w w w . r b o . o r g . b r
Original
Article
Biomechanical
evaluation
between
the
modified
Mason-Allen
stitch
and
the
locked
double-tie
stitch
on
the
infraspinatus
of
sheep
夽
,
夽夽
Alberto
Naoki
Miyazaki,
Marcelo
Fregoneze,
Pedro
Doneux
Santos,
Luciana
Andrade
da
Silva,
Guilherme
do
Val
Sella
∗,
Luiz
Antonio
Zanotelli
Zanella,
João
Caron
La
Salvia,
Sergio
Luiz
Checchia
DepartmentofOrthopedicsandTraumatology,SchoolofMedicalSciences,SantaCasadeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received12August2013 Accepted21October2013 Availableonline16October2014
Keywords:
Suturingtechniques Shoulder
Rotatorcuff
a
b
s
t
r
a
c
t
Objectives:Toevaluateandcomparetheinvitrobiomechanicalresultsfromtwostitches:the Mason-Allenstitch,asmodifiedbyHabermeyer;andthelockeddouble-tiestitchdeveloped atourservice,ontendonsoftheinfraspinatusmuscleofsheep.
Methods:Twentytendonsfromtheinfraspinatusmuscleofsheepwererandomlydivided intotwogroups:LDT,onwhichthelockeddouble-tiestitchwasperformed;andMA,with themodifiedMason-Allenstitch.Theevaluationwasperformedinthemechanicslaboratory, usingastandardtestmachinewithunidirectionaltraction,constantvelocityof20mmper secondanda500Nloadcell,withoutforcecycling.
Results:WeobservedthatLDTwassuperiortoMA,fortheforceneededtoformspacesof both5mm(p=0.01)and10mm(p=0.002)andalsoforthemaximumtractionresistance (p=0.003).
Conclusion:WeconfirmedourhypothesisthatLDTstitchesaresuperiortoMAstitchesfrom abiomechanicalpointofview.Thisisafurtherstitchingoptionforsurgeons,whenfragile andpoorlyvascularizedtendonsneedtobesutured,anditimprovesthequalityoffixation withoutincreasingthe“strangulation”and,consequently,theischemicarea.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
Pleasecitethisarticleas:MiyazakiAN,FregonezeM,SantosPD,daSilvaLA,doValSellaG,ZanellaLAZ,LaSalviaJC,ChecchiaSL. Avaliac¸ãobiomecânicadeovinosentreopontoMason-Allenmodificadoeopontocomduplo-lac¸obloqueadoeminfraespinal.RevBras Ortop.2014;49:630–635.
夽夽Work developed in the Departmentof Orthopedics and Traumatology, School ofMedical Sciences, Santa Casa de São Paulo,
FernandinhoSimonsenWing,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected],[email protected](G.V.Sella).
http://dx.doi.org/10.1016/j.rboe.2014.10.001
Avaliac¸ão
biomecânica
de
ovinos
entre
o
ponto
Mason-Allen
modificado
e
o
ponto
com
duplo-lac¸o
bloqueado
em
infraespinal
Palavras-chave: Técnicasdesutura Ombro
Bainharotadora
r
e
s
u
m
o
Objetivos: Avaliarecompararosresultadosbiomecânicosinvitrodedoispontos:o Mason-AllenmodificadoporHabermeyereopontoduplo-lac¸obloqueado(DLB),desenvolvidono nossoservic¸oemtendõesdemúsculosinfraespinaisdeovinos.
Métodos: Vintetendõesdomúsculoinfraespinaldeovinosforamdivididosaleatoriamente emdoisgrupos:oDLB,noqualfoiconfeccionadoopontoduplo-lac¸obloqueado;eoMA, comopontoMason-Allenmodificado.Aavaliac¸ãofoifeitanolaboratóriodemecânica,com umamáquinadetestepadrão,detrac¸ãounidirecional,comvelocidadeconstantede20mm porsegundo,comumacéluladecargade500N,semciclagemdeforc¸a.
Resultados: EvidenciamosumasuperioridadedoDLBsobreoMA,tantonaforc¸anecessária paraformar5mmde espac¸o(p=0,01)como 10mm(p=0,002)etambém naresistência máximadetrac¸ão(p=0,003).
