Causation and Validation of Nursing Diagnoses:
A Middle Range Theory
Marcos Venícios de Oliveira Lopes, RN, PhD, Viviane Martins da Silva, RN, PhD, and T. Heather Herdman, RN, PhD, FNI
Marcos Venícios de Oliveira Lopes, RN, PhD, is a Nursing Professor at Federal University of Ceará, Fortaleza, Brazil, Viviane Martins da Silva, RN, PhD, is a Nursing Professor at Federal University of Ceará, Fortaleza, Brazil, and T. Heather Herdman, RN, PhD, FNI, is a Visiting Professor at Federal University of Ceará, Fortaleza, Brazil and CEO/ Executive Director of NANDA International, Inc., Kaukauna, Wisconsin, United States
Search terms:
Clinical reasoning, middle-range theory, nursing diagnosis
Author contact:
[email protected], with a copy to the Editor: [email protected]
PURPOSE: To describe a predictive middle range theory (MRT) that provides a process for validation and incorporation of nursing diagnoses in clinical practice.
DATA SOURCES: Literature review.
DATA SYNTHESIS: The MRT includes definitions, a pictorial scheme, proposi-tions, causal relationships, and translation to nursing practice.
CONCLUSIONS: The MRT can be a useful alternative for education, research, and translation of this knowledge into practice.
IMPLICATIONS FOR NURSING PRACTICE: This MRT can assist clinicians in
understanding clinical reasoning, based on temporal logic and spectral interaction among elements of nursing classifications. In turn, this understanding will improve the use and accuracy of nursing diagnosis, which is a critical component of the nursing process that forms a basis for nursing practice standards worldwide.
Introduction
Nursing is an emergent profession, but remains on the margins of other professional disciplines, for example, soci-ology, psychsoci-ology, epidemisoci-ology, and environmental sci-ences (Moule & Goodman, 2014). These disciplines guide research and nursing practice, but models that bring coher-ence and meaning to the findings are required, to enable their incorporation in practice scenarios without the loss of nursing’s professional uniqueness (Smith & Liehr, 2008).
Every discipline is defined by the phenomena represent-ing its core practice; those focus areas for which its members are considered responsible. Phenomena for which nurses have acccountability have been named differently by different scholars, including nursing problems, adapta-tion problems, nursing phenomena, clinical condiadapta-tions, and so on (Alligood & Tomey, 2009; International Council of Nurses [ICN], 2009; Roy, 2009). Each of these terms includes the action “to diagnose,” although there is no con-sensus among nurses about the adoption of a system to organize these phenomena within a nursing classification.
The incorporation of diagnoses by a profession allows it to establish its field of action, and can help clinicians and researchers to focus their actions on the development of nursing knowledge. However, there is still a gap between nursing research and practice in various scenarios of care. The development of middle range theories (MRTs) has been suggested as an approach for reducing this gap; it refers to
a set of related ideas that are focused on a particular dimension of nursing knowledge, including a limited number of concepts and propositions, described at a specific and concrete level, which are directly linked to research and practice (Smith & Liehr, 2008).
There are three different MRT types: descriptive, explanatory, and predictive. The first describes or classifies a phenomenon, such as taxonomies of nursing diagnoses, which organize nursing phenomena from a single concept (nursing diagnosis). Explanatory MRT involves the relation-ships between multiple concepts that are concerned with the manner and extent to which one concept is related to others. Some clinical reasoning models follow the idea of an explanatory MRT, such as the Outcome–Present state–Test (OPT) model, in which interrelated networks of diagnoses, or “clinical reasoning webs,” should be established (Pesut & Herman, 1999). Predictive MRT seeks to establish the precise relationships between concepts, or effects from one or more concepts, on one or multiple concepts, aiming to describe how changes occur within a phenomenon (Fawcett, 2005).
Although the NANDA-International (NANDA-I) taxonomy would be considered a descriptive MRT, and there are clini-cal reasoning models that are characterized as explanatory MRTs, there are no theories that bring together the knowl-edge already developed on nursing diagnosis to discuss the causal links between their clinical elements or their relationship with the nursing intervention and outcome
classifications. Causation models are essentially predictive, and allow the generation of robust clinical evidence and the translation of the knowledge developed in research into clinical practice. Thus, this article describes a predictive MRT, establishing causal relationships to direct studies on the validation of nursing diagnoses and its translation into practice.
