w w w . r b o . o r g . b r
Original
Article
Intra
and
interobserver
concordance
between
the
different
classifications
used
in
Legg–Calvé–Perthes
disease
夽
André
Cicone
Liggieri
∗,
Marcos
Josei
Tamanaha,
José
Jorge
Kitagaki
Abechain,
Tiago
Moreno
Ikeda,
Eiffel
Tsuyoshi
Dobashi
DisciplineofPediatricOrthopedics,EscolaPaulistadeMedicina,UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received2September2014 Accepted26September2014 Availableonline29October2015
Keywords: Hip/radiography Legg–Calvé–Perthes disease/classification Legg–Calvé–Perthes disease/radiography Osteonecrosis
a
b
s
t
r
a
c
t
Objective:The aimofthisstudy wastodeterminetheintra andinterobserver concord-anceratesoftheWaldenström,CatterallandHerringclassificationsforLegg–Calvé–Perthes disease.
Methods:OnehundredradiographsofthepelvisinanteroposteriorandLauensteinviews, frompatientswiththisdisease,wereselected.Theradiographswereclassifiedbyfour physi-cianswithdifferentlevelsofexperiencewhohadpreviouslybeengivenguidanceregarding theclassificationsused,inordertominimizeanybiasofinterpretation.Theradiographs wereexaminedbythesameobserversattwodifferenttimesinordertoevaluatetheintra andinterobserverconcordance.Reproducibilitywasassessedusingthekappaindex. Results:Theconcordanceanalysiswasstratifiedintolevels (poor,slight,fair,moderate, goodandexcellent).Theintraobserveranalysisshowed,fortheWaldenström classifica-tion,moderateconcordanceforthreeexaminersandfairforone;forHerring,excellentfor oneexaminerandgoodforthree;andforCatterall,goodforalltheexaminers.The inter-observeranalysisshowed:forthethreeclassificationsystems,nosituationsofexcellent concordance;forWaldenström,foursituationsoffairconcordance,onemoderateandone slight;forHerring,foursituationsofmoderateconcordance,onegoodandonefair;andfor Catterall,foursituationsofmoderateconcordanceandtwofair.
Conclusion:Theclassificationsstudiedaretheonesmostusedforguidingthetreatmentfor Legg–Calvé–Perthesdisease,butthedegreeofintraandinterobserverconcordanceisfar fromideal.Complementarystagingsystemsneedtobetakenintoconsideration,sothat therecanbegreatercertaintyregardingthetreatment.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkperformedonthedatabaseofimagesofpatientsattendedwithintheDisciplineofPediatricOrthopedics,EscolaPaulistade Medicina,UniversidadeFederaldeSãoPaulo(UNIFESP),SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](A.C.Liggieri). http://dx.doi.org/10.1016/j.rboe.2015.09.010
Concordância
intra
e
interobservadores
das
diferentes
classificac¸ões
usadas
na
doenc¸a
de
Legg–Calvé–Perthes
Palavras-chave: Quadril/radiografia Doenc¸ade
Legg–Calvé–Perthes/classificac¸ão Doenc¸ade
Legg–Calvé–Perthes/radiografia Osteonecrose
r
e
s
u
m
o
Objetivo: Determinaroíndicedeconcordânciaintraeinterobservadoresdasclassificac¸ões deWaldenström,CatteralleHerringnadoenc¸adeLegg–Calvé–Perthes.
Métodos: Foramselecionadas100radiografiasdabacia,nasincidênciasanteroposteriore deLauensteindepacientesportadoresdadoenc¸a.Asradiografiasforamclassificadaspor quatromédicoscomdiferentesníveisdeexperiência,previamenteorientadosarespeito dasclassificac¸õesusadas,paraminimizarqualquerviésdeinterpretac¸ão.Asradiografias foramexaminadaspelosmesmosobservadoresemdoismomentosdistintosparaavaliar asconcordânciasintereintraobservadores.Aanálisedareprodutibilidadefoiavaliadapelo índicedeKappa.