Conclusão: Confirmamosnossahipótesedequeoponto comDLBésuperioraoMAdo pontodevistabiomecânico.Essaémaisumaopc¸ãodepontoparaocirurgião,quando precisasuturartendõesfrágeisepoucovascularizados,emelhoraaqualidadedafixac¸ão semaumentaro“estrangulamento”e,consequentemente,aáreaisquêmica.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Suturingofrotator cuffinjuries(RCIs)isoneofthe biggest challengesforshouldersurgeons.Therearehighdehiscence rates,especiallyinrelationtoextensiveinjuries,andthe inci-dencecanrangefrom13%to94%ofthecases.1,2
Theaimofsurgicaltreatmentistomechanicallyproduce afirmandsecuresutureofthetendonatitsinsertionsiteso thathealingcantakeplace.Thesurgicalmaterialsusedare todayhighlyreliableandforthisreason,accordingto Cum-mins,themajorcauseofrepairfailureistheinterfaceofthe suturethreadwiththetendon.3Gerberetal.4suggestedthat
theidealrepairshouldwithstandahightractionforceduring theinitialperiodoffixation,enableformationoftheminimum spacebetweenthetendonandboneandmaintain mechani-calstabilityuntilhealingtakesplace.Thetypeofstitchused forthesutureisacrucialpartofthesuccessorfailureofthe surgicalprocedure.
ArthroscopicRCIrepairsrequirearefinedoperative tech-niqueandknowledgeandskillonthepartofthesurgeonin ordertopassthethreadthroughthetendon.Thesuturingcan beperformedusing differenttypesofstitches,which were developedtowithstandtractionforceswithoutundoingthe tendonrepair.5TheMason-Allenstitchisthemostresistant
type.4Itcanbeperformedarthroscopicallyandisthenknown
asthemodifiedMason-Allenstitch,asdescribedbyScheibel andHabermeyer.6
Withregardtotendonsuturingperformedasanopen pro-cedure,thetechniquedevelopedbyKrackowetal.7isgenerally
recognizedasthemostresistantandsecure method,butit isalmostimpossibletoperformitarthroscopically.Moreover, becauseitinvolvesstitchesthataretransversetothedirection ofthetendon,itmaycompromisethevascularizationofthe tendonandthusthehealingoftheinjury.
BasedontheLasso-LoopstitchdescribedbyLafosseetal.,8
the seniormember ofourgroup(SLC) sought todevelopa techniquethatcouldbecombinedwiththeresistanceofthe suturedevelopedbyKrackowetal.7andwhichcouldbe
per-formedarthroscopicallywhileonlyminimallycompromising thevascularization.Thisnewtechniqueisperformedusing doubly locked longitudinal stitches, which we have name lockeddouble-tie(LDT)stitches.
In additionto describingthetechnique forconstructing LDTstitches,doneonthetendonoftheinfraspinatusmuscle ofsheep,wecompareitbiomechanicallywiththemodified Mason-Allenstitch,whichisconsideredtobethemost resis-tantmethodperformedarthroscopically.6
Thisstudyusinganimalswasapprovedbyourinstitution’s ethicscommittee.
Materials
and
methods
Surgicaltechnique
TheLDTstitchissimples,butlikealltechniques,itneedsto bepracticedandassistantsneedtobetrained.Useofknotless anchorsfacilitatesconstruction ofthesestitchesbutisnot essential.Thesixstepsinmakingthesestitchesareasfollows: First: Afterplacingthe sutureanchor intheappropriate position, usinganarthroscopic suturingneedle, oneofthe endsofthethreadispassedthroughthetendonfromthe artic-ulartothesubacromialface,approximately20mmmedially tothelateralborderofthetendon,closetothemuscle–tendon transition.Thethreadshouldrunthroughtheanchorandnot betrapped(Fig.1A).
Fig.1–Sequenceofstepsforconstructingthelockeddouble-tiestitch.(A)Firstpassageofthesuturingthreadfromthe articularfacetothesubacromialface.(B)Formationofthefirstloop(subacromialface).(C)Passageofthesubacromialthread throughtheloopthatwasmadepreviously.(D)Tensioningthelowerthread,thuslockingthefirstpartofthesuture.(E) Formationofthesecondloop,approximately10mmfromthelateralextremityofthetendon.(F)Passageoftheacromial threadthroughthissecondloop.(G)Tensioningofthelowerthread,thuslockingthesecondpartofthesuture.(H)
Performingthesamestitchwiththeotherthreadontheanchor.(I)Finalappearanceofthestitch,showinghowitisparallel tothebloodirrigationofthetendon.
thesamethread,leavingaloopfromthearticularfacetothe subacromialface(Fig.1B).
Third:Theendofthethreadthatisinthesubacromialspace ispassedthroughthisloop.Atthistime,thelowerthreadis tensioned,whichthuslocksthefirstpartofthesuture(Fig.1C andD).
Fourth:Anewloopismadeapproximately10mmfromthe lateralextremityofthetendon(Fig.1E).
