w w w . r b o . o r g . b r
Original
Article
Total
knee
arthroplasty:
indication
of
blood
transfusion
according
to
hematimetric
variation
and
clinical
symptoms
of
hypoperfusion
夽
,
夽夽
Rodrigo
Tavares
Cardozo
∗,
Edison
Fidelis
de
Souza
Junior,
Wagner
Campoli
Alves,
Flávio
Barbi
Filho
OrthopedicsandTraumatologyService,HospitalSãoFrancisco,RibeirãoPreto,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received12August2013 Accepted12September2013 Availableonline13August2014
Keywords:
Hemoglobin Surgicalbloodloss Joints
Arthroplasty Hypovolemia
a
b
s
t
r
a
c
t
Objective:Toanalyzetherelationshipbetweenhematimetricvariationandthepresenceof clinicalsymptomsofhypoperfusionforindicatingbloodtransfusioninpatientsundergoing totalkneearthroplasty.
Methods:Aretrospectiveanalysiswasconductedondatagatheredfromthemedicalfilesof 55patientswithadiagnosisofgonarthrosis,whounderwenttotalkneearthroplastyata hos-pitalorthopedicsandtraumatologyservicebetweenFebruary2011andDecember2012.The patientsstudiedpresentedunilateraljointdegenerationandfittedintotheindicationsfor surgicaltreatment.Allthepatientsunderwentapreoperativecardiologicalevaluation, pre-sentingapatternofASAI–IIIandabsenceofblooddyscrasia,andpreoperativehemoglobin measurementsweremade.However,nominimumhematimetricvaluewasestablishedfor thesurgicaltreatment;therewereonlyclinicalcriteriaforbloodperfusion.
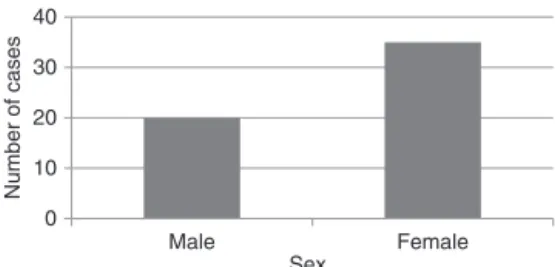
Results:Amongthe55patients,35werefemaleand20weremale,andthemeanagewas 68years.Sixpatientsunderwenthomologousbloodtransfusion,becauseoftheirclinical conditionoftissuehypoperfusion,persistenthypotension,lossofconsciousness,sweating andcoerciblevomiting.Theypresentedpostoperativehemoglobinof7.5–8.8g/dL.
Conclusion: Forpatientswithfallsinhemoglobincountsgreaterthan20%andvalueslower than9g/dLafterthesurgery,thereisapossibleneedforbloodtransfusion,whichshould onlybeindicatedwhenaccompaniedbymajorsymptomsoftissuehypoperfusion.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
Pleasecitethisarticleas:TavaresCardozoR,FidelisdeSouzaJuniorE,CampoliAlvesW,BarbiFilhoF.Artroplastiatotaldojoelho: indicac¸ãodetransfusãosanguíneadeacordocomavariac¸ãohematimétricaeossintomasclínicosdehipoperfusão.RevBrasOrtop. 2014;49(5):507–512.
夽夽
WorkdevelopedattheOrthopedicsandTraumatologyService,HospitalSãoFrancisco,RibeirãoPreto,SP,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](R.TavaresCardozo). http://dx.doi.org/10.1016/j.rboe.2013.09.002
Artroplastia
total
do
joelho:
indicac¸ão
de
transfusão
sanguínea
de
acordo
com
a
variac¸ão
hematimétrica
e
os
sintomas
clínicos
de
hipoperfusão
Palavras-chave:
Hemoglobina
Perdasanguíneacirúrgica Articulac¸ões
Artroplastia Hipovolemia
r
e
s
u
m
o
Objetivo: Analisararelac¸ãoentreavariac¸ãohematimétricaeapresenc¸adesintomas clíni-cosdehipoperfusãoparaaindicac¸ãodetransfusãosanguíneaempacientessubmetidosa artroplastiatotaldojoelho.
