SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
article
Measurement
of
quality
of
life
among
patient
undergoing
arthroplasty
of
the
thumb
to
treat
CMC
arthritis
夽
Marcio
Aurélio
Aita
∗,
Rafael
Saleme
Alves,
Luis
Felipe
Longuino,
Carlos
Henrique
Vieira
Ferreira,
Douglas
Hideki
Ikeuti,
Luciano
Muller
Reis
Rodrigues
FaculdadedeMedicinadoABC,DepartamentoClínico-CirúrgicoIV,DisciplinadeOrtopediaeTraumatologia,SantoAndré,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received3August2015 Accepted5October2015 Availableonline6June2016
Keywords: Qualityoflife Trapeziumbone Arthroplasty Thumb
a
b
s
t
r
a
c
t
Objective:Topresenttheclinicalandfunctionalresults,includingmeasurementofquality oflife,ofpatientsundergoingtrapeziometacarpalarthroplasty.
Method:Thiswasaprospectiveevaluationon45patients(53thumbs)withadiagnosisof idiopathicrhizarthrosiswhounderwentresectionarthroplastyandinterpositionofan unce-mentedAscension®implant,madeofpyrocarbon.Theclinicalandfunctionalresultswere
analyzedthroughradiography,rangeofmotion(ROM)indegrees(◦),visualanalogscale(VAS)
forpainandthedisabilityofarm,shoulderandhand(DASH)questionnaireforqualityof life.Inthegroupanalyzed,38werewomenandsevenweremen,andtheirmeanagewas 63.17years(range:50–78).Eightpatientsweretreatedbilaterally.
Results:After42.08monthsoffollow-up(range:8–73),thesubjectivepainevaluation(VAS) scorewas1.37(range:1–4).ThecompleteROMofthethumbincreasedto95.75%(range: 75–100%)inrelationtothecontralateralside.ThemeanDASHquestionnairescorewas9.98 (range:1–18).Thecomplicationrate(negativeevents)was11.32%.Fivepatientspresented dislocationofthethumbprosthesis.Allofthemwerereoperatedbymeansofdorsal cap-suloplastyusingaportionoftheretinaculumoftheextensorsasagraft,andgoodclinical evolutionwasachievedinthesecases.Onepatientpresentedfracturingofthemetacarpal andwastreatedbymeansofosteosynthesisusingKirschnerwires.
Conclusion: Thismethodiseffectivefortreatingrhizarthrosis,accordingtothe measure-mentsmadeontheclinicalandfunctionalresults,evenaftertakingthecomplicationrate intoconsideration.Moreover,itprovidesanimprovementofqualityoflifeforthesepatients. ©2016PublishedbyElsevierEditoraLtda.onbehalfofSociedadeBrasileiradeOrtopedia eTraumatologia.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedatHospitalMarioCovas,SantoAndré,SP,CentroHospitalarMunicipaldeSantoAndré,SP;andHospitaldeEnsino PadreAnchietadeSãoBernardodoCampo,SãoBernardodoCampo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](M.A.Aita).
http://dx.doi.org/10.1016/j.rboe.2016.06.003
Mensurac¸ão
da
qualidade
de
vida
dos
pacientes
submetidos
a
artroplastia
do
polegar
no
tratamento
da
rizartrose
Palavras-chave: Qualidadedevida Trapézio
Artroplastia Polegar
r
e
s
u
m
o
Objetivo: Apresentarosresultadosclínico-funcionaiseamensurac¸ãodaqualidadedevida dospacientessubmetidosàartroplastiatrapézio-metacárpica.