Methods
This study followed six stages: defining the approach to construct the MRT; definition of conceptual models to be analyzed; definition of key concepts; developing a pictorial diagram; construction of propositions; and establishment of causal relationships and evidence for practice (Roy, 2014).
Defining the Approach to Construct the MRT
The MRT was derived from the idea that clinical reason-ing steps include elements that must be combined to represent the phenomenon of interest. In addition, the clini-cal reasoning process is directly related to diagnostic validation methods used in research and to clinical-epidemiological causal models. Thus, construction of the MRT included the combination of elements that comprise clinical reasoning models, validation processes for nursing diagnoses, and epidemiological causal models.
Definition of Conceptual Models to Be Included
The five main clinical reasoning models used in nursing education were included: Gordon (1987), Risner (1986), OPT (Pesut & Herman, 1999), Lunney (2009), and Think Aloud (Herdman, 2014). Five nursing diagnosis validation models were also included in the study: Gordon (1987), Hoskins (1989), Fehring (1987), Lopes, Silva, and Araujo (2012), and Walker & Avant’s (2013) concept analysis model. The latter was included because it is a model used recurrently in the other four mentioned validation models. Finally, we included epidemiological causal models: linear, trigger effect, domino effect, feedback, butterfly effect, quality leap, and sufficient cause (Brown, 1995; Bunge, 1979; Pearl, 2000; Rothman, Greenland, & Lash, 2013).
Definition of Main Concepts
After review and analysis of the models, three main con-cepts were established to compose the MRT: clinical ante-cedents, clinical consequents, and essential attributes. These concepts were defined and related to three other secondary concepts: clinical spectrum, causality, and temporality.
Developing a Pictorial Diagram
A pictogram was developed with the primary and second-ary concepts of the MRT to facilitate understanding of
causal relationships. The scheme is divided into three parts, which include the temporal relations between its concepts, from the perspective of a nursing diagnosis as a clinical reasoning process and as the product of the clinical judgment.
Construction of Propositions
For the construction of explanatory relationships between concepts, four propositions related to clinical indi-cators, and five propositions related to the etiological factors, were established. These propositions underlie the construction of predictive causal relationships for the next step.
Establishment of Causal Relationships and Evidence for Practice
Interrelationships that allow the establishment of causal relationships have been defined. Examples for each type of causation related to nursing diagnoses are described to provide better understanding of its clinical use.
An MRT of Causation in Nursing Diagnosis
The MRT developed for the validation of nursing diagno-ses depends on two basic aspects: how a nursing diagnosis is defined (process or product) and the establishment of three essential elements that are objects of the validation process: essential attributes, clinical antecedents, and consequents.
Definition of Main Concepts and Pictorial Diagram
Nursing diagnosis can be defined as clinical reasoning process which allows the establishment of relationships between its elements, through a series of cognitive activi-ties, including phases of collection, processing, clustering, and naming (Lunney, 2009). A nursing diagnosis can also be seen as the product or outcome of this reasoning process, and therefore as an element of the nursing process whose previous step is data collection, and whose later steps refer to the establishment of interventions to achieve outcomes (Gordon, 1987).
Model of Causation and Nursing Diagnosis as a Process
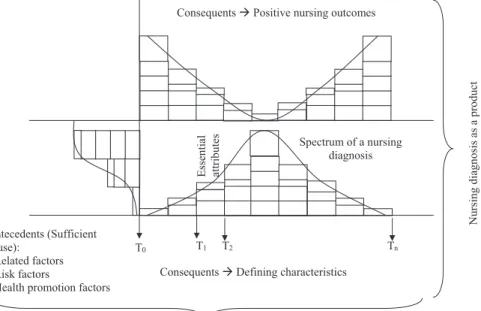
Clinical antecedents (etiologic elements). From the perspective of a clinical reasoning and judgment process, the establishment of a nursing diagnosis begins with the interaction between supposed etiological factors that inter-act with the person/group, producing physiological and/or psychosocial responses (T0 time in Figure 1). The clinical development of etiological factors (antecedents) can be seen in the lower left corner of the pictorial scheme. Each rectangle represents a different etiologic factor, and the thickness of each rectangle represents its clinical spectrum. These clinical antecedents may be related factors, risk factors, or health promotion factors. Although they are dif-ferent terms used in difdif-ferent contexts, these three ele-ments represent the same idea, that is, a set of factors that converge as the cause of a phenomenon of focus for nursing practice.
