www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Middle
ear
impedance
studies
in
elderly
patients
implications
on
age-related
hearing
loss
夽
Olusola
Ayodele
Sogebi
DepartmentofEarNoseandThroat,OlabisiOnabanjoUniversityTeachingHospital,Sagamu,Nigeria
Received1November2013;accepted12April2014 Availableonline8October2014
KEYWORDS
Acousticimpedance tests;
Pure-tone audiometry; Aged; Presbycusis; Acousticreflex
Abstract
Introduction:Controversiesarisewithrespecttofunctioningofthemiddleearovertime.
Objective: Toassesschangesinmiddleearimpedancethatmayberelatedtoaging,and/orif therewasanassociationofthesechangeswiththoseoftheinnerearintheelderlypatients.
Methods:Cross-sectional, comparative study of elderly patients managed in ear, nose and throatclinics.Astructuredquestionnairewasadministeredtoobtainclinicalinformation.Pure toneaudiometry,tympanometry,andacousticreflexeswereperformed.Comparative analy-seswereperformedtodetectintergroupdifferencesbetweenclinico-audiometricfindingsand middleearmeasures,viz.tympanogramsandacousticreflexes.
Results:Onehundredandthreeelderlypatientsparticipatedinthestudy;52.4%weremale, averagely70.0±6.3yearsold,age-relatedhearinglossin59.2%,abnormaltympanogramsin 39.3%,absentacousticreflexin37.9%.Therewasnoassociationbetweenageandgenderin patientswithabnormaltympanogramsandabsentacousticreflex.Significantlymorepatients withdifferentformsandgradesofage-relatedhearinglosshadabnormaltympanometryand absentacousticreflex.
Conclusion: Some abnormalities were observed in the impedance audiometric measures of elderlypatients,whichweresignificantlyassociatedwithparametersconnectedtoage-related hearingloss.
© 2014Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽
Pleasecitethisarticleas:SogebiOA.Middleearimpedancestudiesinelderlypatients:implicationsonage-relatedhearingloss.BrazJ Otorhinolaryngol.2015;81:133---40.
E-mail:[email protected] http://dx.doi.org/10.1016/j.bjorl.2014.09.007
PALAVRAS-CHAVE
Impedânciaelétrica; Audiometriadetons puros;
Idoso; Presbiacusia; Reflexosacústicos
Estudosdeimpedânciadaorelhamédiaempacientesidosos;implicac¸õesnaperda auditivarelacionadaàidade
Resumo
Introduc¸ão:Existem controvérsiasnoqueserefereàsalterac¸õesfuncionaisdaorelhamédia comopassardosanos.
Objetivo:Avaliarasmudanc¸asnaimpedânciadaorelhamédiaquepodemestarrelacionadas aoenvelhecimento,bemcomoqualquerassociac¸ãodessasalterac¸õescomasqueocorremna orelhainterna.
Método: Estudoprospectivocomparativodepacientesidososatendidosemambulatórios espe-cializadosemotorrinolaringologiaeaplicac¸ãodequestionárioestruturadopara obtenc¸ãode informac¸õesclínicas.Foramrealizadas audiometriadetonspuros,timpanometriaereflexos acústicos e análise comparativa para detectar as diferenc¸as intergrupos entre os achados clínico-audiométricos.
Resultados: Participaramdoestudo103pacientesidosos:52,4%dogêneromasculino;idadede 70±63anos;perdaauditivarelacionadaàidadedetectadaem59,2%;timpanogramaanormal em 39,3%;ereflexoacústicoausenteem37,9%. Nãofoi encontradaassociac¸ão entreidade egêneroem pacientescomtimpanogramaanormal ereflexoacústicoausente. Umnúmero significantementemaiordepacientescomdiferentesgrauseconfigurac¸õesdeperdaauditiva relacionadaàidadeapresentoutimpanometriaanormalereflexoacústicoausente.
Conclusão:Algumasanormalidadesforamobservadasemmedidasdeimpedânciaaudiométrica empacientesidosos,queforamsignificantementeassociadoscomosparâmetrosligadosàperda auditivarelacionadaàidade.
©2014Associac¸ãoBrasileira deOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicadopor ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Hearing involves a complex interplay and integration of severalmechanisms,including conduction ofsound waves fromtheenvironmentthroughtheexternalauditorycanal, vibrations of the tympanic membrane, stimulation of the transformermechanism in the middle ear, aswell asthe sensoryhaircellsofthecochleathecentralneuronal con-nectionswithtermination at theprimaryauditory cortex. Thefunctionsofsomeofthesemechanismsareaffectedby agingandtendtomanifestashearingimpairment,whichis particularlycommonintheelderly.