Métodos: Fez-se umaanálise retrospectivados dadoscoletados nos prontuários de 55 pacientescomdiagnósticodegonartrosesubmetidosaartroplastiaunilateraltotaldojoelho feitapeloservic¸odeortopediaetraumatologiadeumhospitaldefevereirode2011a dezem-brode2012.Ospacientesestudadosapresentaramdegenerac¸ãoarticularunilateralese enquadraramnaindicac¸ãoparaotratamentocirúrgico.Todosforamsubmetidosaavaliac¸ão pré-operatóriacardiológicaemanteve-seumpadrãocorrespondenteaASA-IatéIII, ausên-ciadediscrasiasanguíneaemensurac¸ãodehemoglobinapré-operatória.Porém,nãofoi estabelecido valorhematimétricomínimoparaotratamentocirúrgico,apenas critérios clínicosdeperfusãosanguínea.
Resultados: Dos55pacientes,35dosexofemininoe20domasculino,commédiade68anos, apenasseisforamsubmetidosatransfusãosanguíneahomóloga,decorrentedoquadro clínicodehipoperfusãotecidual,hipotensãopersistente,perdadaconsciência,sudoresee vômitoscoercíveiseapresentaramhemoglobinapós-operatóriaentre7,5e8,8g/dL.
Conclusão:Pacientescomquedaacimade20%nacontagemdehemoglobinaevaloresabaixo de9g/dLapósacirurgiasugeremumapossívelnecessidadedetransfusãosanguínea,que sódeveserindicadaquandoacompanhadadesintomasmaioresdehipoperfusãotecidual. ©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Totalkneearthroplasty(TKA)isoneofthesurgicalprocedures mostindicatedfortreatingosteoarthrosis,1whichisadisease ofinflammatoryanddegenerativenaturethatcauses destruc-tionofthekneejointcartilageandleadstojointdeformity.2 TKAisanincreasinglycommonprocedure,3–6 butitis asso-ciatedwithmajorpostoperativebloodlossesthatmayreach quantitiesgreaterthanorequalto1.5L.Insuchcases, trans-fusionbecomesinevitable.7,8Thebleedingoccursmainlyafter removalofthetourniquet.9,10
It is understood that in cases of trauma and in large-scale surgicalprocedureslike TKA,inwhichthereisacute bloodloss,oxygenationisthemainindicatorregardingblood volume replacement. Thisis adecisive moment, atwhich replacementshouldbeperformedusingbloodorblood com-ponents,ratherthanbymeansofacellularsolutionsalone. Thus, transfusions can be done using homologous blood donated by another person, or using autologous blood, in whichthedonorandrecipientarethesameperson.Inmost cases, transfusion using homologous blood is done more often.11
However,iftheindicationsfortransfusionsareanalyzed, itisseenthatthereisnoconsensusregardingwhatthe mini-mumacceptablevalueforthehemoglobinlevelwouldbe,for adequatetissueperfusiontobemaintained.Discrepant val-ueshavebeenreported,rangingfromlevelsaslowas1.8g/dL tonormallevelslike12g/dL.12
Thepresentstudyhadtheaimofanalyzingthe relation-shipbetween thehematimetric variationandthe presence
ofclinicalsymptomsofhypoperfusion,forindicatingblood transfusioninpatientsundergoingTKA.
Materials
and
methods
Aretrospectiveanalysiswasconductedondatagatheredfrom themedicalfilesof55patientswhounderwentunilateralTKA, performedattheorthopedicsandtraumatologyserviceofa hospitalbetweenFebruary2011andDecember2012.Among thesepatients,35(63.63%)werefemaleand20(36.36%)were male,andthemeanagewas68.3years(range:45–86),ascan beseeninFig.1.
Alltheprocedureswereperformedbyateamofsurgeons withexperienceofthesurgicaltechniqueofunilateralTKA.
Asinclusioncriteria,thepatientsneededtopresent pri-mary gonarthrosis with an indication for TKA, undergo a preoperative cardiological assessment, remain within cate-goriesI–IIIoftheAmericanSocietyofAnesthesiology(ASA), present absence of blood dyscrasia and have preoperative
0 10 20 30 40
Female Male
Number of cases
Sex
hemoglobinmeasurementsavailable.Nominimum hemati-metric value was established forthe surgery: onlyclinical criteriaforbloodperfusion.Patientswhowereregularlyusing medicationswiththepotentialtoaltertheircoagulationwere advised to suspend their use ten days before the surgical intervention,andallofthepatientspresentednormal coag-ulogramsonthedayoftheprocedure.Anyintraoperativeor postoperativecomplicationwasconsideredtobeanexclusion criterion.