Essential attributes. Over time, etiological elements come together and change their clinical spectrum so that, at any given time, essential attributes of a diagnosis will be highlighted, and a specific clinical situation will be identified as a diagnosis. Thus, multiple factors can interact and con-verge to produce a condition of diagnostic sufficiency, in which a minimum clinical threshold required to establish the diagnosis (essential attributes) is reached. This is illustrated in the pictorial scheme, between T1and T2.
Clinical consequents (clinical indicators). Clinical consequents represent an exacerbation of the essential
attributes associated with exposure to clinical antecedents. Thus, essential attributes also result from the interaction between the clinical antecedents and the person, because it is impossible to determine the exact moment when a human response is established. The interaction of clinical anteced-ents with the person will result in a gradual and intense response, which depends on the spectrum of this exposi-tion. At the lower right corner of Figure 1, the occurrence of an increasing number of clinical indicators, with the wors-ening of its spectrum, is pictured. The continuous interac-tion of the person with clinical antecedents brings forth new consequents, as well as an exacerbation of their clinical spectrum, so as to show a greater degree of impairment. This may continue until an intervention is implemented or the diagnosis reaches its maximum clinical threshold. Thereafter, there will be a gradual reduction of the clinical diagnosis spectrum (Tn). Clinical consequents are represented in the NANDA-I taxonomy as defining characteristics.
Model of Causation and Nursing Diagnosis as a Product
The causal relationship between etiological factors (antecedents) and effects (consequents), when considering the nursing diagnosis as the product of clinical reasoning, is based on a different relationship from that described when considering diagnosis as a process. Clinical antecedents follow the same definition of the previous approach. However, the essential attributes comprise a set of clinical indicators (defining characteristics) identified as the maximum clinical threshold.
Figure 1. A Causation Model to Represent the Relationship Among Nursing Diagnosis Elements
Tn
T2
T1
T0
Antecedents (Sufficient cause):
- Related factors - Risk factors
- Health promotion factors
Essenti
al
at
tr
ib
u
te
s
Consequents Defining characteristics Consequents Positive nursing outcomes
Nursing diagnosis as a product
Nursing diagnosis as a process
In this approach, consequents are represented by out-comes sensitive to nursing care, namely, the goals to be achieved with nursing interventions. This approach approxi-mates the classical methods of concept analysis, in which the core concept (e.g., self-esteem) is a neutral response (Walker & Avant, 2013). From this conceptual core, one seeks to identify antecedents (related/risk/health promot-ing factors), essential attributes (definpromot-ing characteristics), and consequents (outcomes/goals).
The clinical spectrum of the defining characteristics is the inverse representation of nursing outcome indicators. Thus, when the clinical spectrum of a defining characteristic is poor (significant compromise), the corresponding outcome indicator shows a high value (positive outcome) and vice versa. This relationship can be seen by comparing the lower right corner to the upper right corner of Figure 1. The limitation of this approach in terms of validation is that the goals to be achieved are not components of a diagnosis. The approach of diagnosis as a clinical reasoning process is sufficient to support a study of diagnostic vali-dation, and the proposals presented in the following section refer only to this approach. Furthermore, proposals con-cerning the second approach discussed previously can be derived similarly to the first.
Propositions
Some propositions are essential to understanding how a nursing diagnosis is developed and manifested by an individual. The propositions can be delineated as those related to clinical consequents and those related to clinical antecedents.
Clinical consequents. It is critical to consider four propositions related to clinical consequents of a diagnosis: (1) Different diagnoses can share the same clinical conse-quents. This means there are defining characteristics that compose the clinical framework of multiple diagno-ses. An example isdyspnea, a defining characteristic in the nursing diagnoses ofactivity intolerance(00092), decreased cardiac output (00029), and ineffective breathing pattern(00032).
(2) Clinical consequents common to several diagnoses may have different degrees of pertinence for each diagnosis. A defining characteristic, although found in several diagnoses, may be clinically the most representative characteristic for a particular diagnosis. For example, an abnormal breathing pattern may be more strongly associated withineffective breathing patternthan with impaired gas exchange(00030).
(3) Clinical consequents have a spectrum that varies over time and exposure to antecedents. The spectrum of a consequent is the intensity expressed by the person to this element. Thus, an individual with asthma, exposed for a period of time to a specific amount of smoke (related factor forineffective airway clearance, 00031)
may present an ineffective cough (defining characteris-tic) that is more or less intense, depending on the expo-sure time and/or quantity of smoke with which he came into contact.