Adeficit inhearingacuityis themost commonsensory disorderthathasbeenassociatedwithaging.1Infact,
stud-ieshaveshownthatapproximatelyone-thirdofadultsaged
between 61 and 70 years, and over 80% of those older
than85yearshaveclinicallyobviousdifficultyunderstanding
speechandfollowingconversationsinthepresenceof
back-groundnoise.2,3Ontheaverage,hearingthresholdincreases
byapproximately1dBperyearfor subjectsaged60 years
andabove,with atendency tofurtherdeterioration with
increasingage.4 At audiometry,up to35% of elderly
sub-jectsabove 60 years had pure tone average threshold of
25dB HL or more at frequencies between 0.5 and 4kHz,
whichincreased furtherto50% inthe age groupbetween
70and80years.5Whilethereportedprevalenceofhearing
lossamongelderlysubjectsvaryindifferentlocations,itis
anestablishedfactthatitincreaseswithage.6
Traditionally,hearinglossisclassifiedasconductive,
sen-sory,neural,ormixed-type.Age-relatedchangesintheinner
earanditscentralconnectionshavebeenwelldocumented
amongelderlysubjects.Theseincludelossof sensoryhair
cells of the cochlea consequent upon generalized
degen-erative processes,dysfunction of the striavascularis (the
main blood supply to the organ of Corti), and
degenera-tion of the neurons of the cochlear nerve or its central
connections.7 In the external ear, wax impaction in the
externalauditorymeatushasbeenreportedtobe
dispropor-tionatelymorecommonintheelderlypatientsthaninother
groupsofpatients,causingconductivehearingloss.8Thisis
aconsequence of thegeneralizeddegenerationof
epithe-lia,includingthoseofthemicrocilia,affectingtheexternal
auditory canal without an accompanying reduction in the
rateofwaxproduction.Othercausesofconductivehearing
lossareoftenrelatedtothefunctioningofthemiddleear.
Comparedwithothercategoriesofpatients,little
atten-tionhasbeenpaidtotheconductivemiddleearcomponents
inelderlypatients.Controversiesariseconcerningthe
func-tioning of the middle ear as age advances. While some
studies concludedthat theconducting mechanismsof the
middleearremainnormalandfunctional,orthattheymay
play noseriousrole in thehearing impairmentassociated
withaging,9,10othersobservedsomechangesinthedynamic
characteristics of the middle ear that may be related to
aging.11,12Thismighthaveresultedfromdifferenttypesof
instrumentsusedforassessingthemiddleearfunctions.As
partofthestudyontheepidemiologyofhearingimpairment
amongelderly patients, the authorperformed both
pure-toneandimpedanceaudiometries(tympanometry)toassess
thefunctionsoftheinnerandmiddleear,respectively.13The
observationofcertainabnormaltympanometrictracingsin
supposedlypurelysensorineuralhearingloss(SNHL)
stimu-latedthisresearch.
Thisstudyaimedtoassesswhethertherewerechanges
inthemiddleearimpedancethatmayberelatedtoaging,
and/orwhethertherewereanyassociationofthesechanges
withthoseoftheinnerearintheelderlysubjects.Thisis
justifiablebecausehearinglossimpactsthequalityoflifeof
elderlysubjects.
Methods
Studydesign
Thiswasaprospective(cross-sectional),comparativestudy
ofelderlypatientsfollowed-upatspecializedear,nose,and
throat(ENT)clinicsforathree-yearperiod.
Setting/studylocation
This study was conducted at the ENT clinics of a
ter-tiaryreferralhospitalandofaprivate/missionaryhospital.
EthicsapprovalforthisstudywasobtainedfromtheHealth
Research and Ethics Committee, under approval number
OOUTH/DA.326/T/197.
Samplingcriteria/technique
The inclusioncriteriawereelderly patientsaged60 years
and above, who had no clinical middle ear disease,
attendedoneoftheENTclinics.Patientswereconsecutively
recruited.Thegeneralnature,significance,requirementsof
thepatients,includingthefactthatdecliningtoparticipate
in the study would not affect treatment, were explained
tothe patients.Consenting patientswere included in the
study.The categories of the patients that were excluded
were:thosewhodidnot consent,historyof recurrentear
discharges, and those with tympanic membrane
perfora-tions. Patients with wax impaction were treated before
the continuation of the study protocols. Patientswithout
complete investigations(bothforms ofaudiometry---pure
toneaudiometry[PTA]andtympanometry),with
asymmet-ricaudiograms,orevidenceofconductiveormixedhearing
lossintheirPTAsweresubsequentlyexcluded.