Resultados: A análisede concordânciafoi estratificada em níveis(ruim, pequena, reg-ular, moderada,boa e excelente) e evidenciou paraa concordância intraobservadores: concordânciamoderada paratrêsexaminadores e umaregularparaa classificac¸ão de Waldenström;excelenteparaumexaminadoreboaparatrês,naclassificac¸ãodeHerring; naclassificac¸ãodeCatterall,a concordânciafoiconsideradaboaentretodosos exami-nadores.Emrelac¸ãoàanálisedeconcordânciasinterobservadoresforamobtidas:nenhuma concordânciaexcelenteparaostrêssistemasdeclassificac¸ão;quatroregulares,uma mod-eradaeumapequenaparaaclassificac¸ãodeWaldenström;quatromoderadas,umaboae umaregularnaclassificac¸ãodeHerringe,pelosistemadeCatterall,quatroconcordâncias moderadaseduasregulares.
Conclusão: Asclassificac¸õesestudadassãoasmaisusadas paraguiarotratamentoda DLCP,porém ograude concordânciaintra e interobservadoresnãoé ideal esistemas complementaresdeestadiamentodevemserlevadosemconsiderac¸ão,paraumamaior assertividadenotratamento.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
In1910,Legg–Calvé–Perthesdisease(LCPD)wasdescribedfor thefirsttime.Sincethen,ithasarousedgreatinterestamong researchersandhascometobeoneofthemostcontroversial topicsintheorthopedicliterature.Severalaspectsofthis clin-icalentitystillremainunexplained,suchasitsetiologyand thebestwayoftreatingitintheactivephaseofthedisease.
Foralongtime,almostallauthorsconcentratedon ana-lyzing the radiographic aspects of LCPD. The evolutionary phaseswerefirstdescribedbyWaldenström,1whose classi-ficationwassubsequentlysimplifiedandcorrelatedwiththe anatomopathologicalfindingsbyJonsäter.2Evaluationsonthe compromisingofthenucleusofossificationofthe femoral headcametobesystematizedbyCatterall,3 basedon anal-ysis on simple radiographs produced during the phase of maximumfragmentation.Withtheaimofdeterminingthe proportionsoflesionsduringtheinitialphaseorthe necro-sisphase,SalterandThompson4demonstratedthatthesize ofthesubchondralfractureintheLauensteinviewprecisely reflectedthedegreetowhichtheproximalfemoralepiphysis wasaffectedbythedisease.Morerecently,Herringetal.5 pro-posedanewclassificationbasedontheheightofthelateral columnofthefemoralepiphysis.Otherclassificationshave beenproposed,butthe onescitedabovearethose thatare mostusedtoday.
From radiographic analyses on the hips of affected patients,alloftheseauthorsdevelopedclassificationsforuse incasesofLCPDandthussoughttosystematizethetreatment. However,foragivenclassificationtobeconsideredadequate, it needstobereproducible,i.e.thereneedstobeinter and intraobserver concordance,and furthermore, the classifica-tionsystemneedstoaidinguidingdiseaseoutcomes.
AlthoughthetreatmentofLCPDhasbeenthe subjectof exhaustivediscussionsamongorthopedists,thereisstillno clearevidenceregardingthebesttherapeuticmethodforthese patients,andthisisnotwithinthescopeofthepresentstudy. The objective of this study was to evaluate the intra and interobserver concordance of the classifications of Waldenström,1Catterall3andHerringetal.,5attemptto estab-lishwhichofthemhasthegreatestdegreeofreproducibility andthusfacilitatetherapeuticdecision-making.
Materials
and
methods
Thisresearch projectwassubmitted totheresearch ethics committeeoftheBrazilPlatformandwasapprovedfor imple-mentationunderthenumbersCAAE33513214.7.0000.5505and CEP418466.
Lauensteinviews.Aconveniencesampleof100radiographsof patientswithLCPDwascollected.Theseexaminationswere selectedfrom a database withintheDiscipline ofPediatric Orthopedics, relating to patients attended at the orthope-dicsandtraumatologyoutpatientclinicofHospitalSãoPaulo. Theradiographswereselectedbytwoorthopedistswhodid not participate in the disease classification process, such thatgood-quality examinationswere includedand abroad spectrumoflesionswastakenintoconsideration.Withthe aimofminimizingbiasduetodifficultiesininterpretingthe examinations, the observers were provided with an initial explanationoftheclassificationsystemsusedinthisstudy. Furthermore,theprotocol usedforthedata-gathering con-tained adiagramcontainingimages fromthe classification systemsofWaldenström1(asmodifiedbyJonsäter2),Catterall3 andHerringetal.5
Inordertodeterminetheinterobserverconcordance,each of the four researchers evaluated the radiographic exam-inations independently. The different examiners were not allowedtohavepriorknowledgeregardingthepatients’ his-toriesoranyclinicalinformationabouthowthediseasewas addressedor treated. The examinerswere allowed totake all the time that theyneeded to evaluateall ofthe radio-graphs.Aftermakingtheclassifications,theevaluatorswere asked toclassify all the examinationsagain, 30 days after thefirstanalysis,withouthavingaccesstothefirstroundof evaluations.
