REVISTA
BRASILEIRA
DE
REUMATOLOGIA
www . r e u m a t o l o g i a . c o m . b r
Original
article
Hashimoto
thyroiditis
may
be
associated
with
a
subset
of
patients
with
systemic
sclerosis
with
pulmonary
hypertension
Ciliana
Cardoso
B.
Costa
a,
Morgana
Medeiros
a,
Karen
Watanabe
b,
Patricia
Martin
a,
Thelma
L.
Skare
a,∗aHospitalUniversitárioEvangélicodeCuritiba,Curitiba,PR,Brazil bFaculdadeEvangélicadoParaná,Curitiba,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received20December2013 Accepted24April2014 Availableonline20August2014
Keywords: Systemicsclerosis Scleroderma
Hashimotothyroiditis Pulmonaryhypertension
a
b
s
t
r
a
c
t
Introduction:Recentstudiesshowanassociationbetweenautoimmunethyroiditisand sys-temicsclerosis(SSc)andsuggestthatthisconditionmayinterferewiththeESphenotype. Howeverthesestudiesevaluatetheautoimmunethyroiditisasawholeandnoneofthem specificallyaddressesHashimoto’sthyroiditis(HT)inSSc.
Objective:ToinvestigatethepresenceofHTinSScpatientsanditspossibleassociationwith diseasemanifestations.
Methods:Clinicalmanifestationsofhypothyroidism,TSHandanti-thyroidautoantibodies (anti-TPO.antiTBGandTRAb)werestudiedin56patientswithSSc.SScpatientswithHT werecomparedwithSScpatientswithoutthyroiditis.
Results:HTwasobservedin 19.64% ofpatientswith SSc. Noassociationwasobserved betweenHTandthedifferentformsofdiseaseorprofileofautoantibodies.Likewise,there wasnodifferencebetweenthemeanmodifiedRodnanscoreandpresenceofRaynaud’s phenomenon,scars,digitalnecrosis,myositis,arthritis,siccasymptoms,esophageal dys-motilityandsclerodermarenalcrisiswhenthegroupswerecompared.Ontheotherhand, patientswithHThadhigherfrequencyofpulmonaryhypertensioninrelationtopatients withoutHT(66.6%vs22.5%,p=0.016).
Conclusions:InthestudiedsamplepatientswithESandHThadhigherprevalenceof pul-monaryhypertension.Long-termfollow-upstudieswithalargernumberofTHandSSc patientsareneededtoconfirmthesedata.
©2014ElsevierEditoraLtda.Allrightsreserved.
DOIoforiginalarticle:http://dx.doi.org/10.1016/j.rbr.2014.04.001.
∗ Correspondingauthor.
E-mail:[email protected](T.L.Skare). http://dx.doi.org/10.1016/j.rbre.2014.04.001
Tireoidite
de
Hashimoto
pode
estar
associada
a
um
subgrupo
de
pacientes
de
esclerose
sistêmica
com
hipertensão
pulmonar
Palavras-chave: Esclerosesistêmica Esclerodermia
TireoiditedeHashimoto Hipertensãopulmonar
r
e
s
u
m
o
Introduc¸ão: Estudosrecentesmostramassociac¸ãoentretireoiditesautoimuneseesclerose sistêmica(ES),esugeremqueessacondic¸ãopodeinterferirnofenótipodaES.Entretanto, essesestudosavaliamastireoiditesautoimunescomoumtodoenenhumdelesaborda especificamenteatireoiditedeHashimoto(TH)naES.
Objetivo: Investigarapresenc¸adeTHempacientescomESesuapossívelassociac¸ãocom asmanifestac¸õesdadoenc¸a.
Casuísticaemétodos: Manifestac¸õesclínicasdehipotireoidismo,TSH,T4livreeanticorpos antitireoidanos(anti-TPO,antiTBGeTRAb)forampesquisadosem56pacientescomES. PacientescomESeTHforamcomparadoscompacientescomESsemtireoidite.