Studyperiod
Januaryof2010---Juneof2013.
Datasourcesandcollectionprocedure/technique
Dataweregeneratedusinginterviewer-administered
ques-tionnaires,dividedintothreesections.SectionAcomprised
socio-demographicinformation.Section Bconsistedof the
medical condition including questions on history of
per-ceived hearing loss, durationof hearing impairment, and
presentorpreviousearsurgeries,amongothers.
Section C wasdocumentation of the findings on
phys-ical examination, especially the status of the tympanic
membranes,andrecordsoftheaudiometricprofilesofthe
patients,whichincludedthePTA,tympanometry,and
acous-ticreflexes.
AtPTA,airconductionandbone-conductionevaluations
were performed in a commercial sound booth, using an
Amplivoxdiagnosticaudiometermodel 240,withstandard
earphonesenclosedinsupra-auralearcushions,anda
stan-dardbone-conductionoscillatorandheadbandtoevaluate
air-bonegaps.Tympanometrywasconductedbybroadband
middle earpower reflectance and measured using a
cali-brated,commerciallyavailablecomputer-controlledsystem
(InteracousticsmodelMT10.SN156607)thatincorporateda
high-qualityprobeassemblytotransducestimuliandrecord
acousticresponsesfromtheearcanal.Theacousticreflex
thresholdsweretestedwithcontralateralstapedialreflexes
forfrequenciesof500,1000,2000,and4000Hz;the
thresh-oldswereconsideredasnormalwhenelicitedbetween75
and110dBHL.
Main outcome measure: patients were paired into
dif-ferent categories based on the PTA findings as Normal
orAge-related hearingimpairment-presbycusis).The
tym-panogramswereclassifiedaccordingtoJergertypesA,As,
Ad,B,andC;14 withtypeAconsideredasnormal,andany
other tympanographic types as abnormal, while acoustic
reflexeswereclassifiedasPresentorAbsent.
Dataanalysis
Descriptive analysis of the data was done and presented
in tabular and graphical forms. Comparative analyses
wereperformedtodetectinter-groupdifferencesbetween
the clinico-audiometric findings and different middle ear
measures, viz. tympanograms and acoustic reflexes, by
cross-tabulationwithcontingencytables.Categorical
varia-bles were presented as percentages and proportions and
analyzedusingChi-squaretest,whilecontinuousvariables,
presented asabsolute valuesand means, were compared
usingStudent’s t-test. The level of statistical significance
wassetatp<0.05.DataanalysiswasperformedusingSPSS
version19.0(Chicago,IL,UnitedStates).
Results
Onehundredandthree(103)elderlypatientsparticipated
in the study,which comprised 52.4% males, (M:F=1.1:1).
Theagesof thepatientsranged between61 and96years
withamean±SDof70.0±6.3years.Thesocio-demographic
characteristicsof thepatients areshown inTable 1.Over
half(59.2%) of thepatients hadaudiometric evidences of
ARHL,andtheSchuknechttypologyisrepresentedinFig.1.
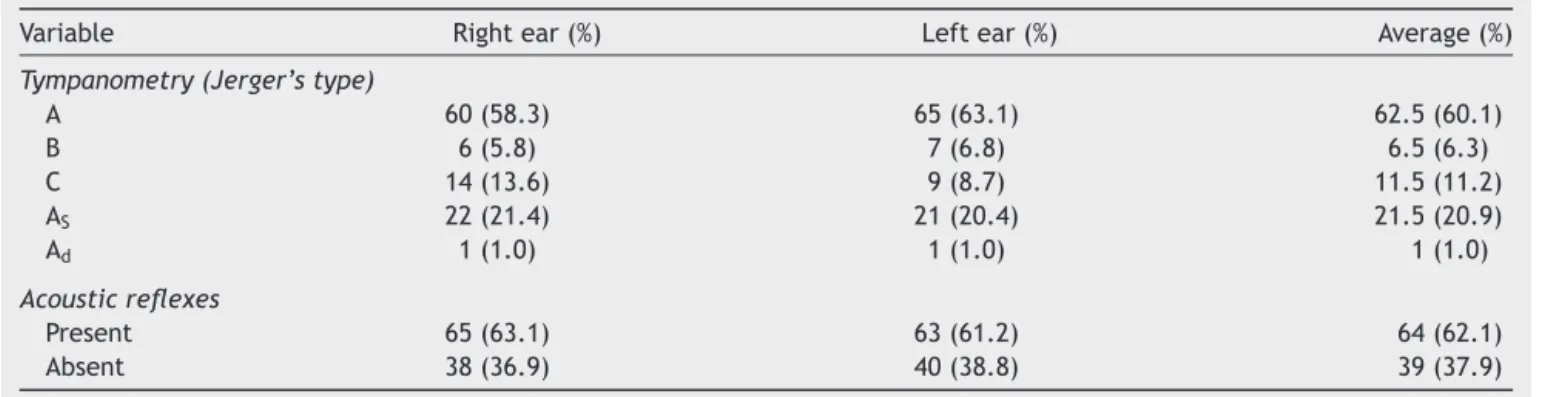
Theimpedanceaudiometryfindingsbasedon
tympanomet-rictracingsaccordingtoJerger’sclassificationrevealedthat
onaverage,60.7% of theparticipants hadnormal (typeA
tympanograms),withahighconcordancebetweenthetwo
ears.The acousticreflexes werepresent inan average of
62.1%ofthepatients.Thedetailsoftheimpedance
Table1 Socio-demographiccharacteristicsofthepatients.