Método: Avaliac¸ãoprospectivade45pacientese53polegaresacometidos,com diagnós-tico derizartroseidiopáticasubmetidosàartroplastiaderessecc¸ãoeinterposic¸ão,com oimplanteAscension®,nãocimentado,depirocarbono.Foramanalisadososresultados
clínico-funcionais:análiseradiográfica,oarcodemovimento(ADM)emgraus(◦),dor(VAS:
visualanalogscore),qualidadedevida(Dash:disabilityshoulder,arm,andhandquestionnaire). Nogrupoanalisado,38sãomulheresesetesãohomenseaidademédiaéde63,17anos (50-78).Foramoperadosoitopacientescomacometimentobilateraldospolegares. Resultados: Após42,08meses(8-73)deseguimento,aavaliac¸ãosubjetivadador(VAS)foide 1,37(1-4).Oarcodomovimentocompletodopolegarteveumaumentode95,75%(75-100)do ladocontralateral.OquestionárioDashfoiemmédiade9,98(1-18).Ataxadecomplicac¸ões oueventosnegativosfoide11,32%.Observamoscincopacientescomluxac¸õesdaspróteses depolegares.Todosforamreoperadosefez-seacapsuloplastiadorsal,comousocomo enxertodeumaporc¸ãodaretináculadosextensores,obteve-seumaboaevoluc¸ãoclínica nessescasos.Umpacienteapresentoufraturadometacarpoefoitratadocomosteossíntese comfiodeKirschner.
Conclusão:Ométodoéeficaznotratamentodarizartrosedeacordocomosvaloresapurados dosresultadosclínico-funcionais,mesmoconsiderando-seastaxasdecomplicac¸ões.Além disso,proporcionaamelhoriadaqualidadedevidadessespacientes.
©2016PublicadoporElsevierEditoraLtda.emnomedeSociedadeBrasileirade OrtopediaeTraumatologia.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Rhizarthrosisisthemostcommondegenerativediseaseand theonethatmostrestrictsthethumbofmiddle-agedwomen, especiallyinthefifthandsixthdecadesoflife.Itcanalsobe observedinmenwithhistoryofrepetitivejointuseand in youngwomenwithligamentouslaxity.1
There are many recommended surgical techniques for the treatment of this disease: trapeziectomy; trapezio-metacarpal arthrodesis; ligament reconstruction; partialor totalarthroplasty;andarthroscopic resection,replacement, orinterposition.
Arthroscopic resectionand interpositionare well estab-lishedfor the treatmentof rhizarthrosisand present good results in 85% of patients. Currently, numerous partial or complete prostheses are being developed and improved to maintainaxial length ofthe first ray ofthe hand,shorten postoperativerecoverytime,2 andallowforatotalrecovery ofpinchstrength.However,resultsarenotwelldocumented.3 Thisstudyaimedtopresentclinicalandfunctionalresults and measurementin quality oflifeofpatients undergoing trapezio-metacarpalarthroplastywithuncemented pyrocar-bonAscension®implant.
Material
and
methods
Thestudyassessed65patientswhoattendedapre-operative visitinthehandsurgeryoutpatientclinicoftheuniversity
hospitalslinkedtotheinstitution.Forty-fivepatientsand53 thumbswereselected.However,inthepostoperativeperiod, patients were followed-up in asingle outpatientclinic. All patientshadthediagnosisofprimaryrhizarthrosisstagesII
andIIIaccordingtotheEatonandLittlerclassification,apud Martin-Ferreroetal.(Table1).2
Patients’ demographyconsistedof38femalesandseven males. Eight patients were surgically addressed for both hands.Thiswasaprospectivestudy,withmeanfollow-upof 42.08months(8–73).Meanagewas63.17years(50–78).
Patientswereassessedinapreoperativeevaluationandin thepostoperativeperiodthroughthefollowingmethods:
1. ApplicationoftheDASHquestionnairetoassessqualityof life;
Table1–EatonandLittlerclassificationapud Martin-Ferreroetal.2
Stage Radiologicalcriteria–EatonandLittler
I Normaljointcontours;theinterliningarticulatemaybe
widenedsecondarytolaxityorjointeffusion
II Slightnarrowingoftheinterliningarticulate;joint
debrisandosteophytes<2mm NormalSTjoint
III Markeddegenerativechangeswithnointerlining
articulate,geodes,osteophytes,andsclerosis>2mm; variabledegreesofsubluxation;normalSTjoint
IV SimilartostageIIIbutwithdegenerativechangesofthe
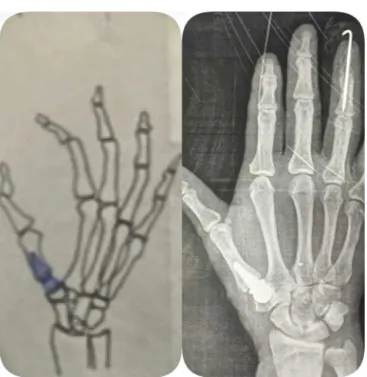
Figure1–Imagetocomparethepre-operativeplanning andradiographaspectspostoperative.
