www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Can
we
use
the
questionnaire
SNOT-22
as
a
predictor
for
the
indication
of
surgical
treatment
in
chronic
rhinosinusitis?
夽
,
夽夽
Pablo
Pinillos
Marambaia
a,∗,
Manuela
Garcia
Lima
a,b,
Marina
Barbosa
Guimarães
c,
Amaury
de
Machado
Gomes
a,
Melina
Pinillos
Marambaia
d,
Otávio
Marambaia
dos
Santos
e,
Leonardo
Marques
Gomes
faEscolaBahianadeMedicinaeSaúdePública(Bahiana),ProgramadePós-graduac¸ão,Salvador,BA,Brazil bUniversidadeFederaldaBahia(UFBA),Salvador,BA,Brazil
cInstitutodeOtorrinolaringologiaOtorrinosAssociados(INOOA),Salvador,BA,Brazil dSantaCasadeSãoPaulo,Otorrinolaringologia,SãoPaulo,SP,Brazil
eUniversidadedoPorto,Bioética,Porto,Portugal
fUniversidadeFederaldeSãoPaulo(UNIFESP),ProgramadePós-graduac¸ãoemOtorrinolaringologia,SãoPaulo,SP,Brazil
Received4March2016;accepted30May2016 Availableonline24June2016
KEYWORDS Nasalsurgical procedures; Qualityoflife; Sinusitis
Abstract
Introduction:Chronicrhinosinusitisisaprevalentdiseasethathasanegativeimpactonthelives ofsufferers.SNOT-22isconsideredthemostappropriatequestionnaireforassessingthequality oflifeofthesepatientsandaveryeffectivemethodofevaluatingtherapeuticinterventions; howeveritisnotusedasatoolfordecision-making.
Objective: TotestthehypothesisthattheSNOT-22scorecanpredicttheoutcomeofsurgical treatment.
Methods:Aretrospective,longitudinalandanalyticalstudy.Weevaluatedthemedicalrecords ofpatientswithchronicrhinosinusitisthatcompletedtheSNOT-22atthetimeofdiagnosis.All thepatientswereconsecutivelyreceivingcareatanotolaryngologyserviceinSalvador,Bahia fromAugust2011toJune2012.Theoutcomesofthesurgicaltreatmentofthesepatientswere obtainedfromtheirmedicalrecords.Theinitialscorewascomparedtoagroupofpatientswho werenotreferredforsurgery.Allthepatientscompletedandsignedaconsentform.
夽
Pleasecitethisarticleas:MarambaiaPP,LimaMG,GuimarãesMB,GomesAM,MarambaiaMP,SantosOM,etal.Canweusethe ques-tionnaireSNOT-22asapredictorfortheindicationofsurgicaltreatmentinchronicrhinosinusitis?BrazJOtorhinolaryngol.2017;83:451---6.
夽夽Institutions:EscolaBahianadeMedicinaeSaúdePública(Bahiana),Salvador,BA.InstitutodeOtorrinolaringologiaOtorrinosAssociados
(INOOA),Salvador,BA.Site:www.inooa.com.br. ∗Correspondingauthor.
E-mail:pablomarambaia@hotmail.com(P.P.Marambaia).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCervico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.05.010
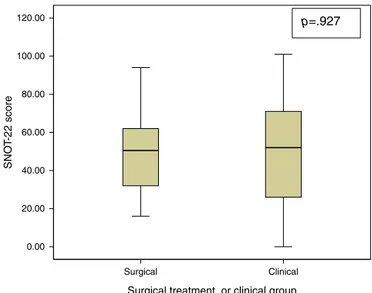
Results:Of the 88 patients withchronic rhinosinusitis, 26 hadevolved tosurgery overthe last3years.Thegroupswerehomogeneousregardinggenderandrespiratoryandmedication allergies.Thepatientsofthesurgicalgroupwere44.8+13.8yearsoldandthepatientsofthe clinicalgroupwere 38.2+12.5yearsold(p=0.517).TheaverageSNOT-22scoreofthecase groupwas49+19andtheaveragescoreofthecontrolgroupwas49+27(p=0.927).