(4) The spectrum of the consequents is directly related to the nursing diagnosis spectrum. There is a direct rela-tionship between the intensity of a person’s response to each clinical consequent and the degree of impairment associated with the nursing diagnosis of interest. For example, a person who has mild changes in frequency, rate, and respiratory depth probably demonstrates a milder clinical condition ofineffective breathing pattern as compared to individuals with more severe changes in these defining characteristics.
Clinical antecedents. Propositions related to the clini-cal antecedents of a nursing diagnosis have a strong asso-ciation with the previous discussion on spectrum because of the temporal and clinical relationship among the elements that comprise a diagnosis:
(1) Different diagnoses can share the same clinical ante-cedent. This proposition denotes the possibility of mul-tiple human responses associated with the same related factor. For example, social isolation is described as a possible causal factor ofhopelessness(00124) andrisk for loneliness(00054).
(2) Clinical antecedents common to several diagnoses may have different degrees of pertinence for each diagnosis. As previously discussed with the clinical consequents, antecedents may have a stronger association with a particular diagnosis. For example, immobility may be more strongly associated with dysfunctional gastroin-testinal motility (00196) than with disturbed sleep pattern(00198).
(3) Clinical antecedents have spectra that vary with time of exposure and the ability to cause damage to an indi-vidual. The spectrum of a clinical antecedent concerns the intensity of its effect on a person. Such intensity will depend on how long the person remains in contact with this antecedent, and/or the power that this antecedent has to cause a more intense change. For example, radia-tion exposure may cause impaired skin integrity (00046), depending on the quantity and duration of the exposure. Thus, prolonged radiation exposure repre-sents a high spectrum antecedent that would result in more intense symptomatology.
(4) The spectrum of a nursing diagnosis is directly related to the spectrum of the clinical antecedent. This propo-sition is a consequence of the third and fourth proposi-tions for clinical consequents, and the third proposition for clinical antecedents.
(00093) may be a causitive factor for the development ofineffective breathing pattern.
Causal Relationships and Translation to Nursing Practice
Clinical antecedents can act in different ways on causal processes (Table 1). Predisposing factors act by increasing the susceptibility of an individual to a phenomenon, for example, age≥65 years, which is identified as one of the
elements of the diagnosis,risk for falls(00155). Disabling factors affect the recovery period or can make of health promotion behaviors difficult, generating a poor health state or extending the effect of other causative agents (Timmreck, 2002). For example, being economically disad-vantaged and having inadequate nutrition are associated with diagnoses such asimbalanced nutrition, less than body requirements (00002), risk for disproportionate growth (00113), orrisk for delayed development(00113).
Some etiological factors act as precipitating factors of the causation process, namely, by initiating the interactions between the environment and individuals (Merrill, 2010). Exposure to high environmental temperature initiates the processes that will culminate inhyperthermia(00007), just as a chemical injury agent can lead to disruption of the dermis, as identified in the diagnosis ofimpaired skin integ-rity(00046).
Finally, reinforcing factors act specifically as potentia-tors of preexisting conditions. In general, these facpotentia-tors rep-resent specific situations associated with other previously described categories (Jeckel, Katz, Elmore, & Wild, 2007). For example, vigorous physical activity may potentiate the effects of solar exposure and lead to a more rapid, more intense presentation ofhyperthermia. In addition to being involved in the causal chain, these reinforcing factors have a direct relationship with the clinical spectrum of the diag-nosis because prolonged exposure leads to a more serious degree of clinical impairment.
Reinforcing factors include unhealthy environmental conditions, for example, inadequate working conditions. Persons performing activities with excessive workload, or working with an excessive demand of responsibilities, may be exposed to other factors, and may develop nursing diag-noses such as sleep deprivation (00096), caregiver role strain(00061), andrisk for injury(00035).
An interesting aspect of reinforcing factors is their rela-tionship to health promotion diagnoses. NANDA-I does not describe etiological factors for this type of nursing diagno-sis. The initial idea is that such diagnoses are innate and therefore are not influenced by environmental interaction (physiological, social, psychological, or spiritual). However, few characteristics that affect health behaviors are innate only. When considering the diagnosis readiness for enhanced breastfeeding (00106), you can see that, although there is expressed desire to provide breast milk for a nursing mother, this desire was influenced by reinforc-ing factors such as knowledge of the benefits of breastfeeding, shared experiences with other mothers, family and cultural influences, and so on.