Fifth:Theendofthisthreadispassedthroughthisnewloop (Fig.1F).
Sixth:Thestitchisthentightenedusingnonslipknotsand thelesionisclosed(Fig.1G).
With a suturing anchor loaded with two thread, two stitchescanbeconstructedandthesutureresistancecanbe furtherincreased(Fig.1HandI).
Biomechanicalevaluation
In previous experimental studies, it was established and demonstratedthatthetendonoftheinfraspinatusmuscleof sheephascharacteristicssimilartothoseofthesupraspinatus
ofthehumanshoulderandservesasamodelforstudieson rotatorcuffdiseases.9,10
TwentytendonsoftheinfraspinatusmuscleofmaleTexel sheepaged1.5–2yearswereusedinthisstudy.Thesewere randomlydividedinto twogroups:LDT,inwhichthestitch describedabovewasconstructed(Fig.2A);andMA,inwhich the modifiedMason-Allenstitch6 wasconstructed(Fig. 2B).
Fig.2–(A)Lockeddouble-tiestitchand(B)modifiedMason-Allenstitch.
wassubjectedtoaninitialloadof30Nfor60stopretensionthe suture.Thetractiondevicehadascalemarkedinmillimeters andthiswasusedtoobservetheforceneededtoform dis-placementsof5mmand10mmandthemaximumforcethat thesamplewithstood.Thecausesofthefailureswere also noted(Fig.3).
The evaluation was done in the mechanics laboratory, usinga standard testmachine withunidirectionaltraction (MTS;Qtestmodel),ataconstantvelocityof20mmper sec-ond,withaloadcellof500Nandwithoutcyclingoftheforce applied.
Fig.3–Layoutofthestitchesandtestplatform.
Statisticalassessment
Descriptiveanalysiswasperformedinrelationtothespaces of5mmand10mmandthemaximumforcemeasuredineach typeofstitch.Afteralloftheadherenceshadbeenchecked, theirequalityofvariancewastestedforeachpairofvariables (measuredinbothtypesofstitch),bymeansoftheFisherF test.
TheStudentttestwasthenusedonthevariablesofweight, widthandthicknesstoascertaintheequalitybetweentheir means,andonthevariablesof5mmspace,10mmspaceand maximumforce,toinvestigatewhetherthemeansobtained fromusingtheLDTstitchweresuperiortothoseobtainedfrom usingtheMAstitch.
Forallthetests,thesignificancelevelusedwas5%.Thus, thehypothesesinwhichthedescriptivelevels(p-values)were <0.05wererejected.
Results
Table 1 presents the mean, standard deviation (SD) and
minimum, medianand maximumvaluesobtainedforeach variableandforeachtypeofstitchused.
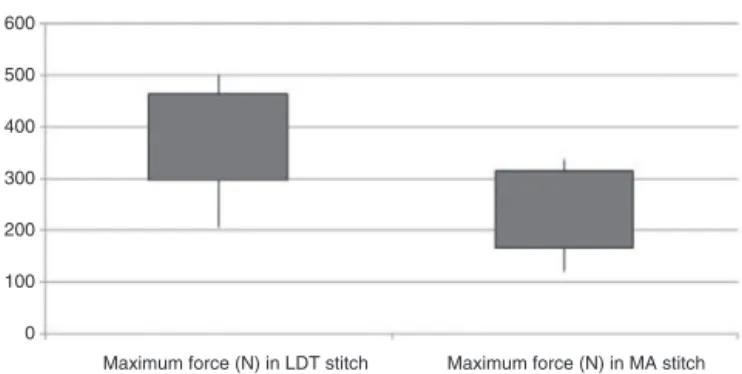
Tocomparethe5mmspace,10mmspaceandmaximum force ofthe twogroups, anF testwas firstlyperformedto collatethevariances.Thehypothesisthatthemeansforthe variables of5mm, 10mmand maximum force inthe LDT stitchgroupwereatmostequaltothemeansintheMAstitch groupwasthentestedusingtheStudentttest.Fromthis,it wasconcludedthatthemeansforthesevariablesintheLDT stitchgroupweresuperiortothoseoftheMAgroup,atthe significancelevelof5%(Figs.4–6).
Discussion
450 400 350 300 250 200 150 100 50 0
Force (N) needed to form 5 mm space, in LDT stitch
Force (N) needed to form 5 mm space, in MA stitch
Fig.4–Differenceinforceneededtoforma5mmspace,
betweenthegroups.
