w w w . j c o l . o r g . b r
Journal
of
Coloproctology
Original
Article
Fecal
occult
blood
test
and
flexible
rectosigmoidoscopy:
tools
for
the
screening
of
colorectal
neoplasms
in
asymptomatic
patients
夽
Mario
Jorge
Jucá
a,∗,
Paulo
Roberto
Torres
Assunc¸ão
a,
Hermann
Nogueira
Hasten-Reiter
Júnior
baFacultyofMedicine,UniversidadeFederaldeAlagoas(UFAL),Maceió,AL,Brazil
bCESMACCentroEducacional,Maceió,AL,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received3March2014 Accepted8July2014
Availableonline28January2015
Keywords:
Colorectalneoplasms Diagnosis
Occultblood
a
b
s
t
r
a
c
t
Purpose:Toassessthefeasibilityandeffectivenessofthefecaloccultbloodtest(FOBT)and flexiblerectosigmoidoscopy (RSS),astoolsusedintheCRCscreening,inasymptomatic patients,from50yearsofage.
Methods:Thestudyistransversalandpresentsasampleof102individuals.TheFOBTused wastheguaiaco,FECA-CULT®method,heldatasingletime,infecescollectedfroma com-pleteevacuation.Individuals,whopresentedthepositiveFOBT,weresenttocolonoscopy complement,although thisisnotprimaryvariableexaminedinthisstudy.Allsubjects underwenttoflexibleRSS,afterbowelpreparation,usingasolutionofsodiumphosphate
monobasicmonohydrateanddibasicsodiumphosphateheptahydrate.
Results:Individualsshowedminimumageof50yearsandmaximum82years,61.6years averageandstandarddeviation+8.1.Ofthe102individuals,42(41%)belongtothemales, whereas60(58.8%)female.TheFOBTpresented10positivecases(9.8%)(IC95%:4.8–17.3%) and92negativecases(90.2%)(IC95%;82.7–95.2%).TheFOBTwaseffectiveat2.9%and pre-sentedfalse-positiveresultin6.9%.TheresultoftheFBOTassociationwithflexibleRSS showedthat70%ofneoplasticpolypsshowednobleeding.Itssensitivitywas30%(IC95%: 0.00–63.40%), thevalueoftherelativeriskwas3.94(IC95%:1.20–12.89)and5.20valued oddsratio(IC95%:−23.15to1.21).Thespecificitywas92.40%(IC95%:86.43–98.35%).The flexibleRSSdetected15polyps,amongwhich,afterhistopathologicalstudy,10were neo-plastic,being09adenomatouspolyps(60%)and01malignity(6.7%)(IC95%:0.20–31.90%) and05non-neoplasticpolyps(33.3%),and03inflammatorypolyps(20%)(IC95%:4.3–48.1%) and02hyperplasticpolyps(13.3%)(IC95%:1.7–40.5%).Neoplasticpolypswerepresentin 60%ofindividualsover60yearsofage.Amongtheadenomatouspolyps,theadenomatous polyptubularprevalenceis53.33%.Amongthe102individuals,flexibleRSSdetected09 adenomatouspolyps(8.82%)and01(0.98%)malignitypolyp.
夽
ResearchperformedatUniversityHospitalProfessorAlbertoAntunes,UniversidadeFederaldeAlagoas(UFAL),Maceió,AL,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](M.J.Jucá). http://dx.doi.org/10.1016/j.jcol.2015.01.002
Conclusion: The toolsFOBT andflexibleRSSpresentedfeasibilityand,whenassociated demonstratedstatisticalsignificanceindetectingpolypsingeneralandimportantclinical significanceonthedetectionofadenomatouspolypsandcolorectalcancer.
©2015SociedadeBrasileiradeColoproctologia.PublishedbyElsevierEditoraLtda.All rightsreserved.
Teste
de
sangue
oculto
nas
fezes
e
retossigmoidoscopia
flexível:
instrumentos
para
o
rastreamento
de
neoplasias
colorretais
em
pacientes
assintomáticos
Palavras-chave: Neoplasiascolorretais Diagnóstico
Sangueoculto
r
e
s
u
m
o
Objetivo:Avaliaraviabilidadeeeficáciadotestedesangueocultonasfezes(TSOF)e retossig-moidoscopia(RSS)flexível,comoinstrumentosutilizadosnatriagemdoCCR,empacientes assintomáticosapartirdos50anos.
Métodos: Esseéumestudotransversaleapresentaumaamostrade102indivíduos.OTSOF utilizadofoiométododoguaiacoFECA-CULT®,realizadoemumaúnicavez,emfezes
cole-tadasdeumaevacuac¸ãocompleta.IndivíduoscomTSOFpositivoforamencaminhados
paraocomplementodecolonoscopia,emboraessanãosejaavariávelprimáriaexaminada nesteestudo.TodosospacientesforamsubmetidosaumaRSSflexível,apósapreparac¸ão dointestinocomousodeumasoluc¸ãodefosfatodesódiomonobásicomono-hidratadoe defosfatodesódiodibásicohepta-hidratado.
