w w w . r b o . o r g . b r
Original
Article
Evaluation
of
the
reproducibility
of
the
AO/ASIF
classification
for
humeral
shaft
fractures
夽
Gustavo
Soriano
Pignataro
∗,
André
Elias
Junqueira,
Fabio
Teruo
Matsunaga,
Marcelo
Hide
Matsumoto,
João
Carlos
Belloti,
Marcel
Jun
Sugawara
Tamaoki
EscolaPaulistadeMedicina,UniversidadeFederaldeSãoPaulo,SãoPaulo,SP,Brazila
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received8May2014 Accepted25June2014 Availableonline26July2015
Keywords:
Humeralfractures/classification Humeralfractures/radiograph Humeralfractures/surgery
a
b
s
t
r
a
c
t
Objective:To evaluatethe reproducibilityoftheAO/Asifclassificationforhumeralshaft fractures.
Methods:Consecutiveradiographsofthearminbothanteroposteriorandlateralviewfrom 60patientswithhumeralshaftfractureswereanalyzed.Sixobserverswhowerefamiliar withtheAO/Asifclassification(threeshoulderandelbowsurgeryspecialistsandthree gen-eralorthopedists)wereselectedtomaketheanalysis,whichwasdoneatthreedifferent times.Thedataweresubjectedtostatisticalanalysisusingthekappacoefficient.
Results:Theintraandinterobserverconcordancewasstatisticallysignificantinallthe anal-yses.
Conclusions:Alltheevaluatorsshowedconcordancebetweenthethreeevaluationsthatwas consideredtobestatisticallysignificant.However,thehighestvalueswerefoundamongthe specialists.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Avaliac¸ão
da
reprodutibilidade
da
classificac¸ão
AO/Asif
para
fraturas
diafisárias
do
úmero
Palavras-chave:
Fraturasdoúmero/classificac¸ão Fraturasdoúmero/radiografia Fraturasdoúmero/cirurgia
r
e
s
u
m
o
Objetivo:Avaliarareprodutibilidadedaclassificac¸ãoAO/Asifparaasfraturasdiafisáriasdo úmero.
Métodos:Foramanalisadasradiografiasconsecutivasemduasincidências(anteroposterior eperfildobrac¸o)de60pacientescomfraturadoúmerodiafisário.Seisobservadores famil-iarizadoscomaclassificac¸ãoAO/Asif,trêsespecialistasemcirurgiadoombroecotovelo etrêsortopedistasgeraisforamselecionadosparaanálise,aqualsedeuemtrêstempos distintos.Osdadosforamsubmetidosàanáliseestatísticacomocoeficientekappa().
夽
WorkdevelopedintheDisciplineofHandandUpper-limbSurgery,DepartmentofOrthopedicsandTraumatology,EscolaPaulistade Medicina,UniversidadeFederaldeSãoPaulo,SãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](G.S.Pignataro).
http://dx.doi.org/10.1016/j.rboe.2015.07.003
Resultados: Aconcordânciaintraeinterobservadoresfoiestatisticamentesignificanteem todasasanálises.
Conclusões: Todososavaliadoresconcordamcomastrêsavaliac¸õesconsideradas estatisti-camentesignificantes.Porém,osmaioresvaloressãoencontradosentreosespecialistas.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Diaphyseal fractures of the humerus account for 1–3% of allfractures amongadults1,2 and 20%ofall fractureofthe humerus.3 The annual incidence is 13 to 14.5 per 100,000 individuals.4,5 Non-surgical treatment is still the standard forcasesofsolelydiaphyseal fracturingofthe humerus.6,7 Ontheother hand,surgicaltreatmentisrecommendedfor patients with neurovascular, medullary or brachial plexus lesions,those withexposed fractures,multipletrauma vic-timsandindividualswithafloatingelboworunsatisfactory reduction.8–11 Inaddition,it isindicatedincasesofcertain typesoffracturethataremoreunstable:accordingtoAO–OTA, thesearetypeAfracturesandobliquefracturesofthe proxi-malanddistalthirds.12–14
TheAOclassificationisan alphanumericsystem forall fracturesthatwascreatedin1986.15Incategorizingfractures, thissystemtakes intoconsideration theboneaffected,the regionandtypeoffractureline.