Theparticipantswereinstructednottodiscussthe classifi-cationsystemsbetweeneachotheruntilafterallthematerial tobeanalyzedinthisstudyhadbeengathered.
Thestatistical analysisontheresultsobtainedwas per-formedbyaprofessionalwithinthefieldofmedicalstatistics. Thedatacollected were analyzedwithregard tointer and intraobserver concordance, by means of the kappa index. ThetestswereinterpretedasdescribedbyAltman,6as “pro-portionalagreementwithcorrectionforchance”.Kappaisa coefficientofconcordancethathasvaluesrangingfrom +1 (perfectconcordance),passingthrough0(concordanceequal to chance) and going to −1 (complete discordance). There
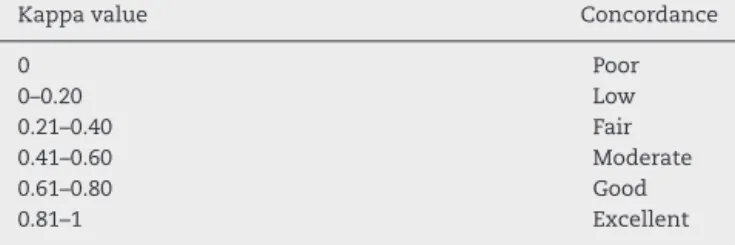
arenodefinitionsregardingwhichconcordancelevelsshould be accepted, but in the study by Svanholm et al.,7 it was indicatedthat concordancegreater than 0.75 isconsidered excellent,0.5–0.75goodandless than 0.5ispoor. However, weusedtheintervalsforthekappaindexthatareshownin Table1.
Table1–Correlationbetweenthekappavalueandthe degreeofconcordance.
Kappavalue Concordance
0 Poor
0–0.20 Low
0.21–0.40 Fair
0.41–0.60 Moderate
0.61–0.80 Good
0.81–1 Excellent
P,poor;L,low;F,fair;M,moderate;G,good;E,excellent.
Results
Table2showstheabsolutefrequenciesoftheclassifications madebytheexaminersatthetwodifferentevaluationtimes ontheradiographsstudied.
Table3showsthedistributionoftheweightedkappavalues andthe95%confidenceintervalsoftheintraobserver concord-anceanalysis.Inthisanalysis,moderateagreementforthree examinersandfairagreementforoneexaminerwereobtained throughapplicationoftheWaldenströmclassification.From theHerringclassification,therewasanexcellentresultforone examinerandgoodagreementforthreeexaminers.Inrelation totheCatterallclassification,alltheresultspresentedgood agreement.
Table4showstheresultsrelatingtoagreementbetween theobserversaccordingtokappavalueswith95%confidence intervals. According to the statistical analysis, no casesof excellentinterobserverconcordancewerefound.Therewere fourresultsinwhichtheconcordancewasfair,onemoderate andonelow,intheWaldenströmclassification.Inrelationto theHerringclassification,fourcasesofmoderate,onegood andonefairagreementwereobtained.Inrelationtothe Cat-terallclassification,therewere fourindexeswithmoderate agreementandtwowithfairagreement.
Discussion
ThechallengefororthopedistsinrelationtoLCPDliesin treat-ing this condition. There hasbeen muchdiscussion about whetherthereisorisnotanydefinitivepossibilityofaltering whatCatterall3calledthenaturalhistoryofthedisease.
Therehasalsobeenmuchdiscussionregardingthe treat-mentthatshouldbeapplied.Becauseofthelackofconvincing evidenceregardingtheeffectivenessoftherapies,these con-ceptshavebeenappliedoverthecourseoftheyears,basedon eachauthor’sexperienceofdiagnosing,classifyingand man-agingLCPD.