On the other hand, if these breastfeeding reinforcing factors are replaced by a precipitating factor (e.g., as maternal illness) or contraindications to breastfeeding (e.g., maternal medication), this health promotion behavior can be overridden by a problem-focused diagnosis, such as interrupted breastfeeding(00105). In addition, reinforcing factors, such as a maternal breast anomaly or supplemental feedings with artificial nipples, can lead to the more serious clinical condition ofineffective breastfeeding(00104). Thus, Figure 1 includes health promotion factors among the etio-logic factors of nursing diagnoses, even though these are not included within the current NANDA-I terminology.
Causal relationship models. These four types of etio-logical factors converge in multiple potential causal rela-tionships, and provide a theoretical basis for the validation process of these diagnostic components. At least seven models of causal relationship apply to nursing diagnosis validation research: linear causality, trigger effect, domino effect, feedback, butterfly effect, quality leap, and sufficient cause (Table 2).
The linear causal model, also known as simple causality, suggests that an antecedent causes a proportional conse-quent (a linear effect) (Bunge, 1979). In this model, the longer the duration and the intensity of the exposure to an antecedent, the stronger the spectrum of the consequents. Thus, the spectrum of exposure to a chemical injury agent will determine the spectrum of its defining characteristics, and the extent of the subsequentimpaired tissue integrity (diagnostic spectrum).
Table 1. Classification of antecedents for nursing diagnoses
Category Definition
Example
Antecedent Nursing diagnosis
Predisposing factors Create a susceptibility status Age, impaired balance, gender Risk for falls
Disabling factors Interfere with recovery or health promotion Poverty, malnutrition Risk for disproportionate growth Precipitating factors Initiate the causal chain Exposure to chemical injury agent Impaired skin integrity
Reinforcing factors Amplify the effect of an existing condition Overstimulating environment, prolonged discomfort
The trigger effect model describes situations in which an antecedent causes a disproportionate effect, namely, in a nonlinear manner (Bunge, 1979). In this model, a low trum antecedent causes consequents with a severe spec-trum and a final extreme response. An example of this model, applicable to nursing diagnosis, is the relationship between bladder distension and autonomic dysreflexia (00009), in which a minor bladder distention may lead to an exaggerated stimulation of the sympathetic nervous system, thus causing more severe symptoms.
The domino effect model, also known as a chain reaction, suggests that an antecedent causes a consequent with a different spectrum (nonlinear), which will cause a subse-quent change with a similar spectrum; this will then be followed by additional change, occurring in a linear sequence (Susser, 1973). In this model, a mild spectrum antecedent causes a diagnosis with a severe clinical spec-trum that will lead, sequentially, to other diagnoses with different clinical spectra. Sleep apnea is an antecedent that, even in a mild clinical condition, can lead to intense degrees of sleep deprivation. This diagnosis, in turn, may cause fatigue, which in turn may lead to the consequent diagnosis, ineffective breathing pattern.
A characteristic of the chain reaction is a need to iden-tify the initial component of the causal chain. In the pre-vious example, removal of the initial antecedent (sleep apnea) can lead to resolution of three diagnoses, which identifies two facts: (1) an extensive list of diagnoses is not a guarantee of a good clinical reasoning process, and (2) seeking out different interventions for multiple diagnoses originating from the same antecedent can lead to ineffi-cient care.
The feedback model describes situations in which the consequent changes the antecedent (Mourão Júnior & Abramov, 2011). In this case, both diagnoses are anteced-ents of each other, and the more severe the clinical spec-trum of one, the more serious the specspec-trum of the other will become. This model describes two different clinical
situa-tions: the vicious cycle consisting of problem-focused nursing diagnoses, and the virtuous circle, consisting of health promotion diagnoses.
The relationship between impaired physical mobility (00085) andactivity intolerance(00092) is an example of negative feedback, which creates a vicious cycle. In this case, the more intense the mobility limitation, the greater the reduction in the ability and willingness to complete a physical activity. In turn, a reduction in the ability to perform an action will prolong the physical recovery, which can lead to damage of the musculoskeletal system and make it more difficult to restore one’s ability to move independently.
On the other hand, individuals with readiness for enhanced knowledge (00161) tend to show greater readi-ness for enhanced communication(00157) and vice versa, featuring positive feedback or the virtuous cycle. This is another example of causal model for identifying etiologic factors for health promotion diagnoses.