Resultados: Os participantes tinham idade mínima de 50 anos e máxima de 82 anos (média±desviopadrão,61,6±8,1anos).Dos102pacientes,42(41%)eramhomens,enquanto 60(58,8%)erammulheres.OTSOFrevelou10casospositivos(9,8%)(IC95%:4,8-17,3%)e92 casosnegativos(90,2%)(IC95%;82,7-95,2%).OTSOFfoieficazem2,9%eapresentou resul-tadofalso-positivoem6,9%.Oresultadodaassociac¸ãodeTSOFcomRSSflexíveldemonstrou que70%dospóliposneoplásicosnãoexibiamqualquersangramento.Suasensibilidadefoi de30%(IC95%:0,00-63,40%),comriscorelativode3,94(IC95%:1,20-12,89)erazãode sensibil-idade(oddsratio)de5,20(IC95%:1,21-23,15).Aespecificidadedaassociac¸ãofoide92,40%(IC 95%:86,43-98,35%).ARSSflexíveldetectou15pólipos,tendosidocontatadoque,depoisdo estudohistopatológico,10eramneoplásicos:9póliposadenomatosos(60%)e1malignidade (6,7%)(IC95%:0,20-31,90%).Alémdisso,aRSSflexíveldetectou5póliposnãoneoplásicos (33,3%):3póliposinflamatórios(20%)(IC95%:4,3-48,1%)e2póliposhiperplásicos(13,3%) (IC95%:1,7%-40,5%).Ospóliposneoplásicosestavampresentesem60%dospacientescom maisde60anosdeidade.Entreospóliposadenomatosos,houveprevalênciatubularde póliposadenomatososem53,33%.Entreos102indivíduos,aRSSflexíveldetectou9pólipos adenomatosos(8,82%)e1(0,98%)pólipomaligno.
Conclusão:FoiconstatadaaviabilidadedosinstrumentosTSOFeRSSflexível;quando associ-ados,demonstraramsignificânciaestatísticanadetecc¸ãodepóliposemgeraleimportante significadoclínicoparaadetecc¸ãodepóliposadenomatososedocâncercolorretal.
©2015SociedadeBrasileiradeColoproctologia.PublicadoporElsevierEditoraLtda. Todososdireitosreservados.
Introduction
Colorectalcancer (CRC)remainsthe second mostcommon
causeofcancermortalityintheUnitedStatesandthefourth inBrazil,withincidenceandmortalityequaltobothgenders.
Althoughtracingreducemortality,byremovingthecancerin
initialstageandthecancerprecursorlesions,knownas
ade-nomatouspolyps,thepreventiveproceduresareveryscarce,
becauseofdoctors,patientsandhealthsystemresistance.1
TheCRC isthe thirdmostcommon cancerinthe world
and the mortality rate has been kept the same, over the
pastfiftyyears.2Tracingmeansusingsimpleteststhatcan
beappliedtothepopulationatriskfordeveloping the
dis-ease,evenasymptomatic,inordertobediagnosedprecursor
lesionofCRCorevencancer,ininitialstage.Thenatural
evo-lutionofthe adenomatouspolyptotheadenocarcinomais
recognized. However,the sequencesincethe emergenceof
adenoma,growthtomalignizationlastsabout10years, favor-abletimefortheriskpopulationtoundergotheCRCscreening andreducethemortalityratebyCRC,inrelationtoa popula-tioncontrol,notsubjectedtothescreening.3,4
The CRC screeningis justifiedby the high incidenceof
adenomatouspolypsandCRCintheinitialstage,with signifi-canttherapeuticresultinpopulationatrisk.Inasymptomatic
patients survival among five years reaches 80–90%, if the
tumorisconfinedtotheintestinalwall.Therefore,itshould
educate the population about the importance of the CRC
screening,todecreaseitsincidence.5
Theaimofthisstudyistoevaluatethefeasibility, effective-nessofflexiblerectosigmoidoscopyandfecaloccultbloodtest, astoolsinthepreventionofcolorectalcancerinasymptomatic individualsandlow-risk.
Methods
Thesample analyses by sectional form 102 asymptomatic
individuals,aged50yearsoldormore,fromvariousregions oftheStateofAlagoas.
Theindividualswhichwereincludedinthissample
per-formedthe followingcriteria: equal or higher age than 50
yearsold,asymptomaticwithregardtocolorectalcomplaints.