Fracturesofthelongbonesaremorecommonastraumatic injuriesthanare fracturesofthe periarticularareas.16 Sev-eralclassificationstandardshavebeendescribedforfractures. However,diaphysealfracturesarealmostexclusively identi-fiedinaccordancewiththeAO/ASIFclassificationsystem.17
Anidealclassificationsystemshouldprovideguidancefor treatment, indicate possible complications and thus make prognosticpredictionsforthefracture.Inaddition,the classifi-cationhasthefunctionsofstandardizingthecommunication languageandprovidingamechanismthatenables compar-isonsoftheresultsobtainedforagiventypeoffractureby differentcenters,inevaluationsin theliteraturethat were madeatdifferenttimes.Forthis reason,it isessentialthat thissystemshouldbevalid,reliableandreproducible.
However,therevisedversionoftheAO/ASIFclassification systemhasbeencriticizedashavinglowreproducibilityand interandintraobserverconcordance.15
In relation to fractures of the diaphyseal region of the humerus,therehavenotbeenanystudiestestingintraand interobserverconcordanceregardingthesefractures,tothe bestofourknowledge.15,18,19
Theobjective ofthe presentstudy wastoevaluateintra andinterobserverconcordanceregardingtheAO/ASIF classi-ficationfordiaphysealfracturesofthehumerus.
Method
Consecutive radiographsintwo views (anteroposteriorand lateral views of the arm) of 60 patients with diaphyseal
fractures ofthehumeruswere analyzed.These were num-beredandthepatients’namesandageswereconcealed.Cases of fractures in patients with an immature skeleton, cases ofpathologicalfractures orcasesinwhichthe patient pre-sentedprevioussurgeryinthebodysegmentconcernedwere excluded.Thequalityoftheimageswasdeterminedbytwo orthopedists whowere notinvolvedin evaluatingthe con-cordance.Theradiographswereacceptedandincludedinthe studyonlywhenbothoftheseevaluatorsconsideredthemto beacceptable.
SixobserverswhowerefamiliarwiththeAO/ASIF classifi-cationsystemwereselectedtoperformtheanalysis.Among theseobservers,threeshoulderandelbowsurgeryspecialists (SES)andthreegeneralorthopedists(GO)werechosen.Sothat the informationfrom all theobservers would be standard-ized, aself-explanatory illustrated diagram ofthe AO/ASIF classificationwashandedouttoeach oftheobservers.The names andidentifications presentonthe radiographswere coveredup and the radiographswere numbered randomly. Eachobserverclassifiedeachfractureinaccordancewiththe AO/ASIFsystematthreedifferenttimes.Atthefirstevaluation (T1),thecomputer-digitizedradiographicimageswereviewed innumericalsequence.Threeweekslater,atthesecond eval-uation(T2), thesequenceoftheradiographswasrandomly modified.Thiswasdoneagainforthethirdevaluation(T3),six weeksafterthefirstevaluation.Thisrandomizationsequence waskeptsecretbyanindividualwhowasnotinvolvedin eval-uatingtheimages.
The data were gathered together on spreadsheets and the kappa coefficient () was used for the analysis, using themethodproposed byFleiss.20 Thismadeit possiblenot onlytocalculatetheconcordancethatwouldbeexpectedby chance,butalsotheconcordancebetweenmultipleobservers (i.e. more than two) in evaluating the nominal variables. Theconcordancecoefficientprovidespairedproportionsof concordance between the observers, who may have made correct observations. The values range from −1 to +1; values between −1 and 0 indicate that the observed con-cordance isless than what would be expected bychance, 0 indicates the level of concordance achievable bychance and +1 indicates total concordance. In general terms, values lower than 0.5 are considered to be unsatisfactory, between 0.5 and 0.75 fair to satisfactory and higher than 0.75 excellent.15–18 Forthis study,wedefinedasignificance level(i.e.theextenttowhicherrorinthestatistical conclu-sionswouldbeacceptedorthestatisticalerrorthatwouldbe madeintheanalyses)of0.05(5%)andaconfidenceintervalof 95%.
1200
1000
0.800
0.600
0.400
0.200
0.000 0.610
General orthopedist 1General orthopedist 2General orthopedist 3General orthopedist Specialist
1
Specialist 2
Specialist 3
Specialist
0.445
0.726
0.596
0.725
0.839
0.763 0.782
Fig.1–Intraobserverconcordanceforthethreeevaluations.
Results
The intra and interobserver concordance values were obtained by calculating the coefficient, as proposed by Fleiss.20
Fig. 1shows the intraobserver concordance,taking into considerationthethreeevaluationtimes,bothforthegroup ofgeneralorthopedistsandforthespecialists.Allthe evalu-atorspresentedconcordancebetweenthethreeevaluations, whichwereconsideredtobestatisticallysignificant.However, highervalueswerefoundamongthespecialists,andthebest amongthemwasforspecialist2,withof0.839,whichwas consideredexcellent.