Conclusion:TheSNOT-22wasunabletopredicttheoutcomeofsurgicalpatientswithchronic rhinosinusitis.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE Procedimentos cirúrgicosnasais; Qualidadedevida; Sinusite
PodemosusaroquestionárioSNOT-22comopreditorparaaindicac¸ãodetratamento
cirúrgiconarinossinusitecrônica?
Resumo
Introduc¸ão:A rinossinusitecrônicaéuma doenc¸a prevalenteque temum impactonegativo sobre avida dos portadores. OSNOT-22 é considerado o questionário maisadequado para avaliaraqualidadedevidadessespacienteseummétodomuitoeficazdeavaliarintervenc¸ões terapêuticas;noentanto,elenãoéusadocomoumaferramentaparaatomadadedecisões. Objetivo:TestaahipótesedequeoescoredoSNOT-22podepreverodesfechodotratamento cirúrgico.
Método: Estudo retrospectivo, longitudinal e analítico. Foram avaliados os prontuários de pacientescomrinossinusitecrônicaquepreencheramoSNOT-22nomomentododiagnóstico. Todosospacientesforamconsecutivamenteatendidosemumservic¸odeotorrinolaringologia em Salvador,Bahia,deagostode 2011ajunho de2012. Osdesfechos dotratamento cirúr-gicodessespacientesforamobtidosapartirdeseusprontuáriosmédicos.Apontuac¸ãoinicial foicomparadacomum grupodepacientesquenão foiencaminhadoparacirurgia.Todosos pacientespreencherameassinaramumtermodeconsentimentoinformado.
Resultados: Dos88pacientescomrinossinusitecrônica,26evoluíramparacirurgianosúltimos trêsanos.Osgruposforamhomogêneosquantoasexo,alergiasrespiratóriasemedicamentos. Ospacientesdogrupocirúrgicotinham44,8+13,8anoseosdogrupoclínicotinham38,2+12,5 (p=0,517).OescoremédiodoSNOT-22dogrupodocasofoide49+19eoescoremédiodo grupocontrolefoide49+27(p=0,927)
Conclusão:OSNOT-22foiincapazdepreverodesfechodospacientescirúrgicoscom rinossi-nusitecrônica.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Dataonthequalityoflifeofpatientswithchronic rhinosi-nusitis(CRS)provethatthisdiseasehasamajorimpacton theactivitiesofdailylivingofthesepatients.
IthasalreadybeenprovedthatCRSnegativelyaffectsthe QOLofsufferersincomparisontopeoplewithoutthedisease andpeoplewithotherchronicdiseaseslikecongestiveheart failureandchronicobstructivepulmonarydisease.1
Themainfocusofthesestudieswastheuseof question-nairestoevaluatetheimpactoftherapeuticinterventions. Thesamequestionnaireisgenerallyappliedbeforeandafter interventiontoagroupofpatients.Theimpactofsurgeryon thebettermentofpatientswithCRShasbeenexhaustively studiedandthereseemstobeaconsensus,especiallyinthe short-termassessment.2Studiesshowthattheimprovement
ratesofsurgeryrangefrom76%to97.5%.3,4
The SinoNasal Outcome Test 22 (SNOT-22) is an easily applied questionnaire that has been validated for use in Portuguese.5Thisinstrumenthas22questionsabout
possi-blesymptomslinkedtochronicrhinosinusitis.Eachquestion receivesascorefrom0to5,wherezeroistheabsenceofthis conditionandfiveistheworstpossible caseofthis condi-tion.Similarly,highertotalscoresrepresentaworsequality of life.According tothe 2012European Position Paperon Rhinosinusitis and Nasal Polyps(EPOS), SNOT-22is a good tool for assessing QOL in patients with CRS. Moreover, it canbeusedrepeatedlyandproducesgraphics(SNOTgrams) withSNOT-22scoresformorethanagivenmomentintime, which clearly display the resultof medicinal and surgical interventionsandexacerbationsovertime.6
example.Later,QOLbecameanadditionalparameterinthis assessmentandseveralstudieshaveusedthistoolto evalu-atepatients.Thispracticehasledtothehopethatwecan extrapolatetheuseof thequestionnairesmostlytoselect patientsfordifferenttypesoftreatmentanddeterminehow tointerpret the informationof populations outside Brazil andapplyittoourscenario.
