatteries,andtestbatterychargeratioinrelationtothe newbatteries.
Mean Standard
deviation
Fullchargeoftestbatteries(V) 2.70 0.32 Fullchargeofnewbatteries(V) 3.19 0.02
Testchargeratio(%) 84.73 10.31
deviation
Testlightintensity(lumens) 188.32 114.783 Newlightintensity(lumens) 366.89 238.272 Testlightintensityratio(%) 54.42 17.33
Newlightintensityratio(%) 100 0
Otoscope1 hadthe lowest battery power; itoriginally hadonly40.9%ofthemaximumvoltageandbattery replace-ment generated a 100% improvement in light intensity (Tables3and4).
lightintensitywithtestbatteriesandnewones(p=0.0000; CI=0.95).
Discussion
Medicalpracticedemonstratesthatotoscopeilluminationis criticalforadequatepatientotologicalassessment,andthis examinationisessentialforthediagnosisandmonitoringof otologicalpathologies.5
The otoscopes assessed in this study used non-rechargeablealkaline batteries, which,when new,have a totalchargeof1.5Veach.Ifthevoltageisbelow0.8V,the
Table3 Fullbatterychargeandtestbatteryratioinrelationtothenewbatteriesofeachotoscope.
Sumofchargeof testbatteries(V)
Sumofchargeof newbatteries(V)
Testbattery ratio(%)
Newbattery ratio(%)
Otoscope1 1.30 3.18 40.9 100
Otoscope2 2.62 3.18 82.4 100
Otoscope3 1.30 3.19 40.7 100
Otoscope4 2.34 3.16 74 100
Otoscope5 2.70 3.18 84.9 100
Otoscope6 3.00 3.16 94.9 100
Otoscope7 2.73 3.18 85.8 100
Otoscope8 2.38 3.22 73.9 100
Otoscope9 2.49 3.22 77.3 100
Otoscope10 2.60 3.23 80.5 100
Otoscope11 2.67 3.21 83.2 100
Otoscope12 2.84 3.22 88.2 100
Otoscope13 2.73 3.21 85 100
Otoscope14 2.64 3.22 82 100
Otoscope15 2.87 3.21 89.4 100
Otoscope16 2.43 3.21 75.7 100
Otoscope17 2.63 3.20 82.2 100
Otoscope18 2.77 3.21 86.3 100
Otoscope19 2.68 3.19 84 100
Otoscope20 2.38 3.20 74.4 100
Otoscope21 2.82 3.20 88.1 100
Otoscope22 2.74 3.19 85.9 100
Otoscope23 2.64 3.19 82.7 100
Otoscope24 2.85 3.18 89.6 100
Otoscope25 2.53 3.18 79.5 100
Otoscope26 2.87 3.18 90.2 100
Otoscope27 2.72 3.16 86 100
Otoscope28 3.04 3.16 96.2 100
Otoscope29 2.98 3.18 93.7 100
Otoscope30 2.94 3.18 92.4 100
Otoscope31 3.00 3.18 94.3 100
Otoscope32 3.08 3.18 96.8 100
Otoscope33 2.76 3.18 86.8 100
Otoscope34 3.00 3.16 94.9 100
Otoscope35 3.03 3.18 95.3 100
Otoscope36 3.00 3.11 96.5 100
Otoscope37 3.04 3.14 96.8 100
Table4 Lightintensityandtestbatterylightratioinrelationtothenewbatteriesineachotoscope.
Testbatterylight intensity(lumens)
Newbatterylight intensity(lumens)
Testlight ratio(%)
Newlight ratio(%)
Otoscope1 80 160 50 100
Otoscope2 183 264 69.3 100
Otoscope3 12 211 5.7 100
Otoscope4 256 656 39 100
Otoscope5 220 421 52.2 100
Otoscope6 168 362 46.4 100
Otoscope7 226 440 51.3 100
Otoscope8 177 398 44.4 100
Otoscope9 198 371 53.3 100
Otoscope10 234 487 48 100
Otoscope11 254 498 51 100
Otoscope12 290 497 58.3 100
Otoscope13 232 467 49.6 100
Otoscope14 211 401 52.6 100
Otoscope15 299 512 58.4 100
Otoscope16 179 399 44.8 100
Otoscope17 207 429 48.2 100
Otoscope18 243 432 56.2 100
Otoscope19 219 401 54.6 100
Otoscope20 188 359 52.3 100
Otoscope21 279 438 63.7 100
Otoscope22 226 430 52.5 100
Otoscope23 257 593 43.3 100
Otoscope24 265 575 46 100
Otoscope25 92 197 46.7 100
Otoscope26 96 169 56.8 100
Otoscope27 46 157 29.3 100
Otoscope28 96 145 66 100
Otoscope29 121 269 45 100
Otoscope30 231 341 67.7 100
Otoscope31 9 10 90 100
Otoscope32 10 11 90.9 100
Otoscope33 63 114 55.2 100
Otoscope34 370 393 94.1 100
Otoscope35 610 1420 42.9 100
Otoscope36 204 233 87.5 100
Otoscope37 38 51 74.5 100
Otoscope38 67 231 29 100
battery issurely exhausted;for voltagesbetween0.8 and 1.3V,theresultis aweakunit;withvoltagesabove1.3V, thebattery canbeconsideredgood.6The meanchargeof
eachanalyzedbatterywas1.35V,whichisconsideredgood, andeventhen,replacingit byanewbattery offersa sig-nificant gain regarding light intensity. This can be clearly observedwhenshowninpercentages,asanincreaseofat least20%ofbatterychargeresultsinanincreaseofover80% inlightintensity.