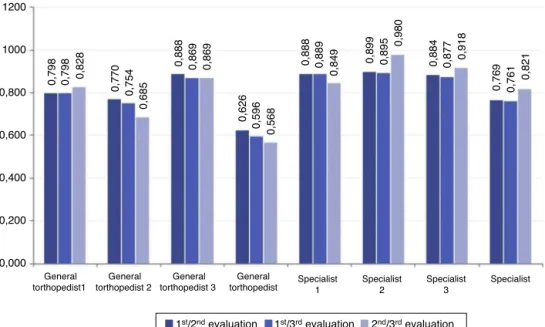
Fig.2shows theintraobserver concordanceofthe three evaluationsinpairs.
Alloftheseconcordancevalueswerestatistically signifi-cant(differentfromzero).Itwasagainseenthatthehighest concordanceoccurredinrelationtospecialist2,betweenthe secondandthirdevaluations,withavalueof0.980,whichwas classifiedasexcellent.Theintraobserverconcordanceamong thegeneralorthopedistswassatisfactory(between0.568and 0.626),whileamongtheshoulderandelbowspecialists,itwas excellent(between0.761and0.821).
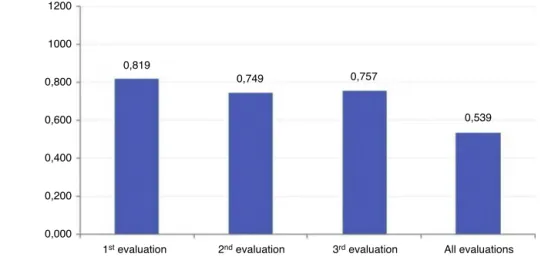
Fig.3bringstogetherthegeneralorthopedistsandthe spe-cialists,tomeasurethedegreeofconcordancebetweenthe groupsateachtime(asthreeevaluations)andingeneral(all thethreeevaluationstogether).Atalltimes,therewas statisti-callysignificantconcordance.Thehighestconcordancewasin relationtothefirstevaluation,withavalueof0.819,whichwas classifiedasexcellent.Fromgroupingthethreeevaluations, theinterobserverconcordancewassatisfactory(=0.539).
General torthopedist1
General torthopedist 2
General torthopedist 3
General torthopedist
1200
1000
0,798 0,798 0,828
0,770 0,754
0,685
0,888 0,869 0,869
0,626
0,596
0,568
0,888 0,889
0,849
0,899 0,895
0,980
0,884 0,877 0,918
0,769 0,761
0,821
0,800
0,600
0,400
0,200
0,000
Specialist 1
Specialist 2
Specialist 3
Specialist
1st/2nd evaluation 1st/3rd evaluation 2nd/3rd evaluation
1st evaluation 2nd evaluation 3rd evaluation All evaluations
1200
1000
0,749 0,819
0,757
0,539 0,800
0,600
0,400
0,200
0,000
Fig.3–Interobserverconcordanceaccordingtoevaluation.
Discussion
Several classification standards for fractures have been described.However, diaphyseal fractures are almost exclu-sivelyidentifiedinaccordancewiththeAO/ASIFclassification system.16
These classification systems are very important within orthopedicpracticebecausetheyservetodescribethefracture anddirectthetreatment,aswellasstandardizingtheinjuries scientificallyandmakingthetreatmentreproducible. There-fore,intraandinterobserverconcordancebecomeessentialfor anyclassificationsystem.
Inthe analysisontheintraobserver concordance,taking the threetimes into consideration,the mean from the AO classification was satisfactory for the generalorthopedists (=0.596), and particularly so for the specialists (=0.782). Theseresultswereprobablyduetothesimplicityand prac-ticalityofthis classification.Greater experienceamongthe orthopedistsinfluencedgreaterreliability.
Inanalyzing the intraobserver concordancebetween T1 andT2andbetweenT2andT3,itwasnotedthatinthegeneral orthopedistgrouptherewasadecreaseinthevalues,while amongthespecialiststherewasanincrease,probablydueto thespecialists’experienceofanalyzingandclassifyingthese fractures,whichtheotherorthopedistsdidnothave.In mea-suringthedegreeofconcordancebetweenthegroupsateach time,itwasseenthatgreatestconcordancewasinrelationto thefirstevaluation.Weconcludedthatsuchconditioningdid notoccurgenerally.
Throughthisstudy,itcouldbeseenthattheAO/ASIF clas-sificationfordiaphyseal fractures ofthehumerus presents goodintraandinterobserverreproducibility.Thegreaterthe familiaritywithandapplicabilityofthisclassificationwere, thegreaterthedegreeofreliabilityalsowas.
