Chagasic enter opathy
Enteropatia chagásica
Ulysses G. Meneghelli
1ABSTRACT
In vo lve m e n t o f th e h o llo w o rga n s o f th e d i ge sti ve a p p a ra tu s c a n o c c u r i n p a ti e n ts i n th e c h ro n i c p h a se o f Ch a ga s’ d i se a se . Th e b a si c m e c h a n i sm i s d e stru c ti o n o f n e u ro n s o f th e e n te ri c n e rvo u s syste m . Wh e re a s m e ga e so p h a gu s a n d m e ga c o lo n a re th e m o st n o ta b le a n d m o st e x te n si ve ly stu d i e d e x p re ssi o n s o f th e d i ge sti ve f o rm o f Ch a ga s’ d i se a se , i n vo lve m e n t o f th e sm a ll i n te sti n e ( Ch a ga si c e n te ro p a th y) i s le ss f re q u e n t a n d le ss k n o wn th a n i n vo lve m e n t o f th e two a b o ve m e n ti o n e d e n ti ti e s. Ch a ga si c e n te ro p a th y c a n b e re sp o n si b le f o r i m p