The model known as the butterfly effect is derived from chaos theory (Brown, 1995). It refers to situations in which an insignificant change causes changes so disproportionate that they change the entire system at the point that the initial change occurred. This model combines the character-istics of the domino effect and feedback models. Thus, a low spectrum antecedent causes sequential consequents, with increasingly intense spectra, culminating in a serious clinical outcome. A caregiver of an individual with spinal cord injury may not receive appropriate guidance about the patient’s response to this injury or its consequences, or he may inter-pret the provided information incorrectly. This misconcep-tion can lead to a misunderstanding related to the need to avoid particular situations in the patient, such as bladder distension. The occurrence of bladder distension may cause autonomic dysreflexia, causing the death of patient.
The quality leap model predicts that when small quanti-tative changes in the system exceed a certain limit, the quality of the system changes abruptly (Bunge, 1979). This
Table 2. Causality models for nursing diagnosis
Model Definition Example
Linear effect An antecedent causes a proportional consequent. Chemical injury agent andimpaired skin integrity
Trigger effect An antecedent causes a disproportional consequent. Bladder distension andautonomic dysreflexia
Domino effect An antecedent causes a disproportional consequent that will cause sequential and proportional consequents.
Sleep apnea→sleep deprivation→fatigue→
ineffective breathing pattern
Feedback effect The consequent modifies the antecedent. Impaired physical mobilityandactivity intolerance
(vicious cycle)Readiness for enhanced knowledge
andreadiness for enhanced communication
(virtuous cycle) Butterfly effect A subclinical antecedent causes disproportional consequents,
amending all initial system.
Misinformation→deficient knowledge→bladder distension→autonomic dysreflexia→death Quality leap Small quantitative changes in a system exceed a threshold at
which the system quality changes abruptly.
Active fluid volume loss anddeficient fluid volume
Sufficient causes The interaction between antecedents forms a minimum set of elements that produce a specific human response.
model is mainly applicable for diagnoses associated with critically ill/injured patients. In this case, the constant inter-action with the clinical antecedent, although mild spectrum, at any given time may lead to a consequent with an exacer-bated clinical spectrum. A person who has coagulation dis-orders and develops a minor, subclinical internal bleed, with active fluid volume loss may, at any given time, present with deficient fluid volume (00027), leading to hypovolemic shock.
The model of sufficient causes defines the interaction among clinical antecedents from a minimum set of ele-ments that produce a specific human response (Rothman et al., 2013). Thus, the occurrence of a nursing diagnosis would be related to the interaction among multiple clinical antecedents. A fall occurrence can be determined by a confluence of four antecedents, for example, insufficient lighting, cluttered environment, impaired balance, and insufficient antislip material in the bathroom. All of these factors have some degree of influence on fall occurrence, and therefore, patients with an interaction of these clinical antecedents are identified with the diagnosis,risks for falls (00155). However, the mere presence of one of them may not be sufficient for this phenomenon to occur.
The model of sufficient causes is flexible and can incor-porate the ideas of the other models for each case compo-nent. Additionally, it provides a broader view of causal relationships because it replaces the idea of a one-to-one relationship between antecedent and consequent, by taking into account the particularities of each clinical situation.
Conclusion and Implications
The ideas in this article represent an adaptation of con-cepts and causality models often used in epidemiology. Clas-sical methods for nursing diagnosis validation have been based on a timeless relationship of elements. An approach combining causal models from epidemiology and concept analysis within nursing provides an interesting, alternative method for nursing diagnosis validation research, which considers the differences between diagnosis elements.
The definitions and examples previously described may be useful to address the specific content of the disciplines of epidemiology and semiology, focused on teaching nursing diagnosis and methods of clinical and epidemiologi-cal assessment. This MRT can assist in teaching the cliniepidemiologi-cal reasoning process, considering the components of a nursing diagnosis, and its temporal and spectral relation-ship with elements of other nursing classifications. For example, it can support the clinical reasoning process by integrating causal factors, clinical indicators, and outcomes sensitive to nursing intervention. In addition, the assump-tions developed in the MRT allow the definition of specific conceptual maps for complex causal relationships involving multiple diagnoses, and directing the focus of nursing action on the diagnosis that initiates the causal chain or on one that presents direct relationship with a set of other diagnoses. This approach will provide the student with a
clearer understanding of the interaction processes between causal factors and clinical indicators that indicate the threshold at which the human response is noticeable and likely to receive a diagnostic label. Finally, clinicians can use the approach described in the MRT to address their cogni-tive processes and establish more efficient treatment plans that consider elements of the causal chain, as well as the level of patient impairment.