Weare convinced that, todealwithLCPD correctly,the diagnosisneedstobesystematizedandtheapproachesused needtobebasedespeciallyonclassificationsthatdirectus towardappropriatetreatment.Sofar,thishasbeendoneon thebasisoftheclassificationsassessedinthisstudy.
Therefore,webelievethatthefirststeptobetaken,after the diagnosis of LCPDhas been established, isto attempt toproperlystageit,usingclassical methodologiesbasedon radiographicanalysesandalsoonmagneticresonance imag-ing,arthrographyandscintigraphywhennecessary.
With the aimof dealing with LCPD from a therapeutic pointofview,wefoundthatseveralauthorsintheliterature proposed classificationsthatwouldallowthis diseasetobe systematizedsoastobeabletopredictwhichapproachwould bethebestonetouse,withtheexpectationofthusobtaining betterresults.
Table2–Weightedkappaand95%CIvaluesfortheintraobserverassessment.
Observer Waldenström Herring Catterall
A 0.44(M) 0.82(E) 0.79(S)
(0.31;0.58) (0.74;0.90) (0.70;0.88)
B 0.32(C) 0.73(S) 0.69(S)
(0.18;0.45) (0.63;0.83) (0.59;0.78)
C 0.53(M) 0.77(S) 0.72(S)
(0.38;0.69) (0.67;0.87) (0.62;0.81)
D 0.52(M) 0.71(S) 0.65(S)
(0.38;0.65) (0.62;0.80) (0.55;0.75)
Table3–Weightedkappaand95%CIvaluesfortheinterobserverassessment.
Classification
Obs1 Obs2 Waldenström Herring Catterall
A B 0.30(C) 0.63(S) 0.41(M)
(0.15;0.45) (0.52;0.74) (0.31;0.52)
C 0.35(C) 0.49(M) 0.30(C)
(0.20;0.50) (0.35;0.63) (0.18;0.42)
D 0.38(C) 0.53(M) 0.32(C)
(0.25;0.52) (0.40;0.65) (0.21;0.44)
B C 0.29(C) 0.41(M) 0.46(M)
(0.14;0.45) (0.28;0.54) (0.34;0.57)
D 0.47(M) 0.54(M) 0.47(M)
(0.33;0.61) (0.41;0.66) (0.36;0.58)
C D 0.23(Pq) 0.39(C) 0.44(M)
(0.08;0.39) (0.27;0.51) (0.32;0.56)
Initially,theclassificationsystemthatmostpolarizedthe attentionofotherauthorsintheorthopedicliteraturewasthe oneproposedbyCatterallin1971.3Thisauthor radiographi-callyassessedthebehaviorofthenucleusofossificationof thefemoralheadduringtheprogressionofthedisease,atthe phaseofmaximumfragmentation.
Thisclassification was contested by several researchers whousedit.Whilesomeauthorsthoughtthatitwasof fun-damentalimportanceforindicatingthetherapythatshould befollowed andthat it had apositivecorrelation withthe
finalresults,8–10otherscriticizeditbecauseitisappliedatan advancedstageofthediseaseandhasquestionable concord-ancewhenusedbydifferentobservers.Allofthesecriticisms were cited by Terjesen et al.11 Despite the reported dis-cordance between observers,many authors haveused this systemtoguidethetherapythatistobeinstituted.However, given that we did not find any excellent or good agree-ment, it is possible that the therapeutic indications may becomedistortedaccordingtothegradationimposedbythis system.
Table4–Absolutefrequenciesoftheobservers’classificationsinthetwoevaluations.
Observers
Classification A B C D
Eval1 Eval2 Eval1 Eval2 Eval1 Eval2 Eval1 Eval2
Waldenström
1 24 14 14 9 14 10 13 8
2 44 29 35 27 38 32 33 33
3 16 38 23 30 30 40 22 31
4 17 20 29 35 19 19 33 29
Herring
1 29 29 23 25 26 24 28 23
2 48 45 51 46 55 56 34 39
3 9 12 8 13 14 13 23 21
4 15 15 19 17 6 8 16 18
Catterall
1 48 42 31 27 24 20 41 35
2 26 31 30 38 31 22 21 21
3 17 18 29 20 27 35 25 28
Because the classification proposed by Salter and Thompson4 isusedataninitialstageofthedisease,itmay perhapsallowearlytreatment.However,itpresentsthe limita-tionthatonly25%ofthepatientswithLCPDhavesubchondral fracturesthatarerecognizableonradiographs.5,12
IncomparisonwiththeclassificationofCatterall,3thatof Herringetal.5iseasiertointerpret.However,sincethis sys-temtoocanonlybeusedatthefinalfragmentationphase,we taketheviewthatitwouldnotbeidealforindicatingearly treatment.12 Sincethetimeoftheinitialdescriptionofthis classification,whichwaspresentedin1994,andbecauseof thedifficulty ofdefining thepatientsbelongingtogroupB, anotherthreesubgroupswerecreated,whichthusallowedthe classificationtohavewidercoverage.