2. Measurement of the range of motion of the affected andunaffectedthumbswithaspecificgoniometer.Value expressed indicated the percentage of thumb range of motionrelativetotheunaffectedthumb;
3. Subjectiveanalysisofpainbyvisualanalogscale(VAS).
Surgicaltechniquewasthesameforallpatientsandwas appliedbythesamesurgeon(Fig.1):
1. Patientinstandard-fashionsupinepositionand prepara-tionunderlocalanesthesia;
2. Dorsalandlongitudinalapproachfortheaffectedthumb inthetrapezio-metacarpalregion;
3. Dissectionofthesensitivebranchofthedorsalnerveto thethumb;
4. Openingofthedorsalcapsuleandcarefuldissectionfor laterreinsertion;
5. Creationofthe proximalanddistalcomponentsofthe arthroplastywithresectionofmetacarpalandtrapezium osteophytes;
6. Creationofthemetacarpaltunnelwithspecificmills; 7. Placementofproofprosthesistoverifytheaccuratesize; 8. Creationofanorificeinthetrapezium,withspecificmills,
forperfectcongruencewiththedistalcomponentofthe prosthesis;
9. Placementofthepyrocarbonprosthesisonthemetacarpal in press-fit; performance of thumb bending, abduc-tion, and circumduction maneuvers to confirm stabil-ity of the prosthesis under direct visualization and fluoroscopy;
10. Soft-tissuebalancingwithdorsalcapsulesutureand ver-ificationofthestabilityofthearthroplasty;
11. Layerbylayerclosureandstitching;
12. Occlusivedressingandplacementofapreviouslymade functionalthumborthotics.
Patients in the postoperative follow-up returned every weektochangedressingsandundergocontrolX-rays.Thumb orthoticwasmaintainedforsixweeks;rehabilitationbegan inthesecondweekattheoccupationaltherapygroupofthe institution, with activities for analgesia, scarring manage-ment,andpassivemobilityofthethumb.
ThepresentedstudywasapprovedbytheResearchEthics CommitteeundertheprotocolNo.1,083,641andaninformed consentformwasprovidedforallparticipants,who volun-tarilyreadandsigned.
Results
Subjective assessmentofpain (VAS)was1.37 (1–4).Thumb rangeofmotionwas95.75%(75–100)oftheunaffectedside. MeanDASHquestionnairescorewas9.98(−18).
Complication rate was 11.32%, asthere were five dislo-cations; all thesepatients underwent reoperation with the dorsalcapsuloplastytechnique,usingadorsalwrist retinacu-lumgraft.Thesepatientspresentedagoodclinicaloutcome. Anotherpatienthad ametacarpal fractureandwastreated withinternalfixationwithKirschnerwires.Noneofthe oper-atedpatientshadfunctionalorposturalcomplaintsregarding there-operatedthumbs(Table2).
Regarding the pyrocarbon prosthesis, no patients pre-sentedimplantlooseningorfracture.
Discussion
There are numerous recommendedsurgical techniquesfor treatingrhizarthrosis.Theyallaimtoreducepainand defor-mity,increasingmobilityandthumbpinchstrength.
TheisolatedtrapeziectomydescribedbyGervisapud Ibsen-Sorensen3orassociatedwithinterpositionpresentsexcellent results,3–6buthasthedisadvantageofdecreasingthelength ofthefirstradiusandthedegreeofpinchstrength.7
Ligamentous reconstruction techniques associated with trapezoidal resection showed preservation of the radius length,andtheoretically,preservationofpinchstrength.2,4,8–11 However,theyrequireamultipleorwideaccessroute,using adjacentstructuresthatrequirealengthyscarringand reha-bilitationtime.
