w w w . r b o . o r g . b r
Case
Report
Charcot
neuroarthropathy:
realignment
of
diabetic
foot
by
means
of
osteosynthesis
using
intramedullary
screws
–
case
report
夽
,
夽夽
Alexandre
Leme
Godoy
dos
Santos
∗,
Rômulo
Ballarin
Albino,
Rafael
Trevisan
Ortiz,
Marcos
Hideyo
Sakaki,
Marcos
de
Andrade
Corsato,
Tulio
Diniz
Fernandes
InstituteofOrthopedicsandTraumatology,HospitaldasClínicas,MedicalSchool,UniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received13August2013 Accepted15October2013 Availableonline28August2014
Keywords:
Charcotjoint Arthrodesis Diabetes Plantigradefoot
a
b
s
t
r
a
c
t
Diabetesmellitusisaseriousdiseasethataffectsalargeportionofthepopulation.Charcot neuroarthropathyisoneofitsmajorcomplicationsandcanleadtoosteoarticular defor-mities,functionalincapacity,ulcersandankleandfootinfections.Realignmentofthefoot bymeansofarthrodesispresentsahighrateofimplantfailureduetoweight-bearingon aninsensitivefoot.Theaimofthisreportwastodescribesuccessfuluseofintramedullary osteosynthesiswithcompressionscrewstostabilizethedeformedfoot,inadiabeticpatient withneuroarthropathy.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Neuroartropatia
de
Charcot:
realinhamento
do
pé
diabético
por
meio
de
osteossíntese
com
parafusos
intramedulares
–
relato
de
caso
Palavras-chave:
Articulac¸ãodeCharcot Artrodese
Diabetes Péplantígrado
r
e
s
u
m
o
Odiabetesmellituséumadoenc¸agravequeafetaumagrandeparceladapopulac¸ão.A neu-roartropatiadeCharcotéumadasgrandescomplicac¸õesquepodemlevaradeformidades osteoarticulares,incapacidadefuncional,úlceraseinfecc¸ãonotornozeloenopé.O realin-hamentodopépormeiodeartrodesesapresentaelevadoíndicedefalhadoimplantepor causadadescargadepesoemumpéinsensível.Oobjetivodesterelatodecasoé descr-everousobem-sucedidodeosteossínteseintramedularcomparafusosdecompressãopara estabilizac¸ãodopécomdeformidadeempacientediabéticocomneuroartropatia.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevierEditora Ltda.Todososdireitosreservados.
夽
Pleasecitethisarticleas:dosSantosALG, AlbinoRB,OrtizRT,Sakaki MH,deAndradeCorsato M.Neuroartropatia deCharcot: realinhamentodopédiabéticopormeiodeosteossíntesecomparafusosintramedulares–relatodecaso.RevBrasOrtop.2014;49(5):535–9.
夽夽
WorkdevelopedbytheFootandAnkleSurgeryGroup,InstituteofOrthopedicsandTraumatology,HospitaldasClínicas,Medical School,UniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](A.L.G.Santos).
http://dx.doi.org/10.1016/j.rboe.2014.08.006
Introduction
Thereare285milliondiabeticsworldwide,representing6.6% of the population aged 20–79 years. Of these, up to 2.5% develop Charcot neuroarthropathy at some stage of the disease.1Thiscomplicationmostfrequentlyinvolvesthe
mid-foot and it resultsinosteoarticular deformities,significant functionalloss,increasedriskofulcersandlocalinfection.2
Theidealtreatment protocol continues tobea topic of debate in the literature. A recent survey by the American OrthopedicFootandAnkle Society revealedthattreatment ofthedeformitiesresultingfromCharcotneuroarthropathy is one ofthe two most controversialproblems within the specialty.3
Controversystillexistsregardingwhatthebesttreatment optionshouldbeandhasgivenrisetointensedebateinpapers publishedwithinthespecialty.4–8
Withregardtochoosingsurgicaltreatment,themajor dis-cussionisinrelationtothebesttechniqueforreestablishing theanatomyoftheplantigradefootanddiminishing recurr-encesofdeformities,ulcersandinfection.Thus,thetypeof implantusedtostabilizethe arthrodesisofthe medialand lateralcolumnsofthefootisanimportantfactor.