Inourstudy,weobtainedfourmoderate,onegoodandone fairagreementfromtestingthesystemofHerringetal.5This suggeststhatthereissomedifficultyinpreciselydefiningeach ofthegroupsandsubgroups.
Anotherimportantmatteristhatsimpleradiographydoes not precisely mirror what happens to the femoral epiph-ysis.Cartilaginoustissue,whichalsoshowsalterationscaused by this disease, is present in greater amounts than bone tissue.13–15 In this light, in some cases,particularly in the earlystagesofthedisease,studyingthiscartilagebymeans ofmagneticresonanceimaging2,16,17and pneumoarthrogra-phy of the joint13,14 may provide greater clarification and more effective guidance for the treatment that is to be instituted.4,14,15,18–20
Therefore,weconsiderthatknowledgeofthebehaviorof thecartilaginousstructuresofthehipisfundamentalfor stag-ingLCPDandindicatingtheappropriatetreatment.4,14,15,18–20 We believe that magnetic resonance imaging currently presentsavarietyofadvantagesoverotherexaminations.This isadvocatedinseveralstudiesinwhichsomeauthors devel-opedtheirownclassificationswiththeaimofindicatingthe therapywithahigherproportionofcorrectchoices.
Althoughwefoundacertaindegreeofintraobserver con-cordance in the three classification systems studied, and interobserverconcordanceintwoofthe threesystems, our dataarenotinagreementwithwhatwehaveobservedinthe worldwideliterature.
Most of the studies observed did not demonstrate this degreeofconcordance.Onelikelycauseforthisdivergence mayrelatetothelowaveragenumberofpatientsstudiedinthe literature(40),21–23incomparisonwiththenumberofpatients inthepresentstudy(100).
Unfortunately,althoughmostexperiencedsurgeons24use theclassificationsstudiedheretodeterminetheapproaches thattheywilluse,theconcordanceobservedafterstatistical analysiswasnotshowntobesufficientforthis.Therefore,this shouldnotbethesolefactor takenintoaccountinmaking therapeuticdecisionsrelatingtopatientswithLCPD.
Conclusion
1. Theintraobserver concordanceanalysis with95% confi-denceintervalsshowedthefollowingthroughthekappa index: moderate concordance for three observers and fairforone,inthe Waldenströmclassification;excellent
concordanceforoneexaminerandgoodforthree,inthe Herringclassification; and good concordancefor all the examiners,intheCatterallclassification.
2. Theinterobserver concordance analysiswith95% confi-denceintervalsshowedthefollowingthroughthekappa indexafterstatisticalanalysis:noexcellentconcordance foranyofthe threeclassificationsystems;four fair,one moderate and onelow agreement forthe Waldenström classification;fourmoderate,onegoodandonefair agree-mentfortheHerringclassification;andfourmoderateand twofairagreementsfortheCatterallclassification. 3. Althoughtheseclassificationsarethesystemsmostused
by orthopedists to treatments for Legg–Calvé–Perthes disease,andalthoughtheintraandinterobserver concord-anceindicesfoundinthepresentstudywerebetterthan thoseseenintheworldwideliterature,theindicesfound here are still far from ideal. Therefore, complementary systemsforstagingthediseaseshouldbetakeninto con-sideration,inordertohavegreaterprecisionintreatingthis disease.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.Theclassic.ThefirststagesofcoxaplanabyHenning Waldenström,1938.ClinOrthopRelatRes.1984;(191):4–7. 2.JonsäterS.Coxaplana:ahistopathologicandarthrographic
study.ActaOrthopScandSuppl.1953;12:5–98.
3.CatterallA.ThenaturalhistoryofPerthes’disease.JBone JointSurgBr.1971;53(1):37–53.