Variable n%
Agegroup(years)
61---65 27(26.2)
66---70 35(34.0)
71---75 25(24.3)
76---80 10(9.7)
≥81 6(5.8)
Mean±SD 70.0±6.3
Gender
Male 54(52.4)
Female 49(47.6)
Maritalstatus
Married 83(80.6)
Others(divorced/widowed) 20(19.4)
Educationlevel
Noformaleducation 3(2.9)
Primaryschool 21(20.4)
Secondaryschool 55(53.4)
Tertiary 24(23.3)
Occupationgroup
Unskilled 17(16.5)
Semi-skilled 44(42.7)
Professional 42(40.7)
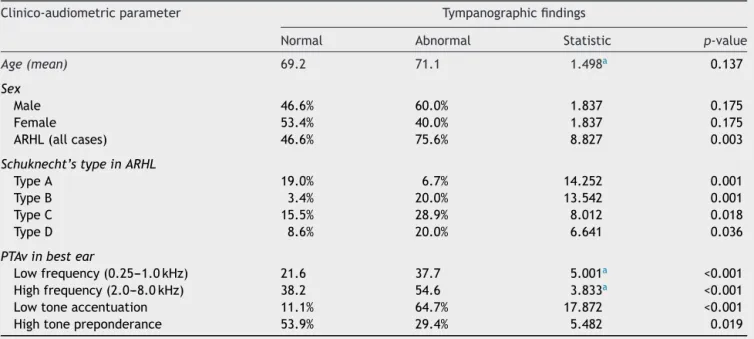
Age,gender,andPTAfindingsofthepatientswere com-parativelyanalyzedagainst thetympanometric findingsin
Table 3. Based on the age distribution of the patients,
theyweresubdividedintotwogroups,≤70and>70years.
There were no statistically significant differences in the
tympanogramsregardingage(t=1.498,p=0.137)and
gen-der (2=1.837, p=0.175) of the patients. There was a
differencewhenthehearingstatus(PTAfindings)was
com-pared;significantlymorepatientswithage-relatedhearing
loss (ARHL) had abnormal tympanometric findings. These
werealsoobviouswhenconsidering thedifferentpatterns
ofaudiometricfindingsthatwereobservedinpatientswith
ARHL. Furtheranalysis of the PTA of patients withARHL,
consideringthedegreesofhearinglossescalculatedaspure
toneaverages(PTAv)indBHLatthelow(0.25,0.50,1.0kHz)
Normal, 40.8%
Normal
Type A, 13.6% Type B, 10.7%
Type C, 21.4% Type D, 13.6%
Type A Type B Type C Type D
Figure 1 Distribution of PTA findings of the patients. Schuknecht’stypologyonlyforpatientswithARHL.
and thehigh (2.0, 4.0,and 8.0kHz) frequencies was
per-formed.
Exploring the PTAv in the better ear at the low
(0.25---1.0kHz) frequencies revealed a mean of 28.7dB
HL (SD=18.0). Low frequency accentuationof the
audio-gram was taken as at least 40dB HL for the PTAv (WHO
classificationformoderatehearingloss)atthelow
frequen-cies.Atthehigh(2.0---8.0kHz)frequencies,computationof
thePTAvinthebetterear,resultedinameanof45.4dBHL
(SD=23.0).EstimateofthedifferencesinthePTAvbetween
thehightonesandlowtonesinthebetterearsrevealeda
meanof24.1dBHL(SD=10.1),thusa valueof≥25dBHL
differencewasusedasthecriterionforahightone
prepon-deranceoftheaudiogram.