External fixators show potential disadvantages, with higherratesofsuperficialinfectionandnon-consolidation.9
Dynamiccompressionplatesorplateswithangular stabil-itypresentthreedisadvantages:greateraggressiontowardsoft tissues,higherosteosynthesisfailureratesandhigherratesof non-consolidation.10
Useofcorticalscrewsinthesecasesfrequentlypresents thecomplicationofperi-implantfracturing,mainlyduetolow bonemineraldensityandtheveryacuteangleofentryintothe boneinthemidfootregion.7–10
Intramedullaryscrewsforstabilizingthemedialandlateral columnsareapromisingalternativeforincreasingthesuccess rateofthissurgicalprocedure.2,7,10
Case
report
Thepatientwas35-year-oldwomanwhohadpost-gestational diabetesfor20yearsandwasusinginsulin.Shefirstcameto
Fig.1–(A)Plantarappearanceofthefootatthefirst consultation;(B)plantarappearanceofthefootafterserial debridementanduseoffullcontactplastercast.
ourclinictwoyearsbeforethetimeofthepresentreport,with ahistory ofpain inherleft foot,andshenowpresenteda plantarulceronthemidfootthathadbeenevolvingforfour months.
In the initial examination, she presented pain, edema, hyperemiaandtemperatureelevatedby4◦Cincomparison
withthecontralateralsideinthemidfootregion,associated withasuperficialulcerof2cmindiameterontheplantarface ofthemidfoot(Fig.1AandB).Investigationofplantar sensi-tivitybymeansofthemonofilamenttestshowedthepresence ofperipheralneuropathy.Vascularexaminationshowedthat thepulsewasnormal.Aprobe-to-bonetestwasnegative.
The initial radiographic evaluation revealed loss of the usualboneanatomyofthemidfoot,withbonefragmentation intheregionofthetarsometatarsaljointandalterationofthe talus-firstmetatarsalanglesseeninanteroposteriorand lat-eralview,alongwithplantarboneprominenceinthemidfoot (Fig.2AandB).
Table1–Eichenholtzclassification.5,6
Stage Clinicalcharacteristics
0 Initialpresentation Pre-fragmentation Acuteinflammatoryphase:edematous,erythematous,hotand
hyperemicfoot
I AcuteCharcot Fragmentationordevelopment Periarticularfracture,developmentofjointsubluxation,riskof
instabilityanddeformity
II SubacuteCharcot Coalescence Reabsorptionofbonedebris,homeostasisofsofttissues
III ChronicCharcot Consolidationorreparation Boneorfibrousstabilizationofdeformityrepair
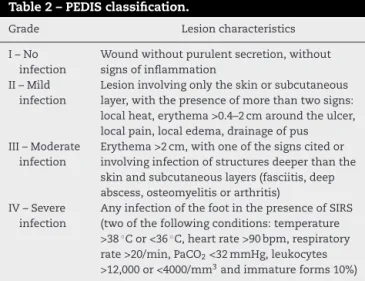
Basedonthesefindings,thehypothesisraisedconsisted ofdiabetic footsyndromeinassociationwithCharcot neu-roarthropathy of stage II of the Eichenholtz classification system(Table1)andcutaneousulceroftypeIIofthePEDIS classificationsystem(perfusion;extent;depth;infection;and sensation)(Table2).
Theinitialtreatmentconsistedofserialdebridementofthe devitalizedtissuesontheborderofthecutaneouslesionevery sevendaysandprotectionagainstloadingbymeansofa full-contactplastercast,untilthe cutaneouslesionhad closed, whichtooksixweeks(Fig.1B).
Duringthe second phaseofthe treatment,foot realign-mentwasplanned,withrestitutionofthebonerelationships bymeansofextendedtriplearthrodesisandosteosynthesis usingintramedullarycannulatedscrews.