The criteria of surgical intervention, for example, are poorly described in literature andconsequently lead to a broadgeographicalvariationofthisindicationandalossof qualityinmedicalcare.7 Measuresthatcanstandardiseor
facilitatethisdecisionwouldhelpimprovethefollow-upof thesesufferers.
Thepresentstudyaimstocomparetheaveragescoreof theSNOT-22intheinitialassessmentofpatientswithchronic rhinosinusitisandtestthehypothesisthattheSNOT-22score canpredicttheoutcomeofsurgicaltherapy.
Methods
Thisisadescriptiveandanalyticalretrospectivelongitudinal study withaconvenience sample derivedfrom aprevious studyofthesameauthor.
Weaccessedrecordsofthepatientswhoparticipatedin thepreviousstudy.Thesepatientshadreceivedcareforthe firsttimebetween2011and2012andcontinuedsupervised care at anotolaryngologyservice in Salvador,Bahia, until August2015.
Theinclusioncriteriawereliteratepatientswithchronic rhinosinusitisover18yearsofage.
The diagnosis of chronic rhinosinusitiswas determined usingthecriteriaof theEPOS-2012,6whereby chronic
rhi-nosinusitis is defined by the presence of two or more symptomsofnasalobstruction/congestion/blockage, ante-riororposteriorrhinorrhea,anosmiaorhyposmia/anosmia andfacialpain/pressureformorethan12weeksthatmust bethe resultof nasalobstruction/congestion/blockage or anteriororposteriorpurulentrhinorrhea.
Thecriteriaforexclusionwereilliteratepatients, smok-ers, patients with immune deficiency, cystic fibrosis or primaryciliarydyskinesia,patientswithbenignormalignant nasal tumours, patients with granulomatous diseases and vasculitis, patients whohad previously undergone surgery andsubjectswhorefusedtoparticipateinthestudy.
Allthepatients wereevaluatedduring thefirst consul-tation and after the confirmation of CRS. The patients subsequently completed a registration form with demo-graphic data, the SNOT-22 questionnaire validated for Portuguese8andaninformedconsentstatement.
The SNOT-22questionnairewasappliedduring thefirst consultationwhenthepatientswereevaluatedbythesame professional,in2011and2012.
After3years,themedicalrecordswerereviewedto ver-ifythereferralforclinicalorsurgicaltreatmentovertime. This referralwasmadebythesame ENTprofessionalwho wasblindedtotheSNOT-22score.
The subjectswere divided into twogroups: The group thatevolvedtothereferralfor surgeryduringthestudied periodandthegroupthatcontinuedwithclinicaltreatment. Surgerywasreferredaftermaximumclinicaltreatment hadfailedforatleast3weeks.Maximumclinicaltreatment
isdefinedastheuseoftopicalorsystemiccorticosteroids, antibiotictherapyandsalinenasalirrigation.
Thefailureofclinicaltreatmentwasdefinedasthelack ofimprovementinsymptomsreferredbytheactualpatient. In the absence of a response, an assessment computed tomographywasrequested, aswellaspossible scheduling ofafuturesurgery.
Surgery was also indicated when tomographic analysis ledto the diagnosis of a condition that required surgical treatment,namely significant anatomicalchangessuch as obstructiveseptum deviation,large or obstructive middle turbinatepneumatisationorextensive sinonasalpolyposis, andrhinosinusitisofdentalorfungalorigin.
Furthermore, surgery was indicated according to the mentionedcriteriaandtheconductofasingleprofessional, although not all the patients were necessarily operated sinceelementssuchasmotivation,personalpreferenceand expectationsregardingtheprocedureinfluencedthe deci-sion.
ThisstudywasapprovedbytheEthicsCommitteeofthe institution,underprotocoln◦181/2011.
Dataanalysis
ThesamplesizewascalculatedusingWinPepiversion11.62, withastandarddeviationoftheSNOT-22scoreofaprevious Brazilianstudyinvolving surgical patients(DP=25),Kosugi etal.,8 to detect a difference of 20 points. In this case,
50 patients would beneeded, divided into two groups of 25subjects.Consequently,thesampleofthepresentstudy exceedstherequirednumberofparticipants.
The resultswere tabulated andanalysed usingSPSS-17 software.