Patientswhichshowedalarmsigns,suchasabdominalpain,
altered intestinaltransit, visible presenceofblood withor
withoutmucousinfecesandtenesmuswereexcludedfrom
this research. The onewho reported the presence ofCRC
onearlyfamiliar historyand/orpersonalhistory andthose
whorefusedtoparticipateintheresearchprotocolwerealso
excludedfromthisscreening.
Thefollowingvariableswereanalyzed:age,being investi-gatedindividualsfrom50yearsold,consideringbeingtarget
fortracing, forpresenting lowrisk todevelopthe CRC. As
regardtogender,therewasnoselection.Thefecaloccultblood testandflexiblerectosigmoidoscopyfollowedtheguidanceof elaboratedesign,inwhichallindividualsunderwentinitially toFOBTthentheflexibleRSS,onlythosewithpositiveFOBT
werethenexaminedbycolonoscopy.
The individuals were advised to avoid red meat and
foodswithhigh peroxidase activity,suchasradish, turnip,
cauliflowerand broccoli, for3days priorto the exam and
onthedayofcollection.Theywerealsoadvisednottotake anti-inflammatorydrugs,corticosteroids,aspirin,iron, anti-coagulant,colchicine,iodine,bromides,boricacid,reserpine, laxativeandvitaminC.Itwasallowedfruitsandvegetables, preferablyboiled.
Allofthem receivedguidance toavoidthecollection of
feces,whenthereisbleedinghemorrhoids,bleedinginthe
gumsmucousorduringmenstrualperiod.Then,thefecesofa
completeevacuationwerecollectedandanalyzedonthesame
day.Thefecaloccultblood test(FOBT)washeldbyFECA–
CULT®,alsoknowninclinicalpracticeasguaiacmethod,
hav-ingascharacteristicaspecialpapertape,impregnatedwith
resinnaturalguaiac.
TheFOBT was conducted priorthe rectosigmoidoscopy,
toavoidfalse-positiveresult, causedbyblood from biopsy,
polypectomyorevenminortraumasincolonicmucosa.
For the realization of flexible RSS, the individual has
undergoneaintestinepreparation,usingthecontentsoftwo
vials,eachcontaining130mLofsodiumphosphatesolution
monobasicmonohydrate(16g/100mL)andsodiumphosphate
dibasicheptahydrate(6g/100mL).Thisenemawasused2and
1hbeforetheendoscopicexamination.
These examinations were held at the coloproctology
serviceoftheUniversityHospitalProf.AlbertoAntunes,ofthe FederalUniversityofAlagoas.
The colonoscopy was not a primary tool used in this
screening,butitwasmandatoryintheimmediatefollow-up
examinationofindividualswhopresentedpositiveFOBTand
inpatients whereadenomatous polypwasdetectedwitha
high degreeofdysplasiaand/ormalignitypolyp,evenwith
thenegativeFOBT,consideringhigherchanceofbeing
diag-nosedsynchronicneoplasticlesions,intheproximalcolonof theseindividuals.Alllesionsweresentforhistopathological
diagnosis,hematoxylin–eosintechnique.
ForstatisticalanalysisweusedtheprogramEpi-Info ver-sion 3.4.3,obtainingrisk oddsratio,relative risk,the Fisher exacttest,Chisquareandadhesionchisquare,allwith95%IC. SensitivityandspecificitywereundertakenbyEPIDAT,version 3.1,usingthe95%confidenceinterval.
Results
The colorectal cancerscreening, using the FOBT tools and
flexibleRSS,washeldin102asymptomaticindividualswith
regardtothecomplaintscolorectalclinical,from50yearsof age,inpopulationconsideredlow-risk.
Theageofthe individuals,who participatedinthe CRC
screening,showedminimumvalueof50yearsoldanda
max-imum of82years old,61.6 yearsold averageand standard
deviationof±8.1.Consideringaclassificationbyagegroup
every five years old, between 50 and 82 years old, it was
observedthattherewasnochangeinthefrequencyforthe
firstthreeagegroups,between68and82yearsold,the
fre-quencywas23.5%(IC95%:15.7–33%).
Ofthe102individuals subjectedtoscreening,42(41.2%)
belong to males and 60 (58.8%) female (x2 (accession)
95%=6.35;p=0.012).
Amongthe102individuals,whounderwentthefecaloccult
bloodtest,10(9.8%)(IC95%:4.8–17.3%),showedpositiveresult and92(90.2%)(IC95%:82.7–95.2%),showedanegativeresult. OfthetenindividualswithpositiveFOBT,06belongtomales. ToanalyzethesensitivityofFOBT,therewastheneedtouse theendoscopicresultsobtainedbyflexibleRSS.TheFOBT pre-sentedlowsensitivityof30%(IC95%:0.00–63.40%),however,
thespecificity was92.4%(IC95%:86.43–98.35%),when
con-sidered theflexibleRSSpositivefordetection ofneoplastic polypsin102individuals,admittingbeingtheflexibleRRSthe
bestmethodtodetectlesionsinthedistalcolon.TheFOBT
waseffectiveinonly2.9%(3/102)andpresentedfalse-positive resultof6.9%(7/102)(Table1).