Resultados:THfoiobservadaem19,64%dospacientescomES.Nãofoiencontradaassociac¸ão entreaTHeasdiferentesformasdedoenc¸aoucomoperfildeautoanticorpos.Damesma forma, nãohouve diferenc¸aentrea média doescore de Rodnanmodificado e entrea presenc¸adefenômenodeRaynaud,cicatrizesestelares,necrosedigital,miosite,artrite, sintomassicca,dismotilidadeesofágicaoucriserenalesclerodérmicaquandoosgrupos foramcomparados.Poroutrolado,pacientescomTHapresentarammaiorfrequênciade hipertensãopulmonarquandocomparadosapacientessemTH(66,6%vs22,5%;p=0,016). Conclusões: NaamostradeESestudada,aTHestáassociadaaumamaiorprevalênciade hipertensãopulmonar.Estudosdeseguimentoalongoprazo,englobandoumnúmeromaior depacientescomESeTH,sãonecessáriosparaconfirmaressesdados.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
The association among autoimmune diseases is common,
regardless if they are organ-specific or systemic.1 Thus, it
is necessary that the physician attending these patients be aware of possible associations, not only for an early diagnosisofsuchentities,butalsotounderstandmore com-pletelythe clinical manifestationsthat thesepatients may have.
Althoughthereisnoclearexplanationfortheassociation betweenautoimmunediseases,itisassumedthatthereisa geneticpredispositiontoacommonimmunedefectinmanyof them.1Amongotherpossibilities,theexposuretosome
even-tualinfectiousorenvironmentalagentthatactsasatriggering factorofseveraldiseasesmaybeimplicated.1
Hashimoto’sthyroiditis(HT)isthemostcommon autoim-munediseaseofthethyroid,beingconsideredasaprototype oforgan-specific autoimmune diseases.2 HT presents with
varyingdegreesofglandulardysfunction, presenceof anti-thyroidantibodiesandgoiteroratrophyofthegland,anda diffuselymphocytictissueinfiltrate.2
Ontheotherhand,SScisasystemicautoimmunedisease characterizedbyvasculopathy, excessive deposition of col-lagenintissuesandpresenceofautoantibodies.3 Theexact
role ofautoantibodiesinSSc isnotwell defined,4 but it is
known that they can influence the phenotype presented.4
Indeed,fluctuations intopoisomeraseItitles correlatewith skinthickening,assessedbythemodifiedRodnanscore,and with disease activity, measured by clinical and laboratory parameters.5 Interestingly,a subsetof patientswho
devel-opednegativityforthisantibodyshowedlessskinthickening,
lesslunginvolvementandbettersurvival,whencomparedto thosepersistentlypositivepatients.6
SScpatientsmayhaveantibodiesagainstthyroidantigens, withorwithoutglanddysfunction.7 Arecentmeta-analysis
showedthatthyroidautoimmunediseasewasthemore com-mon organ-specific autoimmunity disease inpatients with SSc, with anestimated prevalenceof 10.4%.8 The
associa-tionofSScwithanti-thyroidperoxidaseantibodiesislinked tothe presenceofHLA-DR15.7 TheconnectionofSSc with
otherautoimmunediseasesalsoseemstointerferewiththeir phenotype,4,8 affectingthesepatientswithamilderformof
thedisease.However,nostudyhasspecificallyaddressedthe associationofSScwithHT.Thus,theaimofthisstudywasto investigatethepresenceofHTinSScpatientsandits possi-bleassociationwithimmunologicalandclinicalprofilesofthe disease.