References
Alligood, M. R., & Tomey, A. M. (2009).Nursing theorists and their work(7th ed.). Philadelphia, PA: Mosby.
Brown, C. (1995).Chaos and catastrophe theory. Thousand Oaks, CA: Sage Publications.
Bunge, M. (1979).Causality and modern science(3rd ed.). New York: Dover Publications.
Fawcett, J. (2005). Middle-range nursing theories are necessary for the advancement of the discipline.Aquichan,5(1), 32–43.
Fehring, R. J. (1987). Methods to validate nursing diagnoses.Heart and Lung: The Journal of Critical Care,16(6), 625–629.
Gordon, M. (1987).Nursing diagnosis: Process and application. New York: McGraw-Hill.
Herdman, T. H. (2014). Método Think Aloud: uma ferramenta de educação para melhorar o raciocínio clínico e diagnóstico. In T. H. Herdman, M. V. O. Lopes, M. A. Almeida, & T. C. M. Chianca (Eds.),PRONANDA Programa de atualização em diagnósticos de enfermagem: Ciclo 2(pp. 9–32). Porto Alegre, Brazil: Artmed.
Hoskins, L. M. (1989). Clinical validation, methodologies for nursing diagnoses research. In R. M. Carrol-Johnson (Ed.), Classification of nursing diagnoses: Proceedings of the eighth conference of North Ameri-can Nursing Diagnosis Association (pp. 126–131). Philadelphia: JB Lippincott.
International Council of Nurses (ICN). (2009).International Classification for Nursing Practice Version 2. Geneva, Switzerland: Author.
Jeckel, J. F., Katz, D. L., Elmore, J. G., & Wild, D. M. G. (2007).Epidemiology, Biostatistic, and Preventive Medicine(3rd ed.). Philadelphia: Saunders Elsevier.
Lopes, M. V. O., Silva, V. M., & Araujo, T. L. (2012). Methods for establishing the accuracy of clinical indicators in predicting nursing diagnoses. Inter-national Journal of Nursing Knowledge,23(3), 134–139.
Lopez, M. (2001).O processo diagnóstico nas decisões clínicas: ciência, arte, ética. Rio de Janeiro, Brazil: Revinter.
Lunney, M. (2009).Critical thinking to achieve positive health outcomes(2nd ed.). Oxford, UK: Wiley-Blackwell.
Merrill, R. (2010).Introduction to epidemiology(5th ed.). Sudbury, MA: Jones and Bartlett Publishers.
Moule, P., & Goodman, M. (2014). Nursing research: An introduction. In P. Moule & M. Goodman (Eds.),Sources of nursing knowledge(2nd ed., pp. 21–30). London: Sage Publications Ltd.
Mourão Júnior, C. A., & Abramov, D. (2011). Fisiologia essencial. Rio de Janeiro, Brazil: Guanabara Koogan.
Pearl, J. (2000).Causality: models, reasoning, and inference. Cambridge, UK: Cambridge University Press.
Pesut, D. J., & Herman, J. (1999).Clinical reasoning: The art & science of critical & creative thinking. Albany, NY: Delmar Publishers.
Risner, P. B. (1986). Diagnosis: Analysis and synthesis of data. In J. W. Griffith-Kenney & P. J. Christensen (Eds.),Nursing process: Appli-cation of theories, frameworks, and models(2nd ed., pp. 124–151). St. Louis, MO: Mosby.
Rothman, K. J., Greenland, S., & Lash, T. L. (2013).Modern epidemiology(3rd ed.). Philadelphia: Lippincott Williams & Wilkins.
Roy, C. (2009).The Roy Adaptation Model(3rd ed.). Upper Saddle River, NJ: Pearson Education.
Roy, C. (2014).Generating middle range theory: From evidence to practice. New York: Springer Publishing Company.
Smith, M. J., & Liehr, P. R. (2008).Middle range theory for nursing(2nd ed.). New York: Springer Publishing Company.
Susser, M. (1973).Causal thinking in the health sciences. New York: Oxford University Press.
Timmreck, T. C. (2002).An introduction to epidemiology(3rd ed.). Sudbury, MA: Jones and Bartlett Publishers.