ThedataofpositiveFOBTassociatedtotheflexibleRSS
was able to detect 5.2times more neoplastic lesions than
the negativeFOBT,demonstrated bythe Oddsratio: 5.20(IC
95%:1.21–23.16)(Table1).Therelativeriskwas3.94(IC95%: 1.20–12.89)andtheFisherexacttestresultedinp=0.057.The
associationofdataFOBT withthoseofflexibleRSSshowed
that70%ofneoplasticpolypsshowednobleeding.
Amongthe07individualswithfalse-positiveFOBT,
there-forenotassociatedwithlesionstotheflexibleRSS,therewas
a patient who, despite havingpresented the false-positive
Table1–Comparisonofthefecaloccultbloodtestwith neoplasticpolypsdetectedbyflexible
rectosigmoidoscopy.
FBOT RSS
Endoscopicfindings
Positive Negative Total
Positive 03(TP) 07(FP) 10 Negative 07(FN) 85(TN) 92 Total 10 92 102
TP,true-positive;FP, false-positive;FN, false negative; TN,true negative.
complement,was considered positiveFOBT as todigestive tract,tohavebeenitsdyspepticcomplaintsovaluedandwho demandedaninvestigation,whichdemonstratedhigh endo-scopicgastriccancerinsitu.
Amongthe10individualswithpositiveFOBT04presented polypstoflexibleRSS(Table2),amongwhom 03were
ade-nomatouspolyps,beingdiagnosed02tubularadenomasand
01villous-tubuleadenoma,allwithlowgradedysplasiaand
01inflammatorypolyp.TheFOBTpresentedpositive
predic-tivevalueof30%ofneoplasticpolyps.Among92individuals
withnegativeFOBT,11hadpolyps,being06adenomatous,01
malignityand04notneoplastic.Thepolypsassociation gen-erallywithFOBTpresentedaFischerexacttestwithp=0.04, demonstratingstatisticalsignificance.
The flexible RSS presented seven (70% [7/10])
individ-uals withassociatedinjuryto positiveFOBT and 48(52.2%
[48/92])individualswithassociatedinjurynegativeFOBT,Odds ratio=2.14(IC95%:0.52–8.79)andFisherexacttestwithresult ofp=0.23(Table2).
Theflexiblerectosigmoidoscopy presentedlesions in55
individuals(53.92%)(IC95%:43.8–63.8)andabsenceoflesions
in 47 (46.1%) (IC 95%: 36.2–56.2).Among the injured, were
detected15polyps(14.7%)(IC95%:8.5–23.1%),19 inflamma-toryprocesses(18.6%)(IC95%:11.6–27.6%)and21diverticula (20.6%)(IC95%:13.2–29.7%)(Table3).
15polypsweredetectedandremovedandafter
histopatho-logicalstudy,09adenomatous(60%);01malignity(6.7%),(IC 95%:0.2–31.9%);05non-neoplastic (33.3%),andofthese,03
wereinflammatory(20%),(95%CI:4.3–48.1%)and02
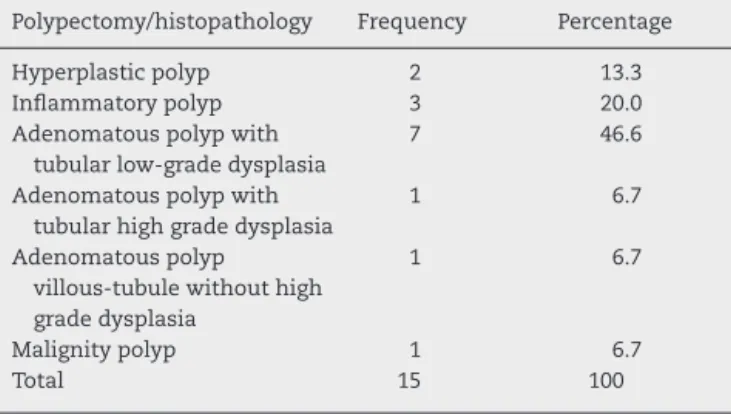
hyper-plastic(13.3%),(IC95%:1.7–40.5%)(Table4).
Ofthe15polyps,10wereneoplasticpolyps,which07were
tubular adenomatous with low dysplasia grade (46.7%) (IC
95%:21.3–73.4%);01 adenomatous villous-tubule,also with
Table3–Distributionofflexiblerectosigmoidoscopy findings.
Rectosigmoidoscopy Frequency Percentage
Normal 47 46.1
Inflammatoryprocess 19 18.6 Diverticulum 21 20.6
Polyp 15 14.7
Total 102 100.0
Table4–Globaldistributionofhistopathologicalresults
concerningpolyps.