Patients
and
methods
A cross-sectional study evaluating 56 consecutive patients followed-up atanoutpatientclinicofsystemicsclerosis in asingletertiarycarehospitalwasconducted.Datawere col-lectedfromJune2012toJune2013.Allpatientsrecruitedmet theclassificationcriteriaforSScfromACR/EULAR2013.9
The following manifestations of SSc were addressed:
Raynaud’sphenomenon, stellarscars, digital necrosis,skin thickeningaccordingtothemodifiedRodnanscore,10
myositiswasestablishedbythepresenceofproximal mus-cleweaknessassociatedwithatleast oneofthe following: increasedCPK,EMGwithmyopathicpattern,orbiopsywith myositis.11Distaldysmotilityoraperistalsiswasconsidered
presentwhendocumented bymanometryor seriography.11
CardiacinvolvementwasconsideredascausedbySScwhen presented in the form of pericarditis and/or heart failure, orasanarrhythmianotattributedtoothercauses.11
Inter-stitial lung disease was diagnosed when the forced vital capacitywas<70%ofthepredicted,orground-glass/fibrosis opacitieswere observedinthoraxhigh-resolution tomogra-physcans.12,13Thediagnosisofpulmonaryhypertensionwas
establishedwhenthesystolicpulmonaryarterypressurewas >40mmHgobservedinanechocardiogram,orthepulmonary arterymeanpressurewas>25mmHgwithpulmonaryartery occlusionpressure<15mmHg.4,11
WeevaluatedalsothepresenceofANA,anti-Scl70, anti-centromere,anti-Roandanti-La.Clinicalandlaboratorydata wereconsideredcumulativelypositive.Diseaseseveritywas assessedbyMedsgerindex.14
The diagnosis of HT was performed in patients who
hadhypothyroidism orgoiter associatedwiththe presence of positive antibodies.4 To evaluate thyroid function, TSH
and free T4 were measured. The dosed antibodies were
anti-peroxidase(anti-TPO),anti-thyroglobulin(anti-TBG)and
anti-TSH receptor (TRAb). TSH and free T4 levels were
obtainedbychemiluminescence,andvaluesof0.5-3.6IU/mL and0.70-1.80ng/dLwereconsiderednormalforTSHandfree T4, respectively. Theanti-thyroid autoantibodieswere also investigatedbychemiluminescence;andvalues<35IU/mLfor anti-TBG;40IU/mLforanti-TPO;and1.35IU/LforTRAbwere consideredasnormalresults.
Theresearch protocol was approvedby the localethics committeeandall participantsgavewritten informed con-sent.
Thedatawerepresentedasmedianandinterquartilerange (IQR)ifnotnormal,andasmeanwithstandarddeviation(SD) ifnormal,accordingtotheKolmogorov-Smirnovtest.When somevariableshowedindicationsofnormaldistribution,we usedtheStudent’sttestforcomparisonbetweenthemeans oftwocontinuousvariables;whennormalitywasrejected,we usedtheMannWhitneytestfortwocontinuousvariables.
Categoricalvariableswerecomparedusingthechi-squared test or Fisher’s exact test, when appropriate. A P-value <0.05 was considered statistically significant. All calcula-tions weremade withtheaid ofMedCalc softwareversion 12.0.
Results
Descriptionofthesample
Fifty-sixpatientswere studied: 52women(92.8%)and four men(7.1%), aged19-81years(median=56;IQRof39-61).In thispopulation,33%wereAfricandescents(blackandbrown), 66%wereCaucasians,and1%hadIndianancestry.Regarding theformofscleroderma,19/56(33.9%)patientshadthediffuse type,and37/56(66.1%)hadthelimitedtype.Approximately 39.6%weresmokers.
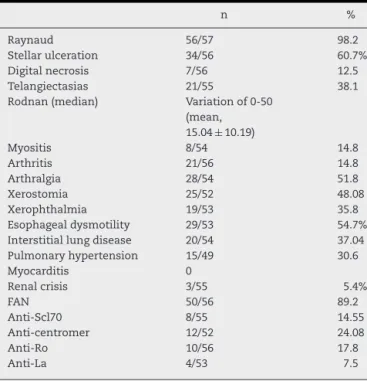
Table1–Clinicalandserologicalprofileof53patients withscleroderma.