Theantibioticcefazolinwasusedasasingledose of1g intravenously, to induce anesthesia. Prevention of venous thromboembolism followed the guidance of the venous thromboembolismpreventioncommittee,withsubcutaneous administrationof40mgofenoxaparinperday, starting6h afteronsetoftheanestheticblockandcontinuingfortendays. Inallthepatients,theanesthesiaconsistedofalocoregional block and the criterion for transoperative and immediate postoperativevolumereplacementwasrestrictive, compris-ingcrystalloidinfusionattherateof10mL/kg/h.Asepsisand antisepsiswereperformed,withapplicationofspecifictopical solutions,andplacementofappropriatesurgicalfields.
During the surgical procedure, a pneumatic tourniquet withapressureof375mmHgwasused.Thiswaspositioned attherootofthethigh,whichwasprotectedwithorthopedic cottonwoolandacrepebandage.Theconventionaltechnique fortotalkneearthroplastywasfollowed,bymeansofamedian accessrouteandmedialparapatellararthrotomy,eversionof thepatella,disturbanceofthekneeextensormechanism,joint dislocationand extensiveviolation ofthe soft tissues sur-roundingthejoint.13–15Allthepatientsreceivedacemented prosthesis,whichisusedmorefrequentlyfortechnicaland economicreasons.16
After the pneumatic tourniquet had been released, hemostasiswasperformedand aone-way vacuumsuction drainwasplacedinsidethejoint,withitsoutletinthelateral distalregionofthefemur.Suturingwasperformedinlayers, withcompleteflexion–extensionmovementsmadeafter clos-ingeachlayer.Dressingswereappliedfromtheinguinalregion tothefoot,consistingofsuccessivelayersofcompressive ban-dagesandorthopediccottonwool,followedbyaplaster-cast splintextendingfromtheinguinalregiontothemalleolus.
Volumereplacementwithcrystalloidswasperformed in theward,withobservanceofarationof3:1forthebloodlosses collectedthroughthevacuumdrainandtheestimateddaily lossintothedressings.Hemoglobincontrolwasapplied24h aftertheendofthesurgicalprocedure,giventhatthisisthe idealtime,sinceitcorrespondstothetimeofgreatervolume drainedthroughthe draincollectorsystem.Afterthistime, thevolumebecomesinsignificant.17
Thelengthofhospitalstaywasthreedays.Isometricand isotonicexerciseswereperformedontheentirelowerlimb, beginningonthefirstpostoperativedayandcontinuinguntil dischargefromhospital.Theaimsweretoachieveactive flex-ionofatleast90◦,completeextensionandwalkingwithpartial weight-bearing,withtheaidofawalkingframe.
Results
Inevaluatingthehemoglobinlevelsafter24h,itwasobserved thatthemeanlosswas3.33g/dL(24.78%),witharangefrom0.5
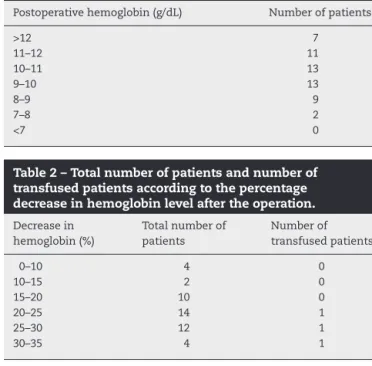
Table1–Numberofpatientsaccordingtothe postoperativehemoglobinassayvalue.
Postoperativehemoglobin(g/dL) Numberofpatients
>12 7
11–12 11
10–11 13
9–10 13
8–9 9
7–8 2
<7 0
Table2–Totalnumberofpatientsandnumberof transfusedpatientsaccordingtothepercentage decreaseinhemoglobinlevelaftertheoperation.
Decreasein hemoglobin(%)
Totalnumberof patients
Numberof transfusedpatients
0–10 4 0
10–15 2 0
15–20 10 0
20–25 14 1
25–30 12 1
30–35 4 1
to6.3g/dL.Thepostoperativehemoglobinassayrangedfrom 7.5to12.7g/dL,andmostofthepatients(67.27%)presented levelsbetween9and12g/dL(Table1).