450 500
400 350 300 250 200 150 100 50 0
Force (N) needed to form 10 mm space, in LDT stitch
Force (N) needed to form 10 mm space, in MA stitch
Fig.5–Differenceinforceneededtoforma10mmspace,
betweenthegroups.
betweenthetendonedgesandthebonebedandmaintain sta-bilityuntiltheinjuryhashealed.4Throughstableandresistant
suturing,muscle–tendon–boneunionwillagainbeachieved afterhealing.
Afterlargenumbersofcasesofrepeatedtearinghadbeen observed,especiallyin situationsofextensive injury, inter-estindevelopingnewtechniquestoimprovetheresultsfrom theseoperationsincreased.11–13 Recentstudieshaveshown
thatthekeypointinmaintainingthesemechanicalproperties istheinterfacebetweenthesutureandthetendon.3,4,6,9,10,14
500 600
400
300
200
100
0
Maximum force (N) in LDT stitch Maximum force (N) in MA stitch
Fig.6–Differenceinmaximumforcebetweenthegroups.
Consequently, several types of arthroscopic stitches have been described, going from very simple ones to U-shaped stitches, modified Mason-Allen stitches,4 Mac-Stitch14 and
Lasso-Loop,8allwiththeaimofincreasingtheresistanceof
thefixation.
Webelievethatbetterhealingisdirectlyrelatedtobetter vascularizationoftherotatorcuffthatistoberepaired,and consequentlytolessareaofischemia.Asshownbyanatomical studies,themicrovascularizationofthisstructureisoriented paralleltoitstendonfibersandprogressesfrommedialto lat-eral,withalessvascularizedareaintheregionofthetendonof thesupraspinatusmuscle(Codman’scriticalarea).15,16Thus,
stitchesconstructedtransversallytothedirectionof vascu-larization willresultingreaterischemicarea andtherefore increasethechanceofrepeatedtearing.Thisdoesnotoccur withLDTstitches,becausetheyareparallelandrespectthe vascularizationofthetendon(Fig.1I).
With the aim of comparing the new stitch that we
developed (LDT) with the Mason-Allen stitch modified by Habermeyer, otherfactors thatcould alterthe resultsfrom thesampleswereexcluded,forexamplefailurerelatingtothe tendon–boneinterface(poorbonequality,positioningerrors, directionality,looseningandevencuttingofthesuturethread attheopeningsoftheanchors).Thus,withthesheeptendon model, we were able to isolate and individually evaluate each stitch with regard to the force required to produce
Table1–Distributionofthevariables.
Variable Stitch Mean SD Minimum Median Maximum pvalue
Age(years) LDT 1.6 0.211 1.5 1.5 2.0
MA 1.5 0.00 1.5 1.5 1.5
Weight(kg) LDT 22.46 1.226 20.4 22.3 24.5 0.280
MA 22.62 1.783 20.3 22.1 25.2
Width(mm) LDT 17.65 1.658 14.9 17.8 20.0 0.536
MA 17.15 1.34 14.20 17.15 19.0
Thickness(mm) LDT 3.5 0.638 2.4 3.5 4.4 0.679
MA 3.78 0.553 2.8 3.7 4.7
Forcetoform5mmspace(N) LDT 286.6 64.1 183 301 392 0.010
MA 203.3 80.5 73.5 209.3 315.5
Forcetoform10mmspace(N) LDT 341.9 87.8 180 345.5 474.3 0.002
MA 219.7 81.8 68.6 241 300
Maximumspace(N) MA 246.7 83.6 121.4 287.1 335.9
displacementsof5mmand10mmandthemaximumload neededforthesampletofail.
UnlikePonceetal.,17wedidnotcutthetendons
longitudi-nally,becausetheirphysicalconformitywasmoreconsistent in the more proximal part of the spine of the scapula, but we obtained a smaller number of samples. We dis-tributedthestitchesonoursamplesandimaginedusingan anchor.Thus,twoLDTstitcheswereconstructedforeveryMA stitch.
OurresultsshowedthattheLDTwassuperiortotheMA stitch, bothregardingthe force requiredto formspaces of 5mmand10mmandregardingthemaximumtraction resis-tance.Thisconfirmedourhypothesisandmakesthisstitchan optionforsuturinginrotatorcuffsurgery.Weobservedduring thetestthattheMAstitchesresultedin“strangulation”ofthe tendon,whichisbadinrelationtoitsvascularization.Thisdid notoccurwiththeLDTstitches.
Incomparingourmaximumloadresultswiththeresults fromotherbiomechanicalstudiesonsheep,weobservedthat theLDTstitcheswithstoodgreaterforcebeforesamplefailure occurred.However,wedidnotperformcyclingoftheforce applied,asdescribedbyBurkhartetal.,18whichisan
impor-tantlimitationofourstudy andimpedesmoretrustworthy comparisons.