Thecategoricaldemographicdatalikegenderand pres-enceofcomorbiditiesandallergieswerearrangedusingthe validpercentile.The chi-squaretest wasusedtocompare categoricalvariablesbetweenthegroups.
The score of the SNOT-22questionnaire was described usingtheaverageandstandarddeviationsincethesample distributionwasnormal.
Theaveragesbetweenthegroupswerecomparedusing theunpairedt-test.
Theunpairedt-testwasalsousedtocomparetheaverage scoreofeachitemoftheSNOT-22individually.
The alpha error was considered acceptable when the valueofp<0.05.
Results
A total of 88 patients were analysed, of which 26 were patientsreferredforsurgeryand62evolvedtodrugtherapy. Table 1 shows the demographic characteristics of the sample.
Withregard totheSNOT-22score inthe first consulta-tion,itwasfound thatthe groupthat evolvedtosurgical treatment scored 49.4±19.8 and clinical group averaged 49.9±27(Table2andFig.1).
Table1 Sociodemographiccharacteristicsofpatientswithchronicrhinosinusitisreferredforsurgery(surgerygroup)andof patientswithchronicrhinosinusitisreferredforclinicaltreatment(clinicalgroup).
Variables Surgerygroup(n=26) Clinicalgroup(n=62) Significance(p)
Gender(%)
Male 12(41) 24(40.8) 0.517
Female 14(59) 38 0.517
Age(years) 44.8+13.8 38.2+12.5 0.438
Comorbidities
SAH 03 02 0.81
DM 0 02 0.307
Asthma 04 02 0.167
Allergytomedication(%)
Yes 07(22.8) 12(13.3) 0.594
No 19(77.2) 50(86.7)
Respiratoryallergy(%)
Yes 02(7.7) 05(8.1) 0.810
No 24(92.3) 57(91.9)
Surgerygroup,patientsreferredforsurgery;clinicalgroup,patientsreferredforclinicaltreatment. Significancelevelp<0.05.
Table2 QualityoflifescorewithSNOT-22ofthegroups.
Variable Surgerygroup Clinicalgroup Significance(p)
SNOT-22 49(±19) 49(±27) 0.927
SNOT-22,SinoNasalOutcomeTest.
Significancelevelp<0.05.Unpairedt-test.Average(standarddeviation).
Discussion
The QOL assessment of patients with CRS requires spe-cific questionnaires to measure the results, such as those obtained after interventions with medication and surgery.Avastamount ofstudiesusetheseinstrumentsto assesssurgicaltreatment3,4 andsome authorsbelievethat
p=.927
120.00
100.00
80.00
60.00
40.00
20.00
0.00
SNO
T-22 scor
e
Surgical
Surgical treatment or clinical group Clinical
Figure1 ShowsthecomparisonoftheSNOT-22scoreaverages ofthegroups.
questionnairescanprovideadditionalinformationfor diag-nosesanddecisionmaking.9
Soleretal.9alsoreportedthatalowscoreofthe
ques-tionnairewastheonlyfactorthatwasrelatedtothedecision to undergo surgery and concluded that questionnaires to assess quality of life should be incorporated into clinical practice.
Smith et al.10 conducted a prospective study that
showedthatpatientswithworsescoresbenefitmorefrom surgery. Moreover, patients with clinical monitoring and worse quality of life scores could switch to the surgi-cal group, which led to a significant improvement of the scores.
Birchetal.11 suggest thatpatients whoarewaitingfor
surgery should have worse endoscopic scores, more CRS symptomsandworseQOLscores.
Rudmiketal.12 concludethatthepatientwitha
SNOT-22scoreabove30pointshavea75%chanceofsignificantly changingtheir clinicalcondition withsurgery.These same patientsimprovedtheirqualityoflifeby45%.Ontheother hand,patientswithSNOT-22scores under20didnotshow significantimprovementsaftersurgery.
Inthepresentstudy,nostatisticallysignificantdifference wasfoundbetweentheaveragesoftheSNOT-22scoreofthe firstconsultationofpatientsforthegroupsthatevolvedto surgicalorclinicalreferrals.
InastudythatvalidatedSNOT-22toPortuguese,Kosugi et al.8 applied the questionnaire to 89 patients before
preoperativescoreforthegroupwiththediseaseof62.39 comparedto49+19ofoursample.