ToviewthedatapresentedinTable1better,ahistogramof frequenciesofnumbersofpatientswasconstructedaccording tothepostoperativehemoglobinassayvalues(Fig.2).
Thepercentagereductioninhemoglobinlevelrangedfrom 5.55%to40.91%.Mostofthepatients(36)presentedadecline, whichrangedfrom15%to30%.Allthepatientswhoreceived transfusionspresentedpercentagesgreater than20%. How-ever, 39 patients presented percentagelosses greater than 20%andonlysix(15.38%)receivedtransfusions,asshownin
Table2.
Thetotalnumber ofpatientsand numberoftransfused patientsaccordingtothepercentagedeclineinhemoglobin levelsaftertheoperationcanbeseeninFig.3.
Six patients (10.9%) underwent exclusively homologous bloodtransfusion,becausetheypresentedsymptomsof tis-sue hypoperfusion, suchaspersistent hypotension,lossof consciousness, coldsweating,coercible vomitingand men-tal confusion. The criteria of hematimetric variation were notdeterminants forthetransfusions.However,in analyz-ingthevalues,weobservedthatallthetransfusedpatients
0 2 4 6 8 10 12 14
Number of patients
Postoperative hemoglobin (g/dL)
>12 11 to 12 10 to 11 9 to 10 8 to 9 7 to 8 <7
0 2 4 6 8 10 12 14
>40% 35 to 40% 30 to 35%
25 to 30% 20 to 25%
15 to 20% 10 to 15%
0 to 10%
Percentage decrease in hemoglobina
Total number of patients Number of transfused patients
Fig.3–Totalnumberofpatientsandnumberoftransfusedpatientsaccordingtothepercentagedecreaseinhemoglobin valueaftertheoperation.
presentedpostoperativehemoglobincountsthatrangedfrom
7.5to8.8g/dL(Table3).Itshouldbeemphasizedthatother
patients withpostoperative hemoglobincounts lower than 8.8g/dLdidnothavetheneedfortransfusion,sincetheydid notpresentclinicalsymptomsofhypoperfusion(Table1).
Dischargefromhospitalwasdelayed byonedayforthe patients who underwent transfusions. However, no other complicationswereobserved.
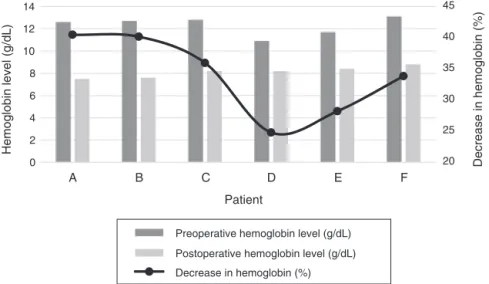
Thebehaviorofthepatientswhounderwentblood trans-fusion, regarding their pre and postoperative hemoglobin levelsandthe percentagereductions,canbeseenbetterin
Fig.4.
Discussion
Blood loss during TKA may lead patients to the need to undergotransfusion.However,thereisnoconsensusinthe pertinentliteratureregardingtheindicationsfortransfusion accordingtohemoglobinlevels.
ItisworthrecallingtheobservationmadebyVuille-Lessard et al.18 that doctors do not have definitive indications or supportguidelines forthe needforblood transfusion after orthopedicsurgery,whichultimatelyresultsinadiversityof levelsusedintransfusionpractice.
Inanalyzing blood management in patients undergoing totalkneeorhiparthroplasty, Bierbaumet al.19 statedthat theirstudy wasthe firsttoprospectivelyassess therole of
hemoglobinaccordingtoitslevelsorspecificcategories.They evaluatedtheneedforautologousorhomologoustransfusion based on the initialhemoglobin level. Patients whose pre-operativehemoglobin levelwas 13g/dL or lesswould need a homologous blood transfusion, particularly those whose initial hemoglobin level was between 10 and 13g/dL. Sub-sequently, Billote et al.20 made a complete review of the manuscriptofBierbaumetal.19anddisagreedwiththe origi-nalresult,withthejustificationthatthecategoryofpatients withinitialhemoglobinlevelsfrom10to13g/dLpresentedin thatstudywasverybroad,inthatitmixedanemicand non-anemicelderlyindividualsandothereligibledonors.Alsoin Billoteet al.,20Bierbaumetal.repliedandstated thatfrom theconceptualpointofview,theintervalof10–13g/dLintheir studywasbasedoninformationfromtheWorldHealth Orga-nization(WHO).Bierbaumetal.19agreedwithBilloteetal.20 instatingthatadditionalinvestigationsofbloodmanagement strategiesinthesesurgicalprocedureswerenecessary.