Polypectomy/histopathology Frequency Percentage
Hyperplasticpolyp 2 13.3 Inflammatorypolyp 3 20.0 Adenomatouspolypwith
tubularlow-gradedysplasia
7 46.6
Adenomatouspolypwith tubularhighgradedysplasia
1 6.7
Adenomatouspolyp villous-tubulewithouthigh gradedysplasia
1 6.7
Malignitypolyp 1 6.7
Total 15 100
lowgradedysplasia(6.7%)(IC95%:0.2–31.9%);01tubular ade-nomatous,withhigh-gradedysplasia6.7%(IC95%:0.2–31.9%) and01adenocarcinomainsitu6.7%(IC95%;0.2–31.9%).Itwas observedthat80%ofthesepolypsweredetectedinfemales, withthediagnosisofadenomatouspolypvillous-tubulewith lowgradedysplasia.
WhenthelesionsdetectedbyflexibleRSSwereassociated with sex(Table 5), it wasobservedthat theselesions were presentin61.9%(26/42)ofmalesand48.3%(29/60)offemales (OR=1.74[IC95%:0.72–4.20]),x2yates=1.33andwithresultof
p=0.25.
When only the polyps were related to gender, it was
observed that theselesions were present in 16.67%(10/60)
of the females and 11.9% (5/42) of males (OR=1.48 [IC
95%=0.42–5.49]),x2yates=0.15andwithresultofp=0.70.
Thedistributionofneoplasticpolyps,byagegroups,with
rangeeveryfiveyears,between50and85yearsold,showed
that 60% of them were aged over 60 years old (IC 95%:
26.2–87.8%).
Thepatient inwhichthe malignity polypwasdetected,
afterpolypectomy, pathology resultsrevealedthat it wasa
flappolypwith1.3cm,coveredbymucosaoflargeintestine, displayingneoplasmofepithelialsource,characterizedbythe
Table2–Distributionoflesionsdetectedbyflexiblerectosigmoidoscopy,associatedwiththefecaloccultbloodtest.
Flexiblerectosigmoidoscopy
FOBT Normal % Inflammatoryprocess % Diverticulum % Polyp % Total %
Positivetest 3 2.94 2 1.96 1 0.98 4a 3.92 10 9.8
Negativetest 44 43.14 17 16.67 20 19.61 11b 10.78 92 90.2
Total 47 46.08 19 18.63 21 20.59 15 14.70 102 100.0
a 03adenomatouspolypsand01inflammatory.
Table5–Distributionoflesionsdetectedbyflexiblerectosigmoidoscopywithregardstosex.
Flexiblerectosigmoidoscopy
Sex Normal % Inflammatoryprocess % Diverticulum % Polyp % Total %
Male 16 15.69 9 8.82 12 11.76 5a 4.91 42 41.18
Female 31 30.40 10 9.80 9 8.82 10b 9.80 60 58.82
Total 47 46.09 19 18.62 21 20.58 15 14.71 102 10,000
a 02adenomatouspolyps,02inflammatoryand01hyperplastic.
b 07adenomatouspolyps,01malignity,01inflammatoryand01hyperplastic.
proliferation of complex tubular glands and anastomosed,
plus digitorum projections, coated by pseudo-stratified
epithelium,whosecellsrevealtheabsenceof
intracytoplas-micmucinandcoreswithtotallossofpolarity,pleomorphism, hipercromasiaandevidentnucleoli.Insuchareas,the
neopla-siainfiltratestheownlamina.Thediagnosiswasmoderately
differentiatedtubular adenocarcinomaoccurringin
villous-tubuleadenomawithhigh-gradedysplasia.Consideringthe
infiltrationofadenocarcinomainthechorion(LevelI,
Hag-gittclassification)andthe presentationofmoderate degree
ofdifferentiation, this patient,59 yearsold,wassubmitted toretossigmoidectomia,whose segmentmeasured 13cm and
revealed the absence ofresidual neoplasia in various cuts
made,absenceofmetastasisinresected23lymphnodesand
freesurgicalmargins.
Ofthe102individuals,10underwent tocolonicmucosal
biopsyandallshowednonspecificinflammatoryprocess,09
observeddiscreteintensityprocessesand01presenteda mod-erateone.
Thecolonoscopy,alsonothavingbeenaprimarytoolused
inthis screening, was held in 10 individuals withpositive
FOBT,ina61yearsoldpatient,whopresentedadenomatous
polypwithhigh degree ofdysplasiain thesigmoid and in
another58yearsoldpatient,whopresentedamalignitypolyp
insigmoid,both detectedbyflexibleRSS. Thecolonoscopy
wasalsoindicatedforthesetwopatients,consideringhigher
chanceofbeingdiagnosedpolypsinthecolonproximal
syn-chronous.