Inaprospectivestudy,Mascarenhasetal.13evaluated60
patientswithreferralsforsurgerypriortosinonasalsurgery andobtainedascoreof61.3±24.
Thepresentstudywaslongitudinalandretrospectiveand thepatientsofthissample wereinitiallytreatedclinically andreferredforsurgeryduringtheirENTmedicalfollow-up. Sincecollectionswerenotcarriedoutperiodicallyoratthe exactmomentofthesurgicalreferral,itisnotpossibleto confirmwhetherthescoredeceasedovertimeor whether thescoreofthesepatientswasworsethanthescoreofthe firstassessmentatthetimeofthesurgicalreferral.
The studies of Kosugi etal.8 and Mascarenhas et al.13
were conducted with patients with a confirmed surgical referral,which differsfromtheprofileofoursample that didnothavethatconfirmation.
IntheBrazilianscenario,thedifferencefoundbetween thescoresmayalsocorrespondtothefactthatoursample usedaservicethatattendsprivatepatients.Thismeansthat thestudiedsubjectsmayhavehadabettersocioeconomic statusthanthepatientsofthestudiesofKosugietal.8and
Mascarenhaset al.13 whose subjects used a publichealth
service.
The expected pathophysiological rationale is that patientswithreferralsforsurgeryobtainhigherscoresand that this couldexplain thebetter scores of patients with referralsfor clinical treatment. Soler etal.8 conducted a
studywith242patientsanalysedovertimeandfoundthat patientsselectedforthesurgicaltreatmentobtainedworse SNOT-22scoresthanpatientswhochoseclinicaltreatment. Factorssuchasdemographiccharacteristics,patient-doctor relationship,comorbiditiesandpersonalitydidnotinfluence thesurgicaloutcome.
In thepresent study,therewasnodifferencebetween thedemographiccharacteristicsofthegroups.Withrespect tothedoctor---patientrelationship,theauthorsbelievethat theuseofasingleevaluatorminimisesthisbias.
The outcome analysedin thisstudyis thesurgery indi-cated by the physician. This decision also depends on subjectivefactors,suchasmotivation,personalpreference andexpectationsofthepatientsregardingtheprocedure. Ofthepatientsofthisstudy,fourpatientsdidnotundergo surgeryanddecidedtocontinuewithclinicaltreatment.
The criterionfor surgical indicationswasthefailureof maximumclinicaltreatmentafterthreeweeks.Information fromtheactualpatientsregardingtheabsenceof improve-mentinsymptomsoreventheworseningofsymptomsand the will of the health professionals make selection more reliableandreducethesubjectivityofmultipleobservers.
The authors believe that these findings do not invali-datetheinformationthattheserialanalysisandprospective follow-upofthesepatientscansignificantlyenableachange ofconductandoptionfortherightmomentofsurgical refer-ral. Over time, considering the natural evolution of the disease or failure of clinical treatment with maintenance orworseningofscoresofthequestionnaire,thiscouldlead toasignificantdifferencebetweenthegroupsthatevolves tosurgerytothedetrimentofclinicaltreatment.
Hopkinsetal.,14 whovalidatedtheSNOT-22forthefirst
timein theUnited Kingdom, appliedthequestionnaire to 2077surgicalpatientsandobtainedapreoperativescoreof
41.7,which is lower than thescore found in the present study.ThisdifferencebetweentheBrazilianstudiesandUK studysuggeststhatthedifferentlifestylesandculturesof the nationsmay influence the concept of quality of life. However,the UK sample of surgical patients consisted of subjectsfromseveralcentres.Suchadiversecriteria sug-geststhatthesampleincludedpatientswithfewsymptoms ora milderformofdisease,which wouldbean errorand mayleadtoover-referralsofsurgicaltreatment.
Gillettetal.15conductedastudyandusedtheSNOT-22
on116patientswithoutsinonasaldiseaseintheUnited King-domtoknowthescoreofthequestionnaireamongpatients withoutsinonasaldisease.The justificationwasthatmany patientswhounderwentsurgeryinotherstudiesobtaineda relativelylowSNOT-22score,whichsuggeststhatthe refer-ralmayhave beeninappropriate.Patientswithlowscores mayhaveoligosymptomaticCRSormayhavebeen overdiag-nosed.