It is evident that biological factors are fundamentally importantinrepairingrotatorcuffinjuries,butthesewerenot anobjectiveofthepresentstudy.
Conclusion
We confirmed our hypothesis that LDT stitches are supe-rior to MA stitches from a biomechanical point of view. LDT stitches are an additional option for surgeons when fragile tendons with poor vascularization need to be sutured. They improve the quality ofthe fixation without increasing the strangulation and consequently the area of ischemia.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. MiyazakiAN,FregonezeM,DoneuxPS,etal.Avaliac¸ãodos
resultadosdasreoperac¸õesdepacientescomlesõesdo
manguitorotador.RevBrasOrtop.2011;46(1):45–50.
2.BoileauP,BrassartN,WatkinsonDJ,CarlesM,HatzidakisAM,
KrishnanSG.Arthroscopicrepairoffull-thicknesstearsofthe
supraspinatus:doesthetendonreallyheal?JBoneJointSurg
Am.2005;87(6):1229–40.
3.CumminsCA,MurrellGA.Modeoffailureforrotatorcuff
repairwithsutureanchorsidentifiedatrevisionsurgery.J
ShoulderElbowSurg.2003;12(2):128–33.
4.GerberC,SchneebergerAG,BeckM,SchlegelU.Mechanical
strengthofrepairoftherotatorcuff.JBoneJointSurgBr.
1994;76(3):371–80.
5.YamaguchiK,LevineWN,MarraG,GalasLM,KleppsS,Flatow
E.Transitioningtoarthroscopicrotatorcuffrepair:thepros
andcons.JBoneJointSurgAm.2003;85:144–55.
6.ScheibelMT,HabermeyerP.AmodifiedMasonAllen
techniqueforrotatorcuffrepairusingsutureanchors.
Arthroscopy.2003;19(3):330–3.
7.KrackowKA,ThomasSC,JonesLC.Anewstitchfor
ligament–tendonfixation.JBoneJointSurgAm.
1986;68(5):764–6.
8.LafosseL,RaebroeckxAV,BrzoskaR.Anewtechniqueto
improvetissuegrip:“Thelasso-loopstitch”.Arthroscopy.
2006;22(11):e1–3,1246.
9.GerberC,ScheneebergAG,PerrenSM,NyffelerRW.
Experimentalrotatorcuffrepair.Apreliminarystudy.JBone
JointSurgAm.1999;81(9):1281–90.
10.SileoMJ,RuotoloCR,NelsonCO,Serra-HsuF,PanchalAP.A
biomechanicalcomparisonofthemodifiedMason-Allen
stitchandmassivecuffstitchinvitro.Arthroscopy.
2007;23(3):235–40.
11.BurkhartSS,DanaceauSM,PearceCEJr.Arthroscopicrotator
cuffrepair.Analysisofresultsbytearsizeandbyrepair
technique:marginconvergenceversusdirecttendon-to-bone
repair.Arthroscopy.2001;17(9):905–12.
12.MaCB,MacGillivrayJD,ClabeauxJ,LeeS,OtisJC.
Biomechanicalevaluationofarthroscopicrotatorcuff
stitches.JBoneJointSurgAm.2004;86(6):1211–6.
13.SchneebergerAG,RollAV,KalbererF,JacobHA,GerberC.
Mechanicalstrengthofarthroscopicrotatorcuffrepair
techniques.JBoneJointSurgAm.2002;84(12):2152–60.
14.MacGillivrayJD,MaCB.Arthroscopicstitchformassiverotator
cufftears:theMacstitch.Arthroscopy.2004;20(6):669–71.
15.YepesH,Al-HibishiA,TangM,MorrisSF,StanishWD.
Vascularanatomyofsubacromialspace:amapofbleeding
pointsforthearthroscopicsurgeon.Arthroscopy.
2007;23(9):978–84.
16.LohrJF,UhthoffHK.Thevascularpatternofthesupraspinatus
tendon.ClinOrthopRelatRes.1990;254(1):35–8.
17.PonceBA,HosermannCD,RaghavaP,TateJP,EberhardtAW,
LafosseL.Biomechanicalevaluationof3arthroscopic
self-cinchingstitchesforshoulderarthroscopy.AmJSport
Med.2011;39(1):188–94.
18.BurkhartSS,DiazPaganJL,WirthMA,AthanasiouKA.Cyclic
loadingofanchor-basedrotatorcuffrepairs:confirmationof
thetensionoverloadphenomenonandcomparisonofsuture
anchorfixationwithtransosseousfixation.Arthroscopy.