When comparingthe increasesinlight intensity,itwas notpossibletoperceiveanyrulesonlightintensity improve-ment.Thisfactisduetothedifferenceinthelampsused intheotoscopesandthevarietyofassessedbrands.Asan example,consider otoscopes1 and3. Otoscope1 showed a100%increaseinlightintensity withanincreaseof144%
of battery power, while otoscope 3, withthe same 144% increaseinthebatterypower,showedanincreaseof approx-imately1700%inluminosity.
InthestudybyBarrigaetal.,theauthorsassessed oto-scopeslocatedin96medicaloffices.4Thelightoutputwas
measuredineachotoscopeandreassessedwithanewlamp, andwhenpossible,anewbatterywasplacedintheunit.4
In approximately one-third of the otoscopes, the light outputwassuboptimal.4Lampreplacementprovided
ade-quateilluminationfor80%oftheotoscopes.4Barrigaetal.
observedthatone-thirdofphysicianschangeotoscopelamps annually,andlessthantwo-thirdsdosoeverytwoyears(as recommended).4Inthatstudy,almosthalfofrechargeable
batteriesweredischarged.4Itwasobservedthatlampbulb
Oneofthedifficultiesinperformingthisstudywas hav-ingaccesstootoscopesatthedesignatedsites,astheywere alwaysbeingutilizedfordiagnosis.Itwasobservedthatthe availableotoscopeinthestudysiteswasnotalwaysthatof theinstitution,whichmakesbatterychargecontroldifficult, aswhentheprofessionalhimselfistheownerofotoscope, he/sheis responsibleforreplacingbatteries.Inthe Emer-gencyDepartmentoftheHospitaldaCruzVermelha(Paraná, Brazil) otoscopes are electric, which provides maximum luminosity,withthestateofthelampbulbrepresentingthe onlyinfluencingfactor.
Regarding the methodology, the researchers had diffi-cultywith theluminosity measurement method standard-ization, asmany items can influence it, such as ambient light, the light direction in relation to the light meter, timeofmeasurement,andthespeculumsize.The comple-tionof the assessment in a controlled environment (dark box) with the light directed to the center of the light meter (perpendicularly), the use of a standard speculum opening(3.00mm), withtheotoscopepositionedonaflat surface and the possibility of changing the light meter height, allowed the standardization of the measurement methodology.
Theauthorsproposeotherstudies,comparingthe influ-enceofthebatterypowerintensityandtheexchangeofthe equipmentlampsassociatedtoaquestionnairedirectedto theassessingphysicianontheinfluenceoftheotoscopelight intensityonthediagnosisofearpathologies.
proportion of light intensity of assessed otoscopes when evaluatedwiththebatteriesusedatthetimeofassessment andwithnew,fullychargedbatteries.
Tocarryoutamorepreciseotoscopicdiagnosis,attention should be paid to the importance of the maintenance of a well-functioning device, withthe capacityclose to the maximum,asasmallvariationinbatterychargeresultsina muchgreatervariationinlightintensity.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.SánchezF. Historiade laORL ---otoscopio y rinoscopio.GAES News.2009:15.
2.SoeiraJMJ[Thesis] Concepc¸ãoedesenvolvimentode um pro-tótipodeumotoscópioóptico-electrónico.Porto:Universidade doPorto;2007.
3.PichicheroME.Acuteotitismedia:improvingdiagnosticaccuracy. AmFamPhysician.2000;61:2051---6.
4.BarrigaF,Schwartz RH,HaydenGF.Adequate illuminationfor otoscopy.Variationsdueto powersource,bulb,andheadand speculumdesign.AmJDisChild.1986;140:1237---40.
5.CocoAS. Cost-effectiveness analysisof treatmentoptions for acuteotitismedia.AnnFamMed.2007;5:29---38.