Inthis regard,Nget al.21 madereferencetothe studies ofSalidoetal.22andHatzidakisetal.,23andstatedonlythat patientswithpreoperativehemoglobinlevelslessthan13g/dL arefourtosixtimesmorelikelytoneedtransfusionthanare patientswithhemoglobinlevelsbetween13and15g/dLand 15timesmorelikelythanthosewithalevelof15g/dL.
In the present study, it was observed that among the patients who underwent blood transfusion, only one of thempresentedapreoperativehemoglobinlevellowerthan 11g/dL,whiletheothers(totaloffive)presentedpreoperative
Table3–Preandpostoperativehemoglobinlevelsandpercentagedecreasesinpatientswhounderwentblood transfusion.
Transfusedpatient Preoperativehemoglobinlevel(g/dL) Postoperativehemoglobinlevel(g/dL) Decreaseinhemoglobin(%)
A 12.6 7.50 40.47
B 12.7 7.60 40.16
C 12.8 8.20 35.94
D 10.9 8.20 24.77
E 11.7 8.40 28.20
20 25 30 35 40 45
0 2 4 6 8 10 12 14
F E
D C
B A
Hemoglobin level (g/dL)
Decrease in hemoglobin (%)
Patient
Preoperative hemoglobin level (g/dL)
Postoperative hemoglobin level (g/dL)
Decrease in hemoglobin (%)
Fig.4–Preandpostoperativehemoglobinlevelsandpercentagedecreaseinpatientswhounderwentbloodtransfusion.
hemoglobinlevelsbetween12.6and13.1g/dL.Thiswasnot thedecisivefactorforindicatingtransfusion.
Regarding postoperative hemoglobin levels, in another study24ontheuseoftourniquetsinTKAcasesintwogroups ofpatients(withandwithoutatourniquet),itwasreported that two patients ineach group underwent blood transfu-sionaftertheoperation.Onepatientunderwenttransfusion whenahemoglobinlevelof8.3g/dLwaspresented, accompa-niedbytachycardiaandmilddyspnea,whiletheotherthree presentedlowhemoglobinlevels(7.2,7.6and7.7g/dL). The meandecreaseinhemoglobinlevelforthesefourpatientswas 4.1g/dL.
Inthe presentstudy,it wasobservedthat all the trans-fusedpatientspresentedpostoperativehemoglobincountsof between7.5and8.8g/dL.However,otherpatientswith post-operativehemoglobincountslowerthan8.8g/dLdidnotneed transfusion,giventhattheydidnotpresentclinicalsymptoms ofhypoperfusionandthehematimetricvariationcriteriawere notdeterminantforthetransfusions.
Other authors25 who studiedtransfusions ofautologous and homologous blood in TKA surgery cases made com-parisonsthrough distributingthe patientsinto twogroups: thosewhoreceivedhomologousbloodtransfusionsandthose who received autologous blood transfusions.They empha-sized that the indication for transfusion for both groups waswhenthepatientpresentedapostoperativehemoglobin levelof8.5g/dL.Theyalsopointedout thattheirstudyhad some limitations and explained that although the recom-mendation from local studies was 8.5g/dL, this was not always followed by some surgeons, who were still reluc-tant to apply this because they thought that it was too low.
These authors25 took the view that this was the expla-nation for higher hemoglobin levels in the homologous transfusiongroup,whichwasnotseenintheautologousgroup becausetheprotocolforthiswascontrolledbythetechnique andtheanesthesiabytheanesthesiologist.
Inthepresent study,theviewtaken wasthat, unlikein thecasesoftheaboveauthors,25thepatientswhounderwent homologous blood transfusion received this solelybecause
theypresentedsymptomsoftissuehypoperfusion.The hema-timetric variation criteria were not determinants for the transfusions.
