www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Endoscopic
repair
of
cerebrospinal
fluid
rhinorrhea
夽
Vladimir
Kljaji´
c
a,b,
Petar
Vulekovi´
c
a,c,
Ljiljana
Vlaˇ
ski
a,b,
Slobodan
Savovi´
c
a,b,
Danijela
Dragiˇ
cevi´
c
a,b,∗,
Vladimir
Papi´
c
a,caUniversityofNoviSad,FacultyofMedicine,HajdukVeljkova,NoviSad,Serbia bClinicalCenterofVojvodina,ENTClinic,HajdukVeljkova,NoviSad,Serbia
cClinicalCenterofVojvodina,ClinicofNeurosurgery,HajdukVeljkova,NoviSad,Serbia
Received29February2016;accepted14April2016 Availableonline4June2016
KEYWORDS
Cerebrospinalfluid rhinorrhea; Nasalsurgical procedures; Endoscopy; Fistula; Fluorescein; Treatmentoutcome
Abstract
Introduction:Nasalliquorrheaindicatesacerebrospinalfluidfistula,anopencommunication between the intracranial cerebrospinal fluid and thenasal cavity. Itcan be traumaticand spontaneous.
Objective:Theaimofthisstudywastoassesstheoutcomeofendoscopicrepairofcerebrospinal fluidfistulausingfluorescein.
Methods:Thisretrospectivestudyincluded30patientsofbothsexes,withameanageof48.7 years,treatedintheperiodfrom2007to2015.Allpatientsunderwentlumbaradministration of5%sodiumfluoresceinsolutionpreoperatively.Fistulawasclosedusingthree-layergraftand fibringlue.
Results:Cerebrospinalfluidfistulaswerecommonlylocatedintheethmoid(37%)andsphenoid sinus(33%).Mostpatientspresentedwithtraumaticcerebrospinalfluidfistulas(2/3ofpatients). Thereportedsuccessrateforthefirstrepairattemptwas97%.Complicationsoccurredinthree patients:onepatientpresentedwithacutehydrocephalus,onewithreversibleencephalopathy syndromeon the fifth postoperative day withbilateral lossof vision, andone patient was diagnosedwithhydrocephalustwoyearsaftertherepairofcerebrospinalfluidfistula.
Conclusion:Endoscopic diagnosis and repair ofcerebrospinal fluid fistulas using fluorescein intrathecallyhashighsuccessrateandlowcomplicationrate.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
夽 Pleasecitethisarticleas:Kljaji´cV,Vulekovi´cP,VlaˇskiL, Savovi´cS,Dragiˇcevi´cD,Papi´cV.Endoscopicrepairofcerebrospinalfluid
rhinorrhea.BrazJOtorhinolaryngol.2017;83:388---93.
∗Correspondingauthor.
E-mails:[email protected],[email protected](D.Dragiˇcevi´c).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.04.024
1808-8694/©2016Associac¸˜aoBrasileiradeOtorrinolaringologiaeCirurgiaC´ervico-Facial.PublishedbyElsevierEditoraLtda.Thisisanopen
PALAVRAS-CHAVE
Rinorreiadelíquido cerebrospinal; Procedimentos cirúrgicosnasais; Endoscopia; Fístula; Fluoresceína; Desfechodo tratamento
Reparoendoscópicodefístulasliquóricasnasais
Resumo
Introduc¸ão: Aliquorreianasalindicaumafístulaliquórica,umacomunicac¸ãoabertaentreo líquidocerebrospinalintracranianoeacavidadenasal.Podesertraumáticaeespontânea.
Objetivo: Oobjetivo deste estudofoi avaliaro desfecho do reparo endoscópico da fístula liquóricanasalutilizandofluoresceína.
Método: Esteestudoretrospectivoincluiu30pacientesdeambosossexos,comidademédia de48,7anos,tratadosde2007a2015.Todosospacientesforamsubmetidosàadministrac¸ão lombardesoluc¸ãodefluoresceínadesódioa5%nopré-operatório.Afístulafoifechadacom enxertodetrêscamadasecoladefibrina.
Resultados: Asfístulasdelíquidocerebrospinalforamcomumentelocalizadasnoseioetmoidal (37%) eesfenoidal(33%).Amaioriadospacientesapresentou fístulasliquóricastraumáticas (2/3dospacientes).Ataxadesucessorelatadaparaaprimeiratentativadereparofoide97%. Complicac¸õesocorreramemtrêspacientes:umapresentouhidrocefaliaaguda;um,síndrome reversíveldeencefalopatianoquintodiadepós-operatóriocomperdabilateraldavisão,eum foidiagnosticadocomhidrocefaliadoisanosapósoreparodefístulaliquórica.