4.SalterRB,ThompsonGH.Legg–Calvé–Perthesdisease.The prognosticsignificanceofthesubchondralfractureanda two-groupclassificationofthefemoralheadinvolvement.J BoneJointSurgAm.1984;66(4):479–89.
5.HerringJA,KimHT,BrowneR.Legg–Calve–Perthesdisease. PartI:classificationofradiographswithuseofthemodified lateralpillarandStulbergclassifications.JBoneJointSurg Am.2004;86(10):2103–20.
6.AltmanDG.Somecommonproblemsinmedicalresearch.In: Practicalstatisticsformedicalresearch.London:Chapman andHall;1991.p.403–9.
7.SvanholmH,StarklintH,GundersenHJ,FabriciusJ,BarleboH, OlsenS.Reproducibilityofhistomorphologicdiagnoseswith specialreferencetothekappastatistic.APMIS.
1989;97(8):689–98.
8.KamhiE,MacEwenGD.TreatmentofLegg–Calvé–Perthes disease.PrognosticvalueofCatterall’sclassification.JBone JointSurgAm.1975;57(5):651–4.
9.DickensDR,MenelausMB.Theassessmentofprognosisin Perthes’disease.JBoneJointSurgBr.1978;60(2):189–94. 10.GreenNE,BeauchampRD,GriffinPP.Epiphysealextrusionas
aprognosticindexinLegg–Calvé–Perthesdisease.JBoneJoint SurgAm.1981;63(6):900–5.
11.TerjesenT,WiigO,SvenningsenS.Thenaturalhistoryof Perthes’disease.ActaOrthop.2010;81(6):708–14. 12.IsmailAM,MacnicolMF.PrognosisinPerthes’disease:a
comparisonofradiologicalpredictors.JBoneJointSurgBr. 1998;80(2):310–4.
femoralempacientesportadoresdadoenc¸ade
Legg–Calvé–Perthesunilateralsubmetidosàosteotomiade Salter.RevBrasOrtop.1993;28(5):299–303.
14.LaredoFilhoJ.Doenc¸adeLegg–Calvé–Perthes.Classificac¸ão artrográfica.RevBrasOrtop.1992;27(1):7–15.
15.DucoulePointeH,HaddadS,SilbermanB,FilipeG,MonrocM, MontagneJP.Legg–Calvé–Perthesdisease:stagingbyMRI usinggadolinium.PediatrRadiol.1994;24(2):88–90.
16.KatzJF.FemoraltorsioninLegg–Calvé–Perthesdisease.JBone JointSurgAm.1968;50(3):473–5.
17.SalesdeGauzyJ,KerdilesN,BauninC,KanyJ,DarodesP, CahuzacJP.Imagingevaluationofsubluxationin Legg–Calvé–Perthesdisease:magneticresonanceimaging comparedwiththeplainradiograph.JPediatrOrthopB. 1997;6(4):235–8.
18.HendersonRC,RennerJB,SturdivantMC,GreeneWB. Evaluationofmagneticresonanceimagingin
Legg–Calvé–Perthesdisease:aprospective,blindedstudy.J PediatrOrthop.1990;10(3):289–97.
19.BosCF,BloemJL,BloemRM.Sequentialmagneticresonance imaginginPerthes’disease.JBoneJointSurgBr.
1991;73(2):219–24.
20.HiehleJFJr,KneelandJB,DalinkaMK.Magneticresonance imagingofthehipwithemphasisonavascularnecrosis. RheumDisClinNorthAm.1991;17(3):669–92.
21.MahadevaD,ChongM,LangtonDJ,TurnerAM.Reliabilityand reproducibilityofclassificationsystemsfor
Legg–Calvé–Perthesdisease:asystematicreviewofthe literature.ActaOrthopBelg.2010;76(1):48–57.
22.PodeszwaDA,StanitskiCL,StanitskiDF,WooR,MendelowMJ. Theeffectofpediatricorthopaedicexperienceon
interobserverandintraobserverreliabilityoftheherring lateralpillarclassificationofPerthes’disease.JPediatr Orthop.2000;20(5):562–5.
23.RajanR,ChandrasenanJ,PriceK,KonstantoulakisC,Metcalfe J,JonesS.Legg–Calvé–Perthes:interobserverand
intraobserverreliabilityofthemodifiedHerringlateralpillar classification.JPediatrOrthop.2013;33(2):120–3.