Thesurgerywasperformedwiththe patientin horizon-taldorsaldecubitus.Theanestheticmethodusedwasspinal anesthesiacombinedwithsedation.
Apneumatictourniquetat300mmHgwasusedontheleft lowerlimbafterdrainingtheveinsbymeansofanEsmarch bandage.
An extended suprafibular lateral access and a medial accesswere used. Thelateral accesswas used to perform dissectionofthesubcutaneouslayeranddeinsertionofthe musculatureoftheshortextensormuscles,inordertogain accessto, performdecortication on and realignthe lateral
Table2–PEDISclassification.
Grade Lesioncharacteristics
I–No infection
Woundwithoutpurulentsecretion,without signsofinflammation
II–Mild infection
Lesioninvolvingonlytheskinorsubcutaneous layer,withthepresenceofmorethantwosigns: localheat,erythema>0.4–2cmaroundtheulcer, localpain,localedema,drainageofpus III–Moderate
infection
Erythema>2cm,withoneofthesignscitedor involvinginfectionofstructuresdeeperthanthe skinandsubcutaneouslayers(fasciitis,deep abscess,osteomyelitisorarthritis)
IV–Severe infection
AnyinfectionofthefootinthepresenceofSIRS (twoofthefollowingconditions:temperature >38◦Cor<36◦C,heartrate>90bpm,respiratory rate>20/min,PaCO2<32mmHg,leukocytes
>12,000or<4000/mm3andimmatureforms10%)
Source:Directricespanamericanasparaeltratamientode infec-cionesenúlcerasneuropáticasdelasextremidadesinferiores.Rev PanamInfectol.2011;13(1Suppl.1):S4.
surfacesofthesubtalar,calcaneocuboidandtarsometatarsal joints.Themedialaccesswasusedtoapproachthe talonavic-ular,navicular-medialcuneiformandmedialcuneiform-first metatarsaljoints.Afterachievingrealignmentandprovisional stabilizationusingKirschnerwires,thepositionwaschecked bymeansofradioscopiccontrol(Fig.3AandB).
Thedefinitiveosteosynthesisofthesubtalarjointwas per-formedusinganAccutrak® Plusscrew;the
calcaneocuboid-fourthmetatarsaljointusinganAccutrak®6/7screw;andthe
talonavicular-medialcuneiform-firstmetatarsaljointusingan Accutrak®6/7screw.
Afterfixation, weperformedpercutaneous tenotomyon theshortextensortendonsofthesecondtofifthtoes.
Thepatientwaskeptwithoutweight-bearingfor30days aftertheoperation.Afterthisdate,shebegantoprogressively applyweight,usingabracefromthesuralareatothefoot,and shestartedphysiotherapyforgaittraining.
Ninetydaysafterthesurgery,shestartedtoapplyherfull weight,whilestillusingabrace,whichshecontinuedtouse untilcompleting120daysaftertheoperation.
Twelvemonthsaftertheoperation,the patientwasfree fromcomplaints,couldwalkwithouttheaidofcrutches,had awell-definedmediallongitudinalarchandpresented pre-servedhindfootandforefootalignment(Fig.4A–C).
Controlradiographsproduced12 monthsafterthe oper-ationshowedatalus-firstmetatarsalangleof6◦ anddorsal
displacementof3mm(Fig.5A–C).
Fig.3–Intraoperativecontrolradioscopytocheckthe provisionalstabilization:(A)lateralviewshowing
Fig.4–Clinicalphotosofthepatientshowingthefootalignment12monthsaftertheoperation:(A)posteriorimageofthe footshowingthehindfootrealignmentachieved;(B)medialimageofthefootshowingtherealignmentbetweenthe hindfootandmidfoot;(C)imageoftheplantarregionofthefootshowingtheachievementofaplantigradefoot.
Fig.5–Radiographiccontrol12monthsaftertheoperation:(A)lateralviewofthefootshowingevidenceofcorrectionofthe alignmentoftheaxisofthetaluswiththefirstmetatarsal;(B)anteroposteriorviewofthefootshowingmaintenanceofthe alignmentofthescrewsandthealignmentoftheaxisofthetaluswiththefirstmetatarsal;(C)anteroposteriorviewofthe ankleshowingmaintenanceofthetibiotalarjoint.