The complementary colonoscopy, performed in these
twelvepatients,detectedonlyoneadenomatouspolypwith
low-gradedysplasiainthedescendingcolon,nearthesplenic
flexure,synchronictotheothertwoadenomatouspolyps,one
withsigmoidlocationandanotherintherectum,bothwith
lowgradedysplasia,inapatientwith75yearsoldwithpositive FOBT.
Discussion
Colorectalcanceristhethirdcauseofmortalityintheworld,
mainlyintheoccident;itsincidencehasbeenshowing
ups-lope.InBrazil,intheSoutheast,theCRCisthesecondmost
frequentcancerinwomen;intheSouth,theNortheastand
the Midwest is the third most common cancer in women
andfinallyintheNorthisthefifthmostcommoncancerin
women.6
AllindividualspresentedahigherrisktodeveloptheCRC, after50yearsold,similartothatproposedforstudy inthe
literature7andsimilaryet,totheoutlineestablishedinthis study.
Inthisresearch,thecasuistryshowedafrequencyof60%of neoplasticpolypsinindividualsover60yearsold.Thisresult
isinagreementwiththeliteratureconsulted,whichshows
thehighpresenceofneoplasticlesionsinelderlyindividuals,
mostly fromthesixth decade oflife.Ageisconsidered the
mostimportantsinglefactorforthedevelopmentofpolypsin thelow-riskgroup.Althoughtheriskexistsbefore50yearsold, morethan90%ofindividualswithCRCexceededthisage, dou-blingtheriskforeachdecadeoflife,inwhichthefrequency
ofcolorectalneoplasmswashigherbetween50and70years
old,1compatiblewiththefindingsofthisresearch.
In relation to the distribution by sex, there was a
pre-dominance of the female gender (58.8%) with statistical
significance,similartothesefindingswerefoundinsimilar
research,8,9 ofwhichmorethan 50%ofindividuals
investi-gatedwerefemale.Theadhesionbetweenthegendersinthis
tracingprogramwasalsogreaterinfemales,witharesult sim-ilartothatfoundbyotherstudy,10inwhichthemalesshowed
moreresistancetoCRCscreening.
Theoccultbloodtest,giveninthisstudyasatooltodetect premalignantlesionsandcolorectalcancer,isbasedonworld literaturewhichuses,inmostscreeningprogramsforcolorectal cancer,thistypeofprocedure,althoughitisrecognizedtheir limitations.
ThepositiveFOBT,indicatingthepresenceofbleeding,also suffersinterference,whichcandistorttheresult,suchasdiet, medications,andthepresenceoflesionsthatarebleedingin anotherplacethanthecolon,aswellasthesizeofthepolyp.
Thisfindingwasmadeinthisresearch,becausethesizeof
themalignitypolypwasdetectedexceeding1cm,itsstaging
wasinitial(insitulesion)anditsmorphologyisnotulcerated,
showingnegativeFOBT.Thisfindingconfirmsthelow
sensi-tivityofthismethodfoundinthisstudy,whichhadalready
beenstatedbyothers,7,11whichfoundnegativetestswith
pos-itivelesions,inpercentagesrangingfrom35%to50%ofthe
individualsstudied.
TheFOBTsensitivityofthisstudywas30%,accordingto
datafromliterature,thatreporttobetheinitiallow
sensitiv-ity,about30–50%,althoughprogramsthatuseannualFOBT,
of long sequencing, are capable ofdetecting up to 92% of
cancers.12
Thelowsensitivityofthemethodcanresultinhigh operat-ingcost,duetothepatients,withfalse-positiveFOBT,having
toundergothemorecomplexandexpensivetests,whichwas
demonstrated in this study,that amongthe 10 individuals
thecolonoscopy,butthisfactdoesnotdiminishthechance
todetectcolorectalneoplasia,whathappenswiththe
false-negatives.2,7
AfavorablestatisticinFOBTisthehighspecificity.Inthis
studywas92.39%,whileaccordingtoanotherthathasshown
similarvalueofspecificityofthetestinaround96–98%.11
Amongthe 102 individuals studied in this research, 10
presentedthe positiveFOBTand,whencomparedwiththe
flexibleRSS,thisdetected03adenomatouspolyps,whichmay saythatthefrequencyofneoplasticlesionsdetectedby
flexi-bleRSSmembershipwithFOBTwas2.9%(3/102),comparable
tofindingresearchthatclaimstohavebeentherateof
ade-nomasinpeoplewithpositiveFOBTaround1–4%.11
ThepositiveFOBTrevealed,whencomparedwiththe
flex-ibleRSS,astrongchancetodetectneoplasticpolyps5.2times
morethanthenegativeFOBT,analyzedbyOddsratio5.20(IC
95%:−23.16to1.21),withimportantclinicalsignificance.The relativeriskwas3.94,asimilarfoundobservedonasimilar study,bysayingthattherelativeriskofneoplasiain
individ-uals withpositiveFOBT was3.47 (IC95%:2.76–4.35),when
comparedwiththosewithnegativeFOBT.13
Using the fecal occult blood test still shows
contro-versy,however,duetoitslowcost,feasibilityandforbeing
non-invasiveexamination,isstillconsideredanappropriate
methodfortracinglow-riskpopulation.