It is importantto emphasize that this study is limited toevaluatingtheconcordancebetweentheopinionsofthe observersanditwasnotpossibletomeasuretheaccuracyof thisclassification.Forthispurpose,adiagnosticstudy com-paringeachobserver withtheresultfromevaluationusing
astandarddiagnosticexamination(withhighsensitivityand specificityforprovingthediagnosis)wouldbenecessary.
Conclusion
The AO/ASIF classification system presented satisfactory intraobserver concordance amongthe generalorthopedists and excellent concordance amongthe shoulderand elbow specialists,andsatisfactoryinterobserverconcordance.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.EmmettJE,BreckLW.Areviewandanalysisof11,000
fracturesseeninaprivatepracticeoforthopaedicsurgery,
1937–1956.JBoneJointSurgAm.1958;40(5):1169–75.
2.SchemitschEH,BhandariM,TalbotM.Fracturesofthe
humeralshaft.In:Skeletaltrauma:basicscience,
managementandreconstruction.4thed.Philadelphia:
Saunders;2008.p.1593–4.
3.RoseSH,MeltonLJ3rd,MorreyBF,IlstrupDM,RiggsBL.
Epidemiologicfeaturesofhumeralfractures.ClinOrthop
RelatRes.1982;(168):24–30.
4.BrinkerMR,O’ConnorDP.Theincidenceoffracturesand
dislocationsreferredfororthopaedicservicesinacapitated
population.JBoneJointSurgAm.2004;86(2):290–7.
5.EkholmR,AdamiJ,TidemarkJ,HansonK,TörnkvistH,Ponser
S.Fracturesoftheshaftofthehumerus:anepidemiological
studyof401fractures.JBoneJointSurgBr.
2006;88(11):1469–73.
6.SarmientoA,KinmanPB,GalvinEG,SchmittRH,PhillipsJG.
Functionalbracingoffracturesoftheshaftofthehumerus.J
BoneJointSurgAm.1977;59(5):596–601.
7.BalfourGW,MarreroCE.Fracturebraceforthetreatmentof
humerusshaftfracturescausedbygunshotwounds.Orthop
8. WallnyT,WestermannK,SagebielC,ReimerM,WagnerUA.
Functionaltreatmentofhumeralshaftfractures:indications
andresults.JOrthopTrauma.1997;11(4):283–7.
9. AmilloS,BarriosRH,Martinez-PericR,LosadaJI.Surgical
treatmentoftheradialnervelesionsassociatedwith
fracturesofthehumerus.JOrthopTrauma.1993;7(3):211–5.
10.FosterRJ,SwiontkowskiMF,BachAW,SackJT.Radialnerve
palsycausedbyopenhumeralshaftfractures.JHandSurg.
1993;18(1):121–4.
11.PollockFH,DrakeD,BovillEG,DayL,TraftonPG.Treatmentof
radialneuropathyassociatedwithfracturesofthehumerus.J
BoneJointSurgAm.1981;63(2):239–43.
12.EkholmR,TidermarkJ,TörnkvistH,AdamiJ,PonzerS.
Outcomeafterclosedfunctionaltreatmentofhumeralshaft
fractures.JOrthopTrauma.2006;20(9):591–6.
13.RutgersM,RingD.Treatmentofdiaphysealfracturesofthe
humerususingafunctionalbrace.JOrthopTrauma.
2006;20(9):597–601.
14.JawaA,McCartyP,DoornbergJ,HarrisM,RingD.
Extra-articulardistalthirddiaphysealfracturesofthe
humerus.Acomparisonoffunctionalbracingandplate
fixation.JBoneJointSurgAm.2006;88(11):2343–7.
15.SwiontkowskiMF,AgelJ,McAndrewMP,BurgessAR,
MacKenzieEJ.OutcomevalidationoftheAO/OTAfracture
classificationsystem.JOrthopTrauma.2000;14(8):
534–41.
16.MullerM,NazarianS,KochP,SchatzkerJ.Thecomprehensive
classificationoffracturesoflongbones.Berlin,Germany:
Springer-Verlag;1990.
17.Fractureanddislocationcompendium.OrthopaedicTrauma
AssociationCommitteeforCodingandClassification.J
OrthopTrauma.1996;10Suppl.1:1–154.
18.JohnstoneDJ,RadfordWJ,ParnellEJ.Interobservervariation
usingtheAO/ASIFclassificationoflongbonefractures.Injury.
1993;24(3):163–5.
19.NeweyML,RickettsD,RobertsL.TheAOclassificationoflong
bonefractures:anearlystudyofitsuseinclinicalpractice.
Injury.1993;24(5):309–12.
20.FleissJL.Measuringnominalscaleagreementamongmany