ThePTAvatthelowandhighfrequencies inthebetter
ear andother parameters,namely low tone accentuation
Table2 Impedanceaudiometricfindingsinthepatients.
Variable Rightear(%) Leftear(%) Average(%)
Tympanometry(Jerger’stype)
A 60(58.3) 65(63.1) 62.5(60.1)
B 6(5.8) 7(6.8) 6.5(6.3)
C 14(13.6) 9(8.7) 11.5(11.2)
AS 22(21.4) 21(20.4) 21.5(20.9)
Ad 1(1.0) 1(1.0) 1(1.0)
Acousticreflexes
Present 65(63.1) 63(61.2) 64(62.1)
Table3 Relationshipbetweenclinico-audiometricandtympanographicfindings.
Clinico-audiometricparameter Tympanographicfindings
Normal Abnormal Statistic p-value
Age(mean) 69.2 71.1 1.498a 0.137
Sex
Male 46.6% 60.0% 1.837 0.175
Female 53.4% 40.0% 1.837 0.175
ARHL(allcases) 46.6% 75.6% 8.827 0.003
Schuknecht’stypeinARHL
TypeA 19.0% 6.7% 14.252 0.001
TypeB 3.4% 20.0% 13.542 0.001
TypeC 15.5% 28.9% 8.012 0.018
TypeD 8.6% 20.0% 6.641 0.036
PTAvinbestear
Lowfrequency(0.25---1.0kHz) 21.6 37.7 5.001a <0.001
Highfrequency(2.0---8.0kHz) 38.2 54.6 3.833a <0.001
Lowtoneaccentuation 11.1% 64.7% 17.872 <0.001
Hightonepreponderance 53.9% 29.4% 5.482 0.019
a Statistic,Student’st-test.
andhightonepreponderance,werecomparedwiththe
tym-panometricfindingsinpatients withARHL. Allparameters
presented statistically significantlydifferences for
tympa-nometricabnormalities,asshowninTable3.
A similarcomparativeanalysiswasperformed withthe
acousticreflexesastheoutcome variable.Similarto
tym-panometric findings, there were no associations between
ageofpatientsthathadabsentacousticreflexes(t=0.970,
p=0.334),andgender(2=0.363,p=0.549)inTable4.
Sta-tisticallysignificantdifferenceswereobservedforpatients
with ARHL, those with type B Schuknecht audiometric
pattern,thePTAvs,andalsoinpatientswithlowtone
accen-tuationoftheirPTAs.
Discussion
This study has demonstrated that elderly patients had
some functional anomalies in the middle ear impedances
andacousticreflexes.Impedanceaudiometricabnormalities
Table4 Relationshipbetweenclinico-audiometricfindingsandacousticreflexes.
Clinico-audiometricparameter Acousticreflex
Normal Abnormal Statistic p-value
Ageinyears(Mean) 69.5 70.8 0.970a 0.334
Sex
Male 54.8% 48.8% 0.363 0.549
Female 45.2% 51.2% 0.363 0.549
ARHL(allcases) 50.0% 73.2% 5.487 0.019
Schuknecht’stype
A 12.9% 14.6% 4.961 0.085
B 4.8% 19.5% 10.106 0.006
C 17.7% 26.8% 2.937 0.230
D 14.5% 12.2% 0.154 0.925
PTAvinbestear
Lowfrequency(0.25---1.0kHz) 24.1 35.9 3.326a 0.001
Highfrequency(2.0---8.0kHz) 39.3 54.5 3.448a 0.001
Lowtoneaccentuation 19.4% 63.3% 12.191 <0.001
Hightonepreponderance 48.4% 36.7% 0.856 0.355
were significantly higher in elderly patients with various
formsanddegreesofARHL,beingmorepronouncedinneural
andstrialtypes,andinlowfrequencyaccentuationofARHL.
Acousticstapedial reflexesappeared tobelessinfluenced
byARHLthantympanometry,anditmaybeamorereliable
indicatorofabnormalmiddleearfunction.
Researchersassessinghearinganditsimpairmentamong
elderly patients have focused disproportionatelyon ARHL
relatingtothesensorineuralaspectofhearing,with
appar-ent neglect of the conductive component. However, the
present study revealed that an average of 39.3% of the
elderly patients had abnormality in their tympanometric
tracings,andaverageof37.9%hadabsentacousticreflexes.