In acomparativestudy on bloodtransfusion practicein elective surgical procedures in three hospitals in France, Vuille-Lessardetal.18concludedthatingeneral,thepatients receivedtransfusionswhentheypresentedhemoglobinlevels ofbetween7.5and8.0g/dL.Thereweresignificantdifferences betweenthehospitals,regardingthedistributionofthe proce-dures,hemoglobinlevelsandbloodlosses,andalsoinrelation tothedecreaseinhemoglobinlevelsanddurationofthisstate. Theseauthorsstatedthatin85%ofthetransfusions,onlythe hemoglobinlevelwasenvisaged.
Inthepresentstudy,themajorityofthepatients(67.27%) presented postoperative hemoglobin levels between 9 and 12g/dL, and none of them required transfusion. However, amongthe11patientswithpostoperativehemoglobinlevels lowerthan9g/dL,six(54.54%)requiredtransfusion.Inother words,patientswithhemoglobinlevelslowerthan9g/dL fol-lowing TKAsurgerypresentedtwiceasmuchpossibilityof needingbloodtransfusion.Thishemoglobinvaluewasshown tobeaminimumthresholdforpossibletransfusion,inrelation toclinicalsymptoms.
Also in the present study, the majority of the patients (65.45%)presentedpercentagedecreasesinhemoglobin lev-elsrangingfrom15%to30%.However,amongthetransfused patients alone, the mean percentagewas greater (33.84%), witharangefrom24.77%to40.47%.
Intotal,therewere39patientswithachangeofmorethan 20%, but only 15.38% required transfusion.Thus, it seems thatindicatingbloodreplacementaccordingtothe percent-agehematimetriclossisnotanappropriatecriterionforuse inclinicalpractice,sincenostandardthatwouldorwouldnot justifybloodtransfusionwasfound.
Conclusion
suggestsapossibleneedforbloodtransfusion,whichshould onlybeindicatedwhenaccompaniedbygreatersymptomsof tissuehypoperfusion.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. CintraFF,YepézAK,RasgaMGS,AbaggeM,AlencarPGC.
Componentetibialnarevisãodaartroplastiadojoelho:
comparac¸ãoentrefixac¸ãocimentadaehíbrida.RevBras
Ortop.2011;46(5):585–90.
2. CamanhoGL.Tratamentodaosteoartrosedojoelho.RevBras
Ortop.2001;36(5):135–40.
3. IamaguchiMM,HelitoCP,GobbiRG,DemangeMK,TiricoLEP,
PecoraJR,etal.Valordaavaliac¸ãoradiográficapré-operatória
dosdefeitosósseosnojoelhonasrevisõesdeartroplastia.Rev
BrasOrtop.2012;47(6):714–8.
4. KhatodM,InacioM,PaxtonEW,BiniSA,NambaRS,Burchette
RJ,etal.Kneereplacement:epidemiology,outcomes,and
trendsinSouthernCalifornia:17,080replacementsfrom1995
through2004.ActaOrthop.2008;79(6):812–9.
5. WellsVM,HearnTC,McCaulKA,AndertonSM,WiggAE,
GravesSE.Changingincidenceofprimarytotalhip
arthroplastyandtotalkneearthroplastyforprimary
osteoarthritis.JArthroplasty.2002;17(3):267–73.
6. PugelyAJ,MartinCT,GaoY,Mendoza-LattesS,CallaghanJJ.
Differencesinshort-termcomplicationsbetweenspinaland
generalanesthesiaforprimarytotalkneearthroplasty.JBone
JointSurgAm.2013;95(3):193–9.
7. LotkePA,FaralliVJ,OrensteinEM,EckerML.Bloodlossafter
totalkneereplacement.Effectsoftourniquetreleaseand
continuouspassivemotion.JBoneJointSurgAm.
1991;73(7):1037–40.
8. SinghVK,SinghPK,JavedS,KumarK,TomarJ.Autologous
transfusionofdraincontentsinelectiveprimaryknee
arthroplasty:itsvalueandrelevance.BloodTransfus.
2011;9(3):281–5.