Discussion
Theclinicalandradiographicresultsweresatisfactoryafter12 monthsoffollow-up.
Surgical reconstruction ofthe midfootcollapse has the aimofreestablishingaplantigradefootwithoutplantarbone prominences, so that the plantar pressure will be better distributedandulcers,infectionandamputationwillbe pre-vented.
Restoration of the alignment of the medial and lateral columnsofthefootusingintramedullaryscrewstotreat Char-cotneuropathyinthemidfoothasbeendescribedinpublished caseseries.2,3,7–9
Thisoptionforosteosynthesishasbiomechanical advan-tages,sinceit hasthe objectives ofincreasingthe consoli-dationrate,diminishingthedehiscence/infection ratesand avoidingfailureoftheimplantmaterial.
Patientswithdiabeticneuropathyhavedifficultiesin bal-ancingandincontrollingtheirweightplacementonthelower limbs.Thus,intramedullaryimplantspresentbiomechanical advantagesinrelationtoextramedullaryimplants.1
Someauthorshaveadvocatedusingmassivescrewsinthis surgicaltechnique.However,thescrewimplantusedinthe presentcasereportwascannulated.
Therearestillnoinvivocomparativestudiesonthe differ-entimplantsavailable.
We conclude that use of cannulated screws with-out heads is a viable procedure for intramedullary fixa-tion of foot realignment in treating Charcot neuroarthro-pathy.
Studydesignswithhigher-gradeevidenceareneededin ordertodefinetreatmentprotocolswithappropriate recom-mendationlevels.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.InternationalDiabetesFederation.WorldDiabetesCongress Dubai,4Decemberto8December2011.Availablefrom:
http://www.idf.org[accessed12.03.12].
2.WiewiorskiM,ValderrabanoV.Intramedullaryfixationofthe medialcolumnofthefootwithasolidboltinCharcot midfootarthropathy:acasereport.JFootAnkleSurg. 2012;51(3):379–81.
3.AssalM,SternR.Realignmentandextendedfusionwithuse ofamedialcolumnscrewformidfootdeformitiessecondary todiabeticneuropathy.JBoneJointSurgAm.
4. FriggA,PagenstertG,SchäferD,ValderrabanoV,Hintermann B.Recurrenceandpreventionofdiabeticfootulcersafter totalcontactcasting.FootAnkleInt.2007;28(1):64–9.
5. SimonSR,TejwaniSG,WilsonDL,SantnerTJ,DennistonNL. Arthrodesisasanearlyalternativetononoperative
managementofCharcotarthropathyofthediabeticfoot.J BoneJointSurgAm.2000;82(7):939–50.
6. LammBM,GottliebHD,PaleyD.Atwo-stagepercutaneous approachtoCharcotdiabeticfootreconstruction.JFootAnkle Surg.2010;49(6):517–22.
7. GrantWP,Garcia-LavinS,SaboR.Beamingthecolumnsfor Charcotdiabeticfootreconstruction:aretrospectiveanalysis. JFootAnkleSurg.2011;50(2):182–9.
8.AssalM,RayA,SternR.Realignmentandextendedfusion withuseofamedialcolumnscrewformidfootdeformities secondarytodiabeticneuropathy:surgicaltechnique.JBone JointSurgAm.2010;92(Suppl.1Pt1):20–31.
9.SammarcoVJ,SammarcoGJ,WalkerEWJr,GuiaoRP. MidtarsalarthrodesisinthetreatmentofCharcotmidfoot arthropathy:surgicaltechnique.JBoneJointSurgAm.2010;92 Suppl.1Pt1:1–19.
10.KitaokaHB,AlexanderIJ,AdelaarRS,NunleyJA,MyersonMS, SandersM.Clinicalratingsystemsfortheankle–hindfoot, midfoot,hallux,andlessertoes.FootAnkleInt.