Itcannotbeconclusivelyascertainedwhetherthesemiddle
earabnormalitieswereduetoagingprocess,ormere
coinci-dentalfindings.Nondahletal.15reportedasmalldegreeof
middle-earstiffeningoccurringovertheyearsamongolder
adults.Ananimalexperimentalsofoundstructuralchanges
inthemiddleearofmousethatwereattributabletoaging.16
Therewasnosignificantdifferencebetweentheagesof
elderlypatientswithnormalorabnormaltympanogramsand
betweenthosewithandwithoutacousticreflexes.Gaihede
and Koefoed-Nielsen17 compared compliance and middle
earpressuremeasured by tympanometry betweennormal
elderlysubjects (meanage 77 years)and normalyounger
patients (mean age 29 years);they observed that middle
earcompliancewasnotinfluencedbyvariationinage.
Sim-ilarly,noassociationwasfoundbetweenthegender ofthe
patientsandmiddleearmechanicsanalogoustofindingsof
theBlueMountains HearingStudyinAustralia.18 Theseare
atvariancewithreportsconcerningpresbycusis,whichwere
reportedtobesignificantlyassociatedwithadvancingage
andalsowiththemalegender.19
The prevalence of anomalies observed in the middle
ear mechanisms in this study were comparable to the
reportedprevalenceofARHL.20,21Thismaysuggesta
simul-taneous or concurrent effect in both the inner and the
middle ear. The abnormal tympanometric findings of the
patients revealed that the Jerger’s typeAs tympanogram
wasthemost commonamongthepatients similartothat
found among centenarians in China,20 providing an
evi-dence of increased stiffness (reduced compliance) of the
conducting mechanisms.15 This was followed by the type
Ctympanogramsuggestiveofeustachiantubedysfunction.
Thus, it is hypothesized that common middle ear
func-tionalanomaliesmaybeattributabletoeitherofthesetwo
pathologies.Sometimesabnormalitiesoccurinthetympanic
membrane and in the bony ossicles, resulting in
signifi-cantmiddleearfunctionalimpairment.16Thereisevidence
that,withadvancing age,thehumantympanicmembrane
exhibits a loss of vascularization, a reduction in collagen
structure, in elasticity,and greater rigidity in the middle
fibrouslayer.22Thesestructuralchangeswouldbeexpected
toalter the compliance response of the middle ear. One
belatedinvestigationofairandboneconductionthresholds
hasobservedmiddle-earlossesofasmuchas12dBinelderly
patients.23
The possibilitythatARHL either initiates or aggravates
abnormalitiesintheimpedancecharacteristicsofthe
mid-dleearshouldalsobeconsidered.Theaudiometricpattern
ofelderlypatientswithARHLobservedinthepresentstudy
showeda preponderance of Schuknecht’s typeC, such as
in other Africanpopulations,24 and distinctfromthe
typi-calslopingpure toneaudiogram commonamongwhites.25
The finding that all Schuknecht’s audiometric patterns in
patients with ARHL were associated with tympanometric
abnormalities, suggested a link withthe etiopathogenesis
of these two entities in elderly patients. It is expected
that subjects with abnormal tympanograms should
mani-fest with hearing loss of conductive type. However, the
finding of these tympanometric patterns also in patients
with normaland sensorineural (ARHL) hearing loss should
stimulate further research into middle ear impedance
mechanisms.
UsingSchuknecht’stypologyinpatientswithARHL,two
particulartypes ofaudiograms(BandC)theoreticallyhad
accentuation at the low frequencies. In this study, these
twoaudiometrictypes comprisedoverhalf (33/61;54.1%)
ofthe audiometrictypesin patientswithARHL. Thus,the
association of low tone accentuation of audiograms with
abnormal tympanograms may derive from the
dispropor-tionate distribution of these two audiometric patterns in
the ARHL patients. Eustachian tube compliance has been
observedtochange withaging,26 butwhetherthischange
is influencedmorebyneural orstrial typesofpresbycusis
remains to beascertained. Contrary toreports of Feeney
and Sanford,9 the present findings suggest an increase in
middle-ear stiffness with specific types of ARHL. Thus,
these impedance middle earchanges may be particularly
commonintheAfricanpopulation,andneedfurther
clarifi-cation.