The flexible rectosigmoidoscopy was the endoscopic
instrument used in this study of colorectal cancer,taking
asargumentsbeingasimpleexam,moreaccessible,easier
attainmentbydoctorswithout the needforsedation, with
fewercomplications,andevenwithacceptablecost–benefit
tobeappliedinpopulationtracingfordetectionofprecursor lesionsoftheCRCandthecarcinomaininitialstage,besides thepossibilityofperformingthepolypectomyandthebiopsy.4
Another strong justification for its realization is that
the majority of colorectal tumors is located within reach
of rectosigmoidoscopy, as demonstrated in a study earlier
conducted.14
DuringtheflexibleRSS,heldonthisresearch, 15polyps
were detected and removed (14.71%), which were sent for
histopathologicstudy,whichidentified10neoplasticpolyps
and 05 non-neoplastic; similarity found in another study
wherepolypsdetectedbetweenarangeof2.3–12.3%.15 Thisstudyhasdetectedfalsepositivetestsin6.9%of102 individuals,withasingleFOBTandthat,whenassociatedwith theflexibleRSS,increasedsafetyandefficiencyindetecting lesionsofdistallocation.
Thedecisiontoperformthecomplimentarycolonoscopy,
afterdetectingdistalneoplasiabyflexibleRSS,shouldbe eval-uatedcase-by-case,consideringindividualovertheageof65
yearsold,histopathologicalresultshowingvillousadenoma
withsizegreaterthanorequalto1cm,mainlytheonethat
presenthighgradedysplasia,multipledistaladenomasand
personaland/orfamilyhistorypositiveforCRCduetothe pos-sibilityofdetectingsynchronicneoplasiainproximalcolon.16 Thisdecisionwasadoptedinthisstudy,threeindividualswho
underwentcolonoscopy,consideringthatthisisacasewith
polypwithhigh-gradedysplasia,anotherwithmalignitypolyp
and even another one with multipleadenomatous polyps,
withalowdegreeofdysplasia, synchronous,all locatedin
distalcolonanddetectedbyflexibleRSS.
InBrazil,theCRCscreeningdidnotsatisfactorilyachieve populationstudies,duetotheprecariousnessofthenational
healthsystem,thepoordisseminationofmethodsof
preven-tion amonghealthcareprofessionals,thehighcostofsome
requestedtestsanddemotivationofasymptomaticpatients,
tobesubjecttoendoscopicexaminationsandtoFOBT,1,4the challengesalsooccurredinthisstudywithlimitationsand dif-ficulties,whichhaveonlybeenovercomewithgreatobstinacy
ofresearchersinmakingtheprogram.
In thisstudy,53.33% ofpolypswerediagnosed asbeing
tubular adenomatous,similar findings of the study where
it wasfound53.9% tubularadenomatouspolypsofthe286
resectedpolyps.17
Amongthe102asymptomaticindividualsexamined,there
wasafrequencyof01malignitypolyp(0.98%),referred
ear-lier,andratifiedtotheresultsofsimilarstudies,wherethere
hasbeendetectionof1%and1.42%ofCRCinasymptomatic
patients.17,18Thedataofthisresearchshowthat80%of neo-plasticpolypsweredetectedinfemales,similarfactobserved bysimilarstudythatreportedthepresenceof64%of neoplas-ticpolypsinfemale,inasamplingthat57.3%of68individuals studiedbelongedtothissex.Itisnotknownthereasonofthis behavior.9
However,whentheendoscopicfindingsrefertothepolyps
in general, it was observed that there was no prevalence
betweenthegenders,evidencedbythelackofstatistical
sig-nificanceasdemonstratedintheresults.Anotherstudy got
identicalresults,inwhichthefrequencyofcolorectalpolyps wasstatisticallyequaltothetwogenders.19
Theprogressionadenoma-adenocarcinomaisrecognized
andadenomatouspolyps,whichshowvillouscomponentin
its structure,haveahigherriskofdevelopingtheCRC; this
phenomenonwasobservedinthisresearchinapatientwith
58 years old,which presented malignity polypin sigmoid,
coexisting in the same polyp villous component and high
gradedysplasia.Themosteffectivemethodforthe
diagno-sisofcolorectallesions premalignantandmalignant isthe
colonoscopy.However,forconductingapopulationscreening,
colonoscopyhasahighcost,increasedriskofcomplications
andtheneedforsedationofpatients.20
Given this,the flexible rectosigmoidoscopyis an
exam-ination accessible tomost health services, bringing, when
associatedwiththefecaloccultbloodtest,greatclinic con-tributiontocolorectalcancerscreening.