Conclusão:odiagnósticoendoscópicoeoreparodefístulasliquóricasnasaiscomusode fluo-resceínaintratecaltemaltataxadesucessoebaixoíndicedecomplicac¸ões.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Nasalliquorrheaistheleakageofcerebrospinalfluid(CSF) into the nasal cavity. It may be either spontaneous or traumatic.TraumaticCSFleakage usuallyoccursfollowing basilarskullfractures,oritcanappearasiatrogenicafter surgicalinterventions.Spontaneousleakagecanbewithor withoutelevatedintracranialpressure.1---3
Althoughbasilarskullfracturesareoftenassociatedwith leakageofthecerebrospinalfluid,Millerinitiallydescribed spontaneousCSFleakage in achild withhydrocephalusin 1826.4 Almost a hundred years later; Cushing5 described three cases of surgically treated traumatic CSF leaks. In 1937, Cairns6 demonstrated that CSF leaks could also be repairedwithextraduralapplicationoffascialata.Untilthe mid-twentieth century, transnasal approach was reserved for cauterization, when Dohlman7 described a transnasal-transethmoidal approach that couldseal off leak through the cribriform plate with a septal and middle turbinate flap.
EndoscopicCSFfistularepairisanextracranial extradu-ralapproach.Ithasbeenacceptedworldwideasthemethod of choicebecauseof excellentvisualization, precisegraft placement,minimal damagetosurroundingtissue, preser-vationof olfactoryfunctionin caseof fistulaleakthrough the cribriformplate, shortenedoperating timeandfaster recoverytime.8---12
Intrathecaladministrationofa5%fluoresceinsolutionis highly effective in the detection of CSFfistulas. The use offluoresceingivesnofalsepositiveresults.Falsenegative findingsmaybeduetotemporaryformationofgranulation tissueclosingtheCSFfistulaandpreventingtheleakageto bevisualizedatthemomentofexamination.
The aim of this study was toanalyze the success rate of endoscopic repair of cerebrospinal fluid fistulas using intrathecaladministrationoffluoresceinforintraoperative visualization.
Methods
Thisretrospectivestudyincluded30patientsofbothsexes surgicallytreated for CSF leakage duringthe period from 2007to2015.Therewere19maleand11femalepatients withameanageof48.7years.Agerangedbetween19and 68years.NoneofthepatientshadpreviousCSFfistularepair operation.
Figure1 Fluorescein-stainedcerebrospinalfluidfistulawith aCSFleak,withoutusingabluelightfilter.
measured according to the body weight (0.1mL/10kg of bodyweight), but thehighest dose of intrathecal fluores-cein was 1mL, regardless of the amount of body weight over100kg. Inordertoenhance thevisualization of fluo-rescein,bluelight filter(Storz)wasusedintraoperatively. Theappearanceofcerebrospinalfluidfistulawithoutusing a blue light filter, and with blue light filter is shown in
Figs.1and2.
Having localized the defect, it was closed using three layers---twolayersoffascialatagraftandonemucosallayer (middleturbinatemucosalgraftorfreenasalmucosalgraft) withfibringlue. The endoscopicrepair wasperformed by theotorhinolaryngologistundergeneral anesthesia. Fig.3
showsthesiteofdefectafterCSFleakmanagement. AfterCSFfistula repair, lumbardrain waskept for five postoperativedayswithcompletebedrest.Antibioticswere administeredintravenouslyduringthisperiod.
The investigationwasdone withapproval oftheEthics Committeeofthe institutionwhere thestudy wascarried out(protocolnumberofEthicsCommitteeis00-81/110).
Figure2 Fluorescein-stainedcerebrospinalfluidfistulawith aCSFleak,withabluelightfilter.
Figure3 ThesiteofdefectafterrepairofCSFleakage.
Results
RetrospectiveanalysisoftheetiologicfactorsofCSFleaks showed that the largest number of patients had previous head trauma --- 17 patients (57%), followed by sponta-neousCSFleaksin10patients(33%)while3(10%)patients previously underwent a surgical procedure (one patient underwentseptoplasty,theotheroneunderwentfunctional endoscopicsinussurgeryforchronicrhinosinusitiswith poly-posisandonepatientwasoperatedbytheneurosurgeonfor olfactorymeningioma).Distributionorthepatients depend-ing on the etiology of CSF leakage is shown in Fig. 4. In thegroupofpatientswithtraumaticCSFleakage,mostof them were men (14/17); spontaneous CSFleaks occurred predominantlyinfemalepatients(7/10)whileinthesmall groupof patientswithiatrogenicCSFleakage,therewere twomaleandonefemalepatient.Bodyweightofthe exam-ineesrangedbetween54and116kg,twopatientsweighted over 100kg, with no statistically significant difference in bodyweightbetweenthegroups ofpatientsdependingon theCSFleakageetiology.