Itis noteworthy thatthere werediscordant findings in
someofthemiddleearmeasuresbetweentheears.These
suggestthat,despitetheearsbeingexposedtoalmostthe
sameconditions,theinfluencesandtheresponsesmightnot
beexactlysame.Thepossibilityofconfoundingfactors,such
asosteoarthritis(whichmightaffectossicularjointsofthe
earsunequally,producingtypeAstympanogram),mayalso
be considered. Asymmetrical audiograms have also been
reportedinpatientswithARHL.13,24
Manyexpertsconsider2.0kHzasbeginningofhigh
fre-quency, although the definition varies.4,27,28 PTAv at high
frequencies andhigh tonepreponderanceHLwere
associ-ated withabnormalities in tympanometricfindings in this
study.Wileyetal.29 reportedthat,foryoungeragegroups
(50---69years),thresholdchangeswerehigherforhigher
fre-quencies,whileinolderagegroups(70---89years),threshold
changes were higher for lower frequencies. Interestingly,
the agedistributionof thepresent patients is in-between
thesetwodivisions.Causesof high-frequencyhearingloss
have a wide variability,21 andthere is a possibilityof
co-existenceoffewoftheseinsomeofthepresent patients.
Thus,itispossiblethatnotenoughpatientswithpureARHL
werestudied.Conversely,lowfrequencyhearinglossisnot
easytoidentify,sinceittendstobeasymptomatic.Infact,
lowerfrequencysoundsdonothaveasmuchinformationas
soundsinthehigherfrequencies.30Oneofthefewcluesto
alow-frequencyhearinglossisthatthepersonhasdifficulty
hearingingroups orina noisyplace.It wasreportedthat
inertiaof themiddle earisnot animportant contribution
totheperception of boneconduction sounds for
frequen-ciesbelow1.5kHz,butappearstocontributeatfrequencies
between1.5and3.5kHz.30However,thisstatementmaynot
The pathway involved in the acoustic reflex is
com-plexandcaninvolvetheossicularchain,cochlea,auditory
nerve,brainstem,facialnerve,andothercomponents.The
absence of acoustic reflex has been shown to effectively
detect hearing lossesexceeding 30dB in adult subjects,31
althoughitmaynotbeconclusiveinidentifyingthesource
of the problem.32 Like impedance measures, parameters
related to ARHL (namely Schnekcht’s type B audiogram,
PTAv, and low-tone accentuation) were significantly
asso-ciatedwithabsenceofthe acousticreflexes in thisstudy.
However, the absence of the acoustic reflexappeared to
be less influenced by parameters relating to ARHL, and
it may possibly be a more reliable parameter in
assess-ing the effect of ARHL on the functioning of the middle
ear.
Thisstudyhadsomelimitations.Firstisthelower
sensi-tivityoftheconventionaltympanometerinassessingmiddle
ear function compared with sweep frequency middle-ear
analyzer.The factthatmagnitudeof theacousticreflexes
wasnotascertainedis alsoa limitation.Furthermore,the
hospital-based nature of the study is prone to bias, as
patients may not represent a normal population of the
elderly. Despite these limitations, the study was able to
demonstrate that the middle ear functioning of elderly
patientsmaynotbefullynormal.
Conclusion
Someabnormalitieswereobservedinimpedance
audiomet-ric measures of elderly patients, which were significantly
associatedwithparameters relatedtoARHL. This arouses
suspicion of some middle ear changes that may be
attributabletoaging.Itisimperativethatelderlypatients
with hearing impairment have both their inner and
mid-dle ear assessed, in order to manage them optimally.
Community-based,longitudinal studies areneeded to
fur-therclarifythesefindings.
Conflicts
of
interest
Theauthordeclaresnoconflictsofinterest.
References
1.VanEykenE,VanCampG,VanLaerL.Thecomplexityof age-relatedhearing impairment: contributing environmental and geneticfactors.AudiolNeurootol.2007;12:345---58.
2.WallingAD,DicksonGM.Hearinglossinolderadults.AmFam Physician.2012;85:1150---6.
3.GlydeH,HicksonL,CameronS,DillonH.Problemshearingin noiseinolderadults:areviewofspatialprocessingdisorder. TrendsAmplif.2011;15:116---26.
4.LeeFS, MatthewsLJ,Dubno JR,MillsJH. Longitudinalstudy ofpure-tonethresholds inolder persons.Ear Hear.2005;26: 1---11.
5.Wiley TL, Cruickshanks KJ, Nondahl DM, Tweed TS. Aging and middle ear resonance. J Am Acad Audiol. 1999;10: 173---9.
6.PacalaJT,YuehB.Hearingdeficitsintheolderpatient:Ididn’t noticeanything.JAMA.2012;307:1185---94.