n %
Raynaud 56/57 98.2
Stellarulceration 34/56 60.7%
Digitalnecrosis 7/56 12.5
Telangiectasias 21/55 38.1
Rodnan(median) Variationof0-50
(mean, 15.04±10.19)
Myositis 8/54 14.8
Arthritis 21/56 14.8
Arthralgia 28/54 51.8
Xerostomia 25/52 48.08
Xerophthalmia 19/53 35.8
Esophagealdysmotility 29/53 54.7%
Interstitiallungdisease 20/54 37.04
Pulmonaryhypertension 15/49 30.6
Myocarditis 0
Renalcrisis 3/55 5.4%
FAN 50/56 89.2
Anti-Scl70 8/55 14.55
Anti-centromer 12/52 24.08
Anti-Ro 10/56 17.8
Anti-La 4/53 7.5
Theautoantibodyandclinicalprofilesofourpopulationare showninTable1.
TheevaluationoftheMedsgerseverityindexwasavailable for40patientsandrangedfrom1to15,withamedianof5.0 (IQR,4.0to7.75).
Anti-TPOantibodywaspresentin32.1%;anti-TBGin18.8%; and anti-TRAbin11.4%.ThediagnosisofHTwasobserved in19.64%ofpatientswithSScandallofthemhad hypothy-roidismatdiagnosis.
ComparisonofSScpopulationswithandwithoutHT
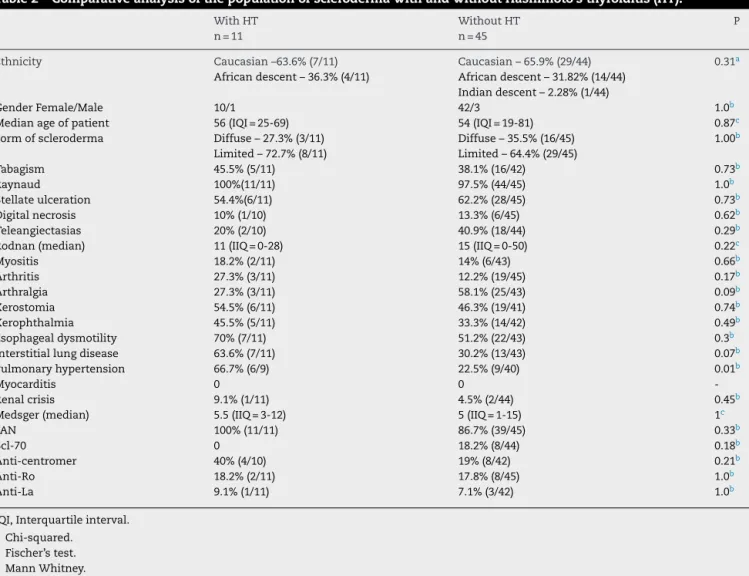
No associationbetween HT and the differentforms ofthe diseaseorautoantibodyprofilewasobserved.Likewise,there wasnodifferencebetweenthemeanmodifiedRodnanscore and betweenthepresenceofRaynaud’sphenomenon, stel-larscars,digitalnecrosis,myositis,arthritis,siccasymptoms, esophagealdysmotilityandsclerodermarenalcrisiswhenthe groupswerecompared,ascanbeseeninTable2.Ontheother hand,patientswithHTexhibitedahigherfrequencyof pul-monaryhypertensionwhencomparedtopatientswithoutHT (66.6%vs.22.5;P=0.016).
Discussion
There are several mechanisms associated with the occur-rence ofhypothyroidisminpatientswithSSc.Thesclerosis ofthe glandular tissueisoneofthem;15 the simultaneous
occurrence of autoimmune thyroid diseases is another.1
As previously mentioned, the association among several
autoimmunediseasesiscommonlyobserved,suggestingthe presenceofcommonpathophysiologicalmechanismsinthe scenario of these conditions.1 Although the true events
Table2–ComparativeanalysisofthepopulationofsclerodermawithandwithoutHashimoto’sthyroiditis(HT).