Conclusion
Basedontheresultsofthisstudy,itcanbeconcludedthatthe fecaloccultbloodtestandflexiblerectosigmoidoscopyare fea-sibleandefficienttoolswhenassociated,indetectingpolyps ingeneralandofimportantclinicalsignificanceondetection ofpremalignantandneoplasticlesionsofcolorectalcancerin
asymptomaticindividualsandlow-risk.
Conflicts
of
interest
r
e
f
e
r
e
n
c
e
s
1. BertgesER,Moraes-FilhoJPP.Câncercolorretal:rastreamento evigilância.GED.2006;25:110–8.
2. AlmeidaFFN,AraújoSEA,SantosFPS,FrancoCJCS,SantosVR, NahasSC,etal.Colorectalcancerscreening.RevHospClin FacMedSPaulo.2000;55:35–42.
3. BurtRW.Coloncancerscreening.Gastroenterology. 2000;119:837–53.
4. Habr-GamaA.Câncercolorretal–Aimportânciadesua prevenc¸ão.ArqGastroenterol.2005;42:2–3.
5. HelmJ,ChoiJ,SutphenR,BarthelJS,AlbrechtTL,ChirikosTN. Currentandevolvingstrategiesforcolorectalcancer
screening.CancerControl.2003;10:193–204.
6. INCA.EstimativadaincidênciadocâncernoBrasilem;2008. Availablefrom:http://www.inca.gov.br(accessed27.03.08). 7. AltenburgFLL,Biondo-SimõesMLP,SantiagoA.Pesquisade
sangueocultonasfezesecorrelac¸õescomalterac¸õesnas colonoscopias.RevBrasColoproctol.2007;27:
304–9.
8. DiógenesCVVN,MarianelliR,SoaresRPS,AbudRM,Falleiros V,Vilari ˜noTC,etal.Achadosderetossigmoidoscopiasno rastreamentodecâncercolorretalempacientes
assintomáticosacimade50anos.RevBrasColoproctol. 2007;27:403–7.
9. FerrariAP,RochaBP,ForonesNM.Freqüênciadepóliposem doentesoperadosdecâncercolorretal.ArqGastroenterol. 2000;37:31–4.
10.BrambillaE,DalPonteMA,BuiffonVR,FelliniRT,DalBoscoA, MayRS.Aderênciaaocontrolecolonoscópiconospacientes submetidosàressecc¸ãoendoscópicadeadenomas.RevBras Coloproctol.2006;26:249–52.
11.MorikawaT,KatoJ,YamajiY,WadaR,MitsushimaT, ShiratoryYA.Acomparationoftheimmunochemicalfecal occultbloodtestandtotalcolonoscopyintheasymptomatic population.Gastroenterology.2005;129:422–8.
12.MandelJS,BondJH,ChurchTR,SnoverDC,BradleyGM, SchumanLM,etal.TheMinnesotacoloncancercontrol study.Reducingmortalityfromcolorectalcancerbyscreening forfecaloccultblood.NEnglJMed.1993;328:1365–71. 13.LiebermanDA,HarfordWV,AhnenDJ,ProvenzaleD,Sontag
SJ,SchnellTG,etal.One-timescreeningforcolorectalcancer withcombinedfecaloccult-bloodtestingandexaminationof thedistalcolon.NEnglJMed.2001;345:555–60.
14.JucáMJ.Survivalafterresectionforadenocarcinomaofthe coloncomparisonbetweenrightandleftcolons.DisColon Rectum.2004;46:1018.
15.CrespiM,WeissmanGS,GilbertsenVA,WinawerJS,Sherlock P.Theroleofproctosigmoidoscopyinscreeningforcolorectal neoplasia.CA:CancerJClin.1984;34:158–66.
16.LevinTR,PalitzA,GrossmanS,ConellC,FinklerL,Ackerson L,etal.Predictingadvancedproximalcolonicneoplasiawith screeningsigmoidoscopy.JAMA.1999;281:1611–7.
17.ManzioneCR,NadalSR,NadalMA,MeloSVM.Análise morfológicaehistológicadepóliposcolorretaissubmetidosà ressecc¸ãoendoscópica.RevBrasColoproctol.2004;24:119–25. 18.GreegorDR.Occultbloodtestingfordetectionof
asymptomaticcoloncancer.Cancer.1971;28:131–4. 19.HossneRS,MaranhãoMF,CarvalhoFA,MendesFG.Estudo
retrospectivodoresultadoanatomopatológicode100 polipectomiascolonoscópicasrealizadasnaFMB-UNESP.Rev BrasColoproctol.2007;27:251–5.