9. AndradeMAP,CamposTVO,SilvaBFA,AssisME,BoechatLC,
BiondiLF,etal.Avaliac¸ãoprospectivadospacientes
submetidosaartroplastiatotaldojoelhocomesemcolocac¸ão
dedrenodesucc¸ão.RevBrasOrtop.2010;45(6):549–53.
10.BurkeDW,O’FlynnH.Primarytotalkneearthroplasty.In:
ChapmanMW,editor.Chapman’sorthopedicsurgery.
Philadelphia:LippincottWilliams&Wilkins;2001.p.2870–95.
11.VaneLA,GanemEM.Doac¸ãohomólogaversusautólogae
substitutosdahemoglobina.In:CavalcantiIL,CantinhoFAF,
AssadAR,editors.Medicinaperioperatória.RiodeJaneiro:
SociedadedeAnestesiologiadoEstadodoRiodeJaneiro;
2006.p.291–306.
12.HajjarLA,AulerJOCJr,SantosL,GalasF.Bloodtransfusionin
criticallyillpatients:stateoftheart.Clinics.
2007;62(4):507–24.
13.MottaFilhoGR,CavanellasN.Artroplastiaminimamente
invasivadojoelho.RevBrasOrtop.2007;42(9):269–77.
14.ScottRD,VolatileTB.Twelveyears’experiencewithposterior
cruciate-retainingtotalkneearthroplasty.ClinOrthopRelat
Res.1986;(205):100–7.
15.MalkaniAL,RandJA,BryanRS,WallrichsSL.Totalknee
arthroplastywiththekinematiccondylarprosthesis:a
ten-yearfollow-upstudy.JBoneJointSurgAm.
1995;77(3):423–31.
16.CobraHAAB,PalmaIM.Artroplastiatotaldojoelho.
SEMCAD/PROATO/SBOT-SociedadeBrasileiradeOrtopediae
Traumatologia.PortoAlegre:Artmed/Panamericana;2008.
17.LopesAIS,CobraHAAB,CavanellasNT.Avaliac¸ãodaperda
sanguíneaemartroplastiatotalprimáriadojoelhocom
drenagemdesucc¸ão:estudoprospectivo.Orto&Trauma:
DiscussõeseComplicac¸ões.2009;(6):4–6.
18.Vuille-LessardE,BoudreaultD,GirardF,RuelM,ChagnonM,
HardyJF.Redbloodcelltransfusionpracticeinelective
orthopedicsurgery:amulticentercohortstudy.Transfusion
(Paris).2010;50(10):2117–24.
19.BierbaumBE,CallaghanJJ,GalanteJO,RubashHE,ToomsRE,
WelchRB.Ananalysisofbloodmanagementinpatients
havingatotalhiporkneearthroplasty.JBoneJointSurgAm.
1999;81(1):2–10.
20.BilloteDB,BierbaumBE,CallaghanJJ,GalanteJO,RubashHE,
ToomsRE,etal.Analysisofbloodmanagement.JBoneJoint
SurgAm.2000;82(6):900–1.
21.NgVY,LustenbergerD,HoangK,UrchekR,BealM,Calhoun
JH,etal.Preoperativeriskstratificationandriskreductionfor
totaljointreconstruction:AAOSexhibitselection.JBoneJoint
SurgAm.2013;95(4):e191–215.
22.SalidoJA,MarínLA,GómezLA,ZorrillaP,MartínezC.
Preoperativehemoglobinlevelsandtheneedfortransfusion
afterprosthetichipandkneesurgery:analysisofpredictive
factors.JBoneJointSurgAm.2002;84(2):216–20.
23.HatzidakisAM,MendlickRM,McKillipT,ReddyRL,GarvinKL.
Preoperativeautologousdonationfortotaljointarthroplasty.
Ananalysisofriskfactorsforallogenictransfusion.JBone
JointSurgAm.2000;82(1):89–100.
24.TaiTW,ChangCW,LaiKA,LinCJ,YangCY.Effectsof
tourniquetuseonbloodlossandsoft-tissuedamageintotal
kneearthroplasty:arandomizedcontrolledtrial.JBoneJoint
SurgAm.2012;94(24):2209–15.
25.SarkanovicML,GvozdenovicL,SavicD,IlicMP,JovanovicG.
Autologousbloodtransfusionintotalkneereplacement