WithHT n=11
WithoutHT n=45
P
Ethnicity Caucasian–63.6%(7/11) Caucasian–65.9%(29/44) 0.31a
Africandescent–36.3%(4/11) Africandescent–31.82%(14/44) Indiandescent–2.28%(1/44)
GenderFemale/Male 10/1 42/3 1.0b
Medianageofpatient 56(IQI=25-69) 54(IQI=19-81) 0.87c
Formofscleroderma Diffuse–27.3%(3/11) Diffuse–35.5%(16/45) 1.00b
Limited–72.7%(8/11) Limited–64.4%(29/45)
Tabagism 45.5%(5/11) 38.1%(16/42) 0.73b
Raynaud 100%(11/11) 97.5%(44/45) 1.0b
Stellateulceration 54.4%(6/11) 62.2%(28/45) 0.73b
Digitalnecrosis 10%(1/10) 13.3%(6/45) 0.62b
Teleangiectasias 20%(2/10) 40.9%(18/44) 0.29b
Rodnan(median) 11(IIQ=0-28) 15(IIQ=0-50) 0.22c
Myositis 18.2%(2/11) 14%(6/43) 0.66b
Arthritis 27.3%(3/11) 12.2%(19/45) 0.17b
Arthralgia 27.3%(3/11) 58.1%(25/43) 0.09b
Xerostomia 54.5%(6/11) 46.3%(19/41) 0.74b
Xerophthalmia 45.5%(5/11) 33.3%(14/42) 0.49b
Esophagealdysmotility 70%(7/11) 51.2%(22/43) 0.3b
Interstitiallungdisease 63.6%(7/11) 30.2%(13/43) 0.07b
Pulmonaryhypertension 66.7%(6/9) 22.5%(9/40) 0.01b
Myocarditis 0 0
-Renalcrisis 9.1%(1/11) 4.5%(2/44) 0.45b
Medsger(median) 5.5(IIQ=3-12) 5(IIQ=1-15) 1c
FAN 100%(11/11) 86.7%(39/45) 0.33b
Scl-70 0 18.2%(8/44) 0.18b
Anti-centromer 40%(4/10) 19%(8/42) 0.21b
Anti-Ro 18.2%(2/11) 17.8%(8/45) 1.0b
Anti-La 9.1%(1/11) 7.1%(3/42) 1.0b
IQI,Interquartileinterval. a Chi-squared.
b Fischer’stest. c MannWhitney.
background on which environmental factors act.1 Several
studieshave shownthat smoking,deficiencyofvitamin D, diet,ultravioletlight,drugsandviralinfectionscanfunctionas environmentaltriggersforautoimmunityingenetically pre-disposedsubjects.1
Itwas observedin the present study a high prevalence ofHT inSSc patients(20%), which confirmsthe finding of thecoexistenceofautoimmunediseases.Aknowledgeofthis associationisoffundamentalimportancetotheclinicianthat, intreating anautoimmune disease,remains alert toother ones.Moreover,thesymptomspresentedbyapatientwithHT andhypothyroidismandSSccanbeconfusedwitheachother, especiallyinthecaseofthosemostnonspecificsymptoms, suchastiredness,fatigue,muscularweakness,anorexiaand arthralgia.16Thesemustbeproperlyattributedtothecausal
element,inordertotreatthepatientadequately.
Avouacetal.,4studyingpatientsofEuropeanorigin,found
thatSScpatientswithother concomitantautoimmune dis-ease appeared to have a milder SSc, associated with the limitedformofpresentation.Inthepresentanalysis,these findings could not be confirmed. However, it is important to note that the authors above included in his work sev-eralorgan-specific autoimmunediseases, suchasSjögren’s
syndrome, myositis, systemic lupus erythematosus, and
thyroiditis,andnotonlyHTasinourstudy,whichmayexplain thedifferenceinfindings.