7.Bielefeld EC,Tanaka C,ChenGD, Henderson D.Age-related hearing loss: is it a preventable condition? Hear Res. 2010;264:98---107.
8.Sogebi OA. Profile of ear diseases among elderly patients in Sagamu, south-western Nigeria. Niger J Med. 2013;22: 143---7.
9.Feeney MP, Sanford CA. Age effects in the human mid-dle ear: wideband acoustical measures. J Acoust Soc Am. 2004;116:3546---58.
10.UchidaY, Nomura H, Itoh A, Nakashima T, Ando F,Niino N, etal.Theeffectsofageonhearingandmiddleearfunction.J Epidemiol.2000;101Suppl.:S26---32.
11.WadaH,KoikeT,KobayashiT.Theeffectofaging onmiddle ear dynamiccharacteristics. NipponJibiinkokaGakkaiKaiho. 1994;97:898---904.
12.Holte L. Aging effects in multifrequency tympanometry. Ear Hear.1996;17:12---8.
13.Sogebi OA, Olusoga-Peters OO. Clinical and audiomet-ric features of presbycusis in Nigerians. Afr Health Sci. 2013;13:886---92.
14.Onusko E. Tympanometry. Am Fam Physician. 2004;70: 1713---20.
15.NondahlDM,CruickshanksKJ,WileyTL,TweedTS,DaltonDS. 16-yearchangeinacousticadmittancemeasuresamongolder adults:datafromapopulation-basedstudy.JSpeechLangHear Res.2013.Epubaheadofprint].
16.DoanDE,ErulkarJS, SaundersJC.Functionalchangesinthe agingmousemiddleear.HearRes.1996;97:174---7.
17.Gaihede M,Koefoed-Nielsen B.Mechanics of themiddle ear system:age-relatedchangesinviscoelasticproperties.Audiol Neurootol.2000;5:53---8.
18.GoldingM,DoyleK,SindhusakeD,MitchellP,NewallP, Hart-leyD.Tympanometricandacousticstapediusreflexmeasures inolderadults:theBlueMountainsHearingStudy. JAmAcad Audiol.2007;18:391---403.
19.MaF,QuCY,WangT,YinJ,ZhangXD,MengJ,etal.Studyon hearingimpairmentamongelderlypopulationinthecommunity ofTaiyuancity,Shanxiprovince.ZhonghuaLiuXingBingXueZa Zhi.2009;30:247---51.
20.MaoZ,ZhaoL,PuL,WangM,ZhangQ,HeDZ.Howwellcan centenarianshear?PLOSONE.2013;8:e65565.
21.Cruz MS, Lima MC, Santos JL, Duarte YA, Lebrão ML, Ramos-CerqueiraAT.Self-reportedhearinglossamongelderly individuals in the city of São Paulo, Brazil: prevalence and associated factors (SABE Study, 2006). Cad Saude Publica. 2012;28:1479---92.
22.RuahCB,SchachernPA,ZeltermanD,PaparellaMM,YoonTH. Age-relatedmorphologicchangesinthehumantympanic mem-brane.Alightandelectronmicroscopicstudy.ArchOtolaryngol HeadNeckSurg.1991;117:627---34.
23.Nixon JC, Glorig A, High WS. Changes in air and bone conduction thresholdsas afunction of age.JLaryngol Otol. 1962;76:288---98.
24.OgunleyeAO,LabaranAS.PresbycusisinNigeriansatthe Univer-sityCollegeHospital,Ibadan.AfrJMedMedSci.2005;34:293---6.
25.ArlingerS.Audiometricprofileinpresbycusis.ActaOtolaryngol Suppl.1990;476:85---9.
26.KanekoA,HosodaY,DoiT,TadaN,IwanoT,YamashitaT.Tubal compliance----changeswithageandintubalmalfunction.Auris NasusLarynx.2001;28:121---4.
27.Frisina ST, Mapes F,Kim SH, Frisina DR,Frisina RD. Charac-terizationofhearinglossinagedtypeIIdiabetics.HearRes. 2006;211:103---13.
29.WileyTL,ChappellR,CarmichaelL,NondahlDM,Cruickshanks KJ.Changesinhearingthresholdsover10yearsinolderadults. JAmAcadAudiol.2008;19:281---92.
30.StenfeltS.Middleearossiclesmotionathearingthresholdswith airconductionandboneconductionstimulation.JAcoustSoc Am.2006;119(5Pt.1):2848---58.
31.MargolisRH.Detectionofhearingimpairmentwiththeacoustic stapediusreflex.EarHear.1993;14:3---10.