Searchingformorephysiologicalandlessinvasive proce-dures, aimingtopreservethe axial axisofmotionand the degreeofclampforce,aswellastoreducetheearlier post-operative recovery time, arthroscopy techniques12 (with or withoutinterpositionofstructures)andseveralpartialortotal replacementprosthesishavebeendeveloped.
In the present study, the partial uncemented pyrocar-bonAscension®prosthesis13–15wasimplantedwithadorsal accessroute,showinggoodfunctionalresultsandimproved qualityoflifeinpatientspostprocedure,despitethe compli-cationrateof11.32%.
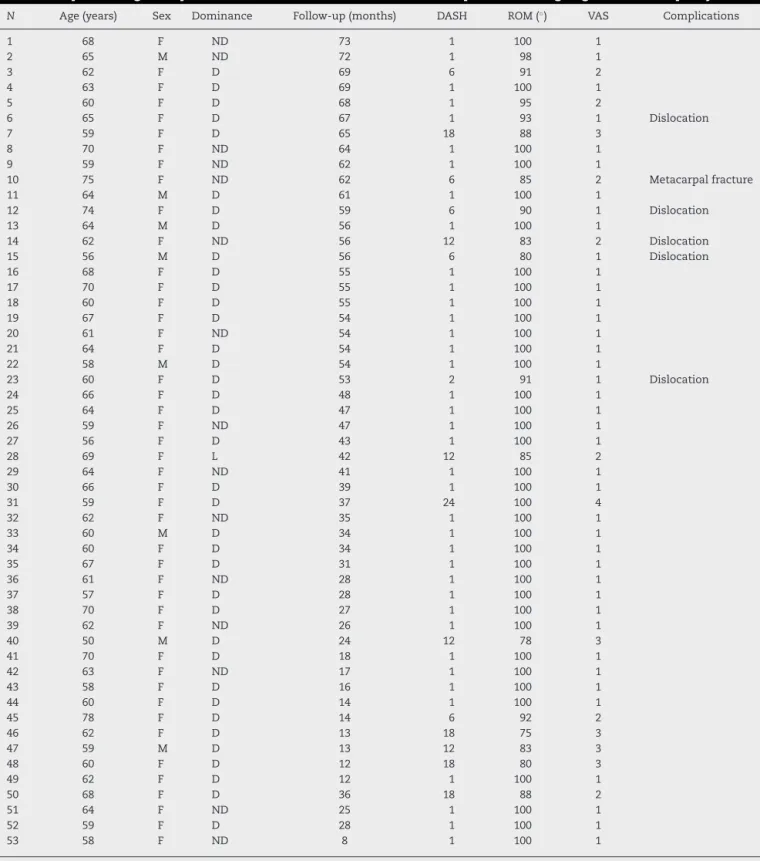
Table2–Epidemiologicalaspectsandclinicalandfunctionaloutcomesofpatientsundergoingthumbarthroplasty.
N Age(years) Sex Dominance Follow-up(months) DASH ROM(◦) VAS Complications
1 68 F ND 73 1 100 1
2 65 M ND 72 1 98 1
3 62 F D 69 6 91 2
4 63 F D 69 1 100 1
5 60 F D 68 1 95 2
6 65 F D 67 1 93 1 Dislocation
7 59 F D 65 18 88 3
8 70 F ND 64 1 100 1
9 59 F ND 62 1 100 1
10 75 F ND 62 6 85 2 Metacarpalfracture
11 64 M D 61 1 100 1
12 74 F D 59 6 90 1 Dislocation
13 64 M D 56 1 100 1
14 62 F ND 56 12 83 2 Dislocation
15 56 M D 56 6 80 1 Dislocation
16 68 F D 55 1 100 1
17 70 F D 55 1 100 1
18 60 F D 55 1 100 1
19 67 F D 54 1 100 1
20 61 F ND 54 1 100 1
21 64 F D 54 1 100 1
22 58 M D 54 1 100 1
23 60 F D 53 2 91 1 Dislocation
24 66 F D 48 1 100 1
25 64 F D 47 1 100 1
26 59 F ND 47 1 100 1
27 56 F D 43 1 100 1
28 69 F L 42 12 85 2
29 64 F ND 41 1 100 1
30 66 F D 39 1 100 1
31 59 F D 37 24 100 4
32 62 F ND 35 1 100 1
33 60 M D 34 1 100 1
34 60 F D 34 1 100 1
35 67 F D 31 1 100 1
36 61 F ND 28 1 100 1
37 57 F D 28 1 100 1
38 70 F D 27 1 100 1
39 62 F ND 26 1 100 1
40 50 M D 24 12 78 3
41 70 F D 18 1 100 1
42 63 F ND 17 1 100 1
43 58 F D 16 1 100 1
44 60 F D 14 1 100 1
45 78 F D 14 6 92 2
46 62 F D 13 18 75 3
47 59 M D 13 12 83 3
48 60 F D 12 18 80 3
49 62 F D 12 1 100 1
50 68 F D 36 18 88 2
51 64 F ND 25 1 100 1
52 59 F D 28 1 100 1
53 58 F ND 8 1 100 1
Source:SAME.