Iatrogenic 10%
Spontaneous
33% Traumatic
57%
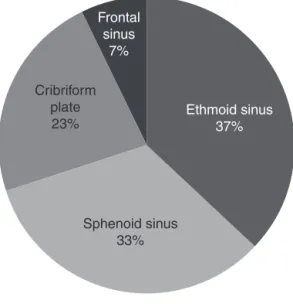
Cribriform plate 23% Frontal sinus 7% Sphenoid sinus 33% Ethmoid sinus 37%
Figure5 CSFleakfistulalocations.
Cerebrospinalfluidleaksweremostcommonlylocatedin theareaoftheethmoidsinus---in11patients(37%),followed bysphenoidsinusandcribriformplateasshowninFig.5.Itis interestingtopointoutthatonepatientpresentedwithfalse nasalliquorrhea.Thispatienthadotoliquorrheawithfistula detected in the basal turn of the cochlea with CSF leak-agethroughtheEustachiantubeintothenasalcavity.This patientunderwentfistularepair viatransmeatal approach andhewasnotincludedinthisstudy.
Success rate of endoscopicrepair washigh(97%) since onlyonepatienthadrecurrentCSFleakagepostoperatively. Itdeveloped onhiseighthpostoperativeday. This patient hadtheCSFleakasaresultofpreviousolfactorymeningioma surgery.DuetothedevelopmentofrecurrentCSFleaksand considering thatthe patienthadloss ofsense ofsmell,it was decided, together with neurosurgeons, to perform a transcranialrepairofCSFfistula.
In examined group of patients, postoperative complications occurred in three of them; two presented with early, and one with late complications. One male patient, 40 years of age, developed acute postoperative hydrocephaluseight hoursafterrepair of the lateral wall ofthesphenoidsinus,andrequiredanurgentneurosurgical intervention(ventriculoperitonealshunting).
On the fifth postoperativeday, one femalepatient, 49 yearsofage, developeda PosteriorReversible Encephalo-pathySyndrome (PRES),manifesting withbilateral lossof vision. Magnetic resonance imagingshowed edema in the occipitalregion.Afterconservativeantiedematherapyusing mannitolandcorticosteroids,allsymptomsresolvedwithin twodays.
Two years after the repair of CSF fistula, one male patient,wasdiagnosedwithhydrocephalus,whichwas man-agedwithaventriculoperitonealshunt.
Therewerenoadversereactionsrelatedtosodium fluo-resceinadministration,whatsoever.
Discussion
Nasalliquorrheaisaseriousconditionthatmayleadto bac-terialmeningitisbyspreadofinfectionfromthenasalcavity
totheendocranium. Duringa 10 year period,almost 80% of patients present with at least one attack of purulent meningitis,someevenmore.Meningitisismorecommonin patientswithtraumaticnasalliquorrhea.12---14
Theauthorsreportednosignificantdifferencerelatedto sexdistribution,whereasinoursample2/3ofpatientswere male,malepatientsoutnumberedfemaleonesinthegroup oftraumaticCSFleaks,whilemostofthepatientswith spon-taneousCSFleakswerefemaleones.Thismaybeduetothe factthat traffic injuries are morecommon amongmales, aswellasoccupationalinjuriesofmaleworkerswhosejob includeshardphysicallabor.Virketal.15reported2/3ofthe studysampletobewomen.
Morethanhalf ofstudiedpatients hada traumaticCSF leakage, and together with those with iatrogenic nasal liquorrhea,itaccounts for 2/3of patients.Kapitanovand associates16 reported an equal number of traumatic and spontaneous CSF leaks, while Virk15 reported on 2/3 of patientswithspontaneousCSFleaks.
ThepredominanceoftraumaticCSFleaksinoursample maybeduetothefactthatourClinicforear,noseandthroat diseasesisatertiaryhealthinstitutionwithclose coopera-tionwiththeClinicofNeurosurgery;thisiswherepatients withsevere injuries arereferred towhenthey cannotbe treatedatthesecondarylevel.