In our sample, patients were recruited from a single service andthe referral wasindicated by a singledoctor, whichminimisestheriskofchangesincriterion.Blindingin relationtotheinitialscorealsoenablesmorerobustdata.
A limitation of this study is the non-discrimination of the CRS groups. We did not distinguish the subjects with sinonasalpolyposisfromthesubjectswitheosinophilia,for example. The intention was to help the otolaryngologist indicatesurgicaltreatmentirrespectiveofthetypeof dis-ease.Furthermore,thesizeofthesampledidnotallowthe creationofsubgroups.
Conclusion
Althoughthisstudydidnotincludemultipleandserial anal-ysis,thefirstassessmentshowedthattheSNOT-22doesnot predictsurgicaloutcome.Itisthereforeimpossibletoaffirm whether these results over time, with serial assessments basedonthequestionnaire,couldestablishtheSNOT-22as agooddecision-makingtool.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.GlicklichRE,MetsonR.Thehealthimpactofchronicsinusitisin patientsseekingotolaryngologiccare.OtolaryngolHeadNeck Surg.1995;113:104---9.
2.Smith TL, Batra PS, Seiden AM, Hannley M. Evidence sup-portingendoscopicsinussurgeryinthemanagementofadult chronic rhinosinusitis: a systematic review. Am J Rhinol. 2005;19:537---43.
3.LingFT,KountakisSE.Importantclinicalsymptomsinpatients undergoingfunctionalendoscopicsinussurgeryforchronic rhi-nosinusitis.Laryngoscope.2007;117:1090---3.
4.Bhattacharyya N. Symptom outcomes after endoscopic sinus surgeryforchronicrhinosinusitis.ArchOtolaryngolHeadNeck Surg.2004;130:329---33.
5.Morley AD,SharpHR.A reviewofsinonasaloutcomescoring systems---whichisbest?ClinOtolaryngol.2006;31:103---9. 6.FokkensW,LundV,MullolJ.Europeanpositionpaperon
7.RudmikL,SolerZM,HopkinsC,SchlosserRJ,PetersA,White AA,etal.Definingappropriatenesscriteriaforendoscopicsinus surgery during management of uncomplicated adult chronic rhinosinusitis:aRAND/UCLAappropriatenessstudy.Rhinology. 2016;54:117---28.
8.Kosugi EM, Chen VG, Fonseca VMG, Cursino MMP, Mendes Neto JA, Gregório LC. Translation, cross-cultural adapta-tion and validation of SinoNasal Outcome Test (SNOT) --- 22 to Brazilian Portuguese. Braz J Otorhinolaryngol. 2011;77: 663---9.
9.SolerZM,RudmikL,HwangPH,MaceJC,SchlosserRJ,SmithTL. Patient-centereddecisionmakinginthetreatmentofchronic rhinosinusitis.Laryngoscope.2013;123:2341---6.
10.SmithTL,KernRC,PalmerJN,SchlosserRJ,ChandraRK,Chiu AG,etal.Medicaltherapyvssurgeryforchronicrhinosinusitis:a prospective,multiinstitutionalstudy.IntForumAllergyRhinol. 2011;1:235---41.
11.Birch DS, Saleh HA, Wodehouse T, Simpson IN, Mackay IS. Assessing the quality of life for patients with chronic rhi-nosinusitisusingtherhinosinusitisdisabilityindex.Rhinology. 2001;39:191---6.
12.RudmikL,SolerZM,MaceJC,DeCondeAS,SchlosserRJ,Smith TL.UsingpreoperativeSNOT-22scoretoinformpatientdecision forendoscopicsinussurgery.Laryngoscope.2015;125:1517---22. 13.MascarenhasJG,FonsecaVMG,ChenVG,ItamotoCH,Pontesda SilvaCA,GregórioLC,etal.Long-termoutcomesofendoscopic sinussurgeryforchronicrhinosinusitiswithandwithoutnasal polyps.BrazJOtorhinolaryngol.2013;79:306---11.
14.HopkinsC,BrowneJP,SlackR,LundV,TophamJ,ReevesB,etal. Thenationalcomparativeauditofsurgeryfornasalpolyposis andchronicrhinosinusitis.ClinOtolaryngol.2006;31:390---8. 15.Gillett S, Hopkins C, Slack R, Browne JP. A pilot study of