DASH,disabilitythearm,shoulder,andhand;ROM,rangeofmotion;VAS,visualanalogscore;kgf,kilogram-force;ND,non-dominant;D, dominant.
ComparingthepresentstudywiththatbyIbsen-Sorensen,3 which used a cemented metal-polyethylene total prosthe-sis, similar results were observed for pain improvement, complicationrate,andrangeofmotiongain.Inthepresent
study,therewerefivedislocationsin53operatedthumbsvs. fivedislocationsinthe54casesoperatedbyIbsen-Sorensen.
reconstruction,4,9–11,16withpatientsatisfactionratescloseto 90%.
Some comparative studies have shown the advantages of arthroplasty with interposition of pyrocarbon implants whencomparedtoligamentreconstructionwithoutimplant interposition.19
Althoughthe present study had a shortfollow-up time (42.08 months), the final results do not change much six monthsaftersurgery.
Prosthesis stability is due to several factors, including implant-trapezoidcongruenceand,moreover,healingofthe soft tissue envelope around the trapeziometacarpal joint, especiallythedorsalcapsule.
Pyrocarbon osseointegration was observed in all cases in the present study, without implant loosening or fracture, which is in agreement with the study by Beckenbaugh–Klawitter.14
The pyrocarbon prosthesis used in this technique has advantages over other implants. It preserves bone mass due to a basic minimal resection of the first metacarpal; trapezium resectionisnot necessary, andtherefore thumb height is maintained. As these are uncemented pros-theses that fixate to the metacarpal through press fit, and given that pyrocarbon has the same hardness as the bone, these prostheses allow for maximum grip with the metacarpal and do not generate debris or stress shielding. Furthermore, pyrocarbon has excellent biocompatibility.20
Complicationrateinthepresent studywas 11.32%.Five patientspresentedsingledislocations,whichwereresolved withdorsalcapsuloplasty.
ThestudybySzalayetal.,16whousedpyrocarbon interpo-sitionprosthesis,presentedahigherrateofcomplicationsand worsefunctionaloutcomeswhencomparedwiththepresent study.
Thepresentauthorsbelievethatreplacementarthroplasty of the base of the first metacarpal bone associated with interposition arthroplasty of the trapezium, using a single component,preservesthumblengthandrangeofmotion,as wellasqualityoflifeforthesepatients.Themobilityofthis joint,whichwaspreviouslysellar,becomessphericalwiththe useofthisprosthesis;thisdemonstratesthatthisprocedure iseffectiveintreatingrhizarthrosis.
Theauthorsnotethatpainimprovementisonlyobserved sixthmonthsaftertheprocedure;thereasonforthisisstill unknown, as pyrocarbon is a recent material in orthope-dics.
Thepresent study limited itself to presentingthe clini-calandfunctionalresultsandassessingthequalityoflifeof patientsafterthedescribedprocedure.