Cerebrospinalfluidfistulasarecommonlylocatedinthe ethmoid(35%), andsphenoidsinus (32%).CSFleaksinthe ethmoidsinus maybecaused by trauma, eitherasa part ofhead trauma or iatrogenic,or theyarespontaneous.A highlypneumatizedsphenoidsinusmayalsocauseCSFleaks. Extreme pneumatizationof the sphenoid sinus maycause boneresorptionintheskullbaseand,sometimes,aprolapse andtearingofthedura.Asmallmeningocelemayoriginate frombonedehiscenceintheoverpneumatizedareasandthis pathogenicmechanism shouldbeconsidered animportant etiological factor for spontaneous CSFleak development. SpontaneousCSFleaksarecommonlylocatedinthelateral wallofthesphenoidsinus.17
Endoscopic endonasal repair of CSF leaks had a high success rateof 97%. This can be attributedtothe use of sodiumfluoresceinsolutionandbluelight filterfor detec-tion of cerebrospinal fluid fistula. Only one patient had recurrentCSFleakagewhichdevelopedonhiseighth post-operativeday.ThispatienthadtheCSFleakasaresultof previousolfactory meningiomasurgery. Otorhinolaryngolo-gistsuggestedendoscopicreoperation,butsincethepatient already had no sense of smell, it was decided, together withneurosurgeons,toperformatranscranialrepairofCSF fistula.
solutionforintrathecaladministrationisused,inthe appro-priatedosage,itisnotassociatedwithanyadverseeffects.21 Complications were reported when using 10% fluorescein solution for intravenous administration and included ver-tiginoussymptoms,tinnitus,cranial nerveandspinal cord impairment,epilepticseizures.
Webelievethatuseoflumbardrainsfor5dayshas posi-tiveeffectsonthesuccessofCSFrepair,becauseitreduces thepressureatthepointofdefectclosure;however,some authorsdonotshare thisopinionand believethatlumbar drainsarenecessaryonlyinpatientswithincreased intracra-nialpressure.15Ontheotherhand,someauthorsdonotuse lumbardrainsafterCSFrepairatall.22,23Inhisstudy,Oles24 didnotuselumbardrains,andpostoperativemanagement wasbasedondiureticsfor5days.
Early postoperative complications were present in 2 patients(6%);onemalepatientpresentedwithacute hydro-cephaluseighthoursfollowingsurgery,whichwasprobably the reason for spontaneously nasal liquorrhea, although preoperativeMRIinthispatientshowednosignsof hydro-cephalus and/or altered CSF flow. The second female patient developed a Posterior Reversible Encephalopathy Syndrome(PRES),manifestingwithbilaterallossofvision. Shewasexaminedbytheophthalmologist,theocular fun-dus appeared normal. Endocranial CT was done with no pathologydetected,but MRIshowededema inthe occipi-talregion.Anti-edematoustherapysuccessfullyresolvedthe symptoms.PRESwasdescribedbyHincheyandassociatesin 1996.25 It usuallyoccursin patients withoscillating blood pressurecausedbyhighbloodpressure,renalinsufficiency andinthosewhoareimmunosupressed.Ourpatient,unlike thesepatients,hadnocomorbidities,herbloodpressurewas normal.Mostofthepatientswiththissyndromearefemale, asproveninourstudy.
One male patient developed late complication, two years following surgery, in the form of hydrocephalus which was managed with ventriculoperitoneal shunt. He also underwent preoperative endocranial MRI showing no abnormalities in CSFflow. MRI is indicated in all patients with non-traumatic CSF leaks in order to detect alter-ationinCSFflow andincasesof developedpostoperative complications.
Therewere nocomplications or sideeffects relatedto sodiumfluorescein.
Conclusion
Nasalliquorrheausuallyoccursinmalepatientsasaresult ofprevioustrauma.
Endoscopic detection and repair of cerebrospinal fluid fistulaswiththree-layergraftandfibringluehashighsuccess rateandlowcomplicationrate.
Theuseof5%sodiumfluoresceinsolutionforintrathecal administration, in the appropriate dosage, is a safe pro-cedure for detection of cerebrospinalfluid fistulas during endoscopicsurgeryandcausesnoadverseeffects.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.OberaderS.PrimarynontraumaticspontaneousCSFrhinorrhea with normal CSF pressure. Arch Neurol Neurochir Psychiatr. 1972;111:369---76.
2.Ommaya AK, DiChiro G, Baldwin M, Pennybacker JB. Non-traumatic cerebrospinalfluidrhinorrhea.JNeurol Neurosurg Psychiatr.1968;31:214---25.