Still in the current sample, HT patients had a higher prevalence of pulmonary arterial hypertension (PAH). The associationbetweenhypothyroidismandprimarypulmonary hypertensionhadbeennotedpreviously.17–19 Opraviletal.20
alsoreportedanincreaseintheprevalenceofhypothyroidism inpatientswithHIVandPAH,confirmingthepossible associ-ationbetweenthesetwoentitiesinanothercontext.
Thyroid dysfunction has been associated with
alter-ationsinvasoreactivity,aphenomenonthatprecedesPAH.21
VasospasmcausingRaynaud’sphenomenonhasbeenfound
in patients with isolated hypothyroidism and responds to
treatment with levothyroxine, which again suggests an
intriguing relationship betweenthis hormone and the sta-bilization of vascular reactivity.22 Furthermore, in animal
models,hypothyroidismhasbeenshowntocauseincreasesin thelevelsofendothelin-1,apotentvasoconstrictorthat con-tributestothepathogenesisofPAH,23,24andtothepulmonary
hypertensionofSSc.25Ifthisassociationwillprovetrue,the
the thyroid dysfunction, respond to the treatment of the endocrinedisease.26
Inthisanalysis,weobservedatrendofpositive associa-tionofHTwithinterstitiallungdiseaseandatrendtowardsa negativeassociationwitharthralgias.Interestingly,the liter-aturedescribescasesofassociationofpatientswithHTand interstitiallungdisease,regardlessoftheexistenceofSSc.27,28
Therearelimitationstothisstudy:oneofthemisthesmall numberofSScpatientsstudied.Thesecondisthefactthat notallpatientshad catheterizationintheright sideofthe heart,andsotheirpulmonaryarterypressuresisestimated by echocardiography. However, from a clinical standpoint, theassociationfoundisveryimportantanddeservesfurther researchwithlargernumbersofpatients.
Inconclusion,itcanbesaidthatinthepresentstudywe foundaprevalenceofHTinabout20%oftheSScpopulation. Largerstudiesareneededtoclarifythedefinitiveroleofthis associationwithPAH.
CApprovalofethics–Opinion398119–ResearchEthics Committee,SociedadeEvangélicaBeneficentedeCuritiba.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. NancyAL,YehudaS.Predictionandpreventionof
autoimmunedisorders.ArchDermatolRes.2009;301:57–64. 2. DayanCM,DanielsGH.Chronicautoimmunethyroiditis.N
EnglJMed.1996;335:99–107.
3. AllanoreY,AvouacJ,KahanA.Systemicsclerosis:anupdate in2008.JointBoneSpine.2008;75:650–5.
4. AvouacJ,AiròP,DieudeP,CaramaschiP,TievK,DiotE,etal. Associatedautoimmunediseasesinsystemicsclerosisdefine asubsetofpatientswithmilderdisease:resultsfrom2large cohortsofEuropeanCaucasianpatients.JRheumatol. 2010;37:608–14.
5. HuPQ,FertigN,MedsgerJrTA,WrightTM.Correlationof serumanti-DNAtopoisomeraseIantibodylevelswithdisease severityandactivityinsystemicsclerosis.ArthritisRheum. 2003;48:1363–73.
6. KuwanaM,KaburakiJ,MimoriT,KawakamiY,TojoT. Longitudinalanalysisofautoantibodyresponseto topoisomeraseIinsystemicsclerosis.ArthritisRheum. 2000;43:1074–84.
7. MolteniM,BariliM,EiseraN,ScrofaniS,MascagniB,ZulianC, etal.Anti-thyroidantibodiesinItaliansclerodermapatients: associationofanti-thyroidperoxidase(anti-TPO)antibodies withHLA-DR15.ClinExpRheumatol.1997;15:529–34. 8. ElhaiM,AvouacJ,KahanA,AllanoreY.Systemicsclerosisat
thecrossroadofpolyautoimmunity.AutoimmunRev. 2013;12:1052–7.
9. vandenHoogenF,KhannaD,FransenJ,JohnsonSR,BaronM, TyndallA,etal.2013classificationcriteriaforsystemic
sclerosis:anAmericanCollegeofRheumatology/European leagueagainstrheumatismcollaborativeinitiative.Ann RheumDis.2013;72:1747–55.
10.ClementsPJ,LachenbruchP.Siebold.InterandIntraobsever variabilityoftotalskinthicknessscore(modifiedRodnanTSS) insystemicsclerosis.JRheumatol.1995;22:1281–5.
11.PoormoghimH,LucasM,FertigN,MedsgerJrTA.Systemic sclerosissinescleroderma:demographic,clinical,and serologicfeaturesandsurvivalinforty-eightpatients. ArthritisRheum.2000;43:444–51.
12.BehrJ,FurstDE.Pulmonaryfunctiontests.Rheumatology. 2008;47:65–7.
13.WellsAU.High-resolutioncomputedtomographyand sclerodermalungdisease.Rheumatology.2008;47:59–61. 14.MedsgerJrTA,SilmanAJ,SteenVD,BlackCM,AkessonA,
BaconPA,etal.Adiseaseseverityscaleforsystemicsclerosis: developmentandtesting.JRheumatol.1999;26:2159–67. 15.RobazziTCMV,AdanLF.Autoimmunethyroiddiseaseon
patientswithrheumaticdiseases.RevBrasReumatol. 2012;52:417–30.
16.PearceEN,FarwellAP,BravemanM.Thyroiditis.NEngJMed. 2003;348:2647–55.
17.SweeneyL,VoelkerNF.Estrogenexposure,obesityand thyroiddiseaseinseverepulmonaryhypertension.EurJMed Res.2009;14:433–42.
18.ChuJW,KaoPN,FaulJL,DoyleRL.Highprevalenceof autoimmunethyroiddiseaseinpulmonaryarterial hypertensiom.Chest.2002;122:1668–73.
19.CurnockA,RaedM,HigginsB,HusseinS,ArroligaAC.High prevalenceofhypothyroidisminpatientswithprimary hypertension.AmJMedSci.1999;318:289–92.
20.OpravilM,PechereM,SpeichR,Joller-JemelkaH,JenniR,Russi EW,etal.HIV-associatedprimarypulmonaryhypertension:a casecontrolstudy.AmJRespirCritCareMed.1997;155:990–5. 21.BadeschDB,WynneKM,BonvalletS,VoelkerNF,RidgwayC,
GrovesBM.Hypothyroidismandprimarypulmonary hypertension:anautoimmunepathogeniclink?AnnIntern Med.1993;119:44–6.
22.LateiwishAM,FeherJ,BaraczkaK,RáczK,KissR,GlázE. RemissionofRaynaud’sphenomenonafterL-thyroxine therapyinapatientwithhypothyroidism.JEndocrinolInvest. 1992;15:49–51.
23.LamHC,WangJP,LeeJK,HoLT,HanTM,ChiangHT,etal. Tissuecontentsofendothelinvaryaccordingtothyroid hormonestatusinrat.JCardiovascPharmacol. 1993;22:S299–302.
24.StewartDJ,LevyRD,CernacekP,LanglebenD.Increased plasmaendothelin-1inpulmonaryhypertension:markeror mediatorofdisease?AnnInternMed.1991;114:464–9. 25.Balbir-GurmanA,Braun-MoscoviciY.Scleroderma-new
aspectsinpathogenesisandtreatment.BestPractResClin Rheumatol.2012;26:13–24.
26.SilvaDR,GazzanaMB,JohnAB,SiqueiraDR,MaiaAL,Barreto SS.Pulmonaryarterialhypertensionandthyroiddisease.J BrasPneumol.2009;35:179–85.
27.HashizumeT1,NumataH,MatsushitaK.Interstitial pneumoniaassociatedwithchronicthyroiditis.Nihon KokyukiGakkaiZasshi.2002;40:31–4.