Conclusion
Thumb arthroplasty is effective in treating rhizarthrosis, according toclinical and functional outcomes and compli-cations rate, and provides better quality of life for these patients.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.Allmaterialwas provided by the company that owns the material, which allowed thestudy tobe conductedatno extra costto the BrazilianUnifiedHealthcareSystem.
r
e
f
e
r
e
n
c
e
s
1.MartouG,VeltriK,ThomaA.Surgicaltreatmentof osteoarthritisofthecar-pometacarpaljointofthethumb:a systematicreview.PlastReconstrSurg.2004;114(2):421–32.
2.Martin-FerreroMH,VegaC,LomoJA.Long-termresults(more than10years)followupoftotaljointarthroplastyinthe treatmentofthumbcarpometacarpaljointosteoarthritis.J HandSurgEur.2011;361Suppl.:S46–7.
3.Ibsen-SorensenA.Theelektraprosthesisfortotal replacementofthefirstcmc-joint.Prospectivestudywith follow-upofonetosixyears.JHandSurgEur.2011;361 Suppl.:S50.
4.BurtonRI,PellegriniVDJr.Surgicalmanagementofbasaljoint arthritisofthethumb.PartII.Ligamentreconstructionwith tendoninterpositionarthroplasty.JHandSurgAm. 1986;11(3):324–32.
5.MurleyAH.Excisionofthetrapeziuminosteoarthritisofthe firstcarpometacarpaljoint.JBoneJointSurgAm.
1960;42:502–7.
6.DellPC,MunizRB.Interpositionarthroplastyofthe
trapeziometacarpaljointforosteoarthritis.ClinOrthopRelat Res.1987;(220):27–34.
7.EatonRG,LaneLB,LittlerJW,KeyserJJ.Ligament
reconstructionforthepainfulthumbcarpometacarpaljoint: along-termassessment.JHandSurgAm.1984;9(5): 692–9.
8.VermeulenGM,BrinkSM,SluiterJBA,EliasMGS,HoviusRES, MoojenTM.Ligamentreconstructionarthroplastyforprimary thumbcarpometacarpalosteoarthritis(WeilbyTechnique): prospectivecohortstudy.JHandSurgAm.2009;34: 1393–401.
9.DavisTR,BradyO,DiasJJ.Excisionofthetrapeziumfor osteoarthritisofthetrapeziometacarpaljoint:astudyofthe benefitofligamentreconstructionortendoninterposition.J HandSurgAm.2004;29(6):1069–77.
10.HartiganJB,SternPJ,KiefhaberTR.Thumbcarpometacarpal osteoarthritis:arthrodesiscomparedwithligament reconstructionandtendoninterposition.JBoneJointSurg Am.2001;83(10):1470–8.
11.TomainoMM.Ligamentreconstructiontendoninterposition arthroplastyforbasaljointarthritis.Rationale,current technique,andclinicaloutcome.HandClin.2001;17(2):207–21.
12.DaRinF,MathoulinC.Arthroscopictreatmentof osteoarthritisofscaphotrapezotrapezoidjoint.ChirMain. 2006;25Suppl1:S254–8.
13.ThompsonJS.Suspensionplasty.JOrthopSurgTech. 1989;4:1–13.
14.BeckenbaughRD,KlawitterJ,CookS.Osseointegrationand mechanicalstabilityofpyrocarbonandtitaniumhand implantsinaload-bearinginvivomodelforsmalljoint arthroplasty.JHandSurgAm.2006;31(7):1240–1.
16.SzalayG,SchleicherI,AltV,PavlidisT,SchnettlerR.Operative treatmentofrhizarthritis:comparisonofligament
reconstructionaccordingtoEppingwithtrapezectomyand interpositionofpyrocarbonspacersasreplacementofthe trapezium.Orthopade.2011;40(3):237–46.
17.GervisWH.Excisionofthetrapeziuminosteoarthritisofthe trapezio-metacarpaljoint.JBoneJointSurgBr.
1949;31(4):537–9.
18.IyerKM.Theresultsofexcisionofthetrapezium.Hand. 1981;13(3):246–50.
19.Colegate-StoneTJ,GargS,SubramanianA,ManiGV.Outcome analysisoftrapezectomywithandwithoutpyrocarbon interpositiontotreatprimaryarthrosisofthe
trapeziometacarpaljoint.HandSurg.2011;16(1): 49–54.