3.SpetzlerRF,WilsonCB.Duralfistulaandtheirrepair.In:Youmans JR,editor.Neurologicalsurgery.2nded.Philadelphia:Saunder; 1982.p.2209---27.
4.MillerC.Caseofhydroceohaluschronicus,withsomeunusual symptomsandappearancesondissection.TransMedChirSoc Edinb.1928;2:243---8.
5.Cushing H. Experience with orbito-ethmoidale osteomata having intracranial complications. Surg Gynecol Obstect. 1927;44:721---2.
6.CairnsH.Injuriesofthefrontalandethmoidalsinuswith spe-cialreferencetocerebrospinalfluidrhinorrheaandaerocele.J LaryngolOtol.1937;52:589---623.
7.DohlmanG.Spontaneous cerebrospinalfluidrhinorrhea.Case reportbyrhinologicmethods.ActaOtolaryngol(Stockh)[suppl]. 1948;67:20---3.
8.Mattox DE, Kennedy DW. Endoscopic management of cerebrospinal fluid leaks and cephalocele. Laryngoscope. 1990;100:857---62.
9.DodsonEE,GrossCW,SwerdloffJL,GustafsonLM.Transnasal endoscopicrepair ofcerebrospinalfluid rhinorrheaand skull basedefect:areviewof29cases.OtolaryngolHeadNeckSurg. 1994;111:600---5.
10.StankiewiczJA.Cerebrospinalfluidfistulaandendoscopicsinus surgery.Laryngoscope.1991;101:250---6.
11.Schaefer SD, Manning S, Close LG. Endoscopic paranasal sinus surgery: indications and considerations. Laryngoscope. 1989;99:1---5.
12.SharmaDP,SinghD,SinhaS,SrivastvaAK,SinghH,JagetiaA, etal.CSFrhinorrhea:anoverviewofendoscopicrepair.Indian JNeurotrauma.2010;7:157---62.
13.CrawfordC,KennedyN,WeirWR.Cerebrospinalfluidrhinorroea and Hemophilusinfluenzae meningitis37years aftera head injury.JInfect.1994;28:93---7.
14.DjilvesiD,Vulekovi´cP,Cigi´cT,Kojadinovi´c ˇZ,Papi´cV,HorvatI. Post-traumaticcommunicationofendocraniumandnasalcavity withrecurrentmeningoencephalitiswithoutrhinorrhea---case report.Vojnosanitetskipregled.2010;67:945---8.
15.VirkJS,ElmiyehB,SalehH.Endoscopicmanagementof cere-brospinal fluid rhinorrhea: the charing cross experience. J NeurolSurgB.2013;74:61---7.
16.Kapitanov DN, Lopatin AS, Potapov AA. Endoscopic diagno-sisand treatmentofnasal rhinorrhea.VestnOtorinolaringol. 2003;4:20---4.
17.Andrey S, Lopatin MD, Dmitry N, Kapitanov MD, Alexander A, Potapov MD. Endonasal endoscopic repair ofspontaneous cerebrospinalfluid leaks. Arch Otolaryngol Head Neck Surg. 2003;129:859---63.
18.NyquistGG,AnandVK,MehraS,KackerA,SchwartzTH. Endo-scopicendonasal repairof anterior skull basenon-traumatic cerebrospinalfluidleaks,meningoceles, andencephaloceles. JNeurosurg.2010;113:961---6.
19.LeeDH,Lim SC, JooYE.Treatmentoutcomesof endoscopic repairsofsinonasalcerebrospinalfluidleaks.JCraniofacSurg. 2011;22:1266---70.
20.Seth R, Rajasekaran K, Benninger MS, Batra PS. The util-ityofintratecalfluoresceinincerebrospinalfluidleakrepair. OtolaryngolHeadNeckSurg.2010;143:626---32.
22.PsaltisAJ,SchlosserRJ,BanksCA,YawnJ,SolerZM.A system-aticreviewoftheendoscopicrepairofcerebrospinalfluidleaks. OtolaryngolHeadNeckSurg.2012;147:196---203.
23.CasinoRR,JassirD.Endoscopiccerebrospinalfluidrhinorrhea repair:isalumbaldrainnecessary?OtolaryngolHeadNeckSurg. 1999;121:745---50.
24.Oles K, Skladzien J, Tomik J, Leszczynska J. Transnasal endoscopic treatmentof cerebrospinalfluid leaks: 10 years experience.B-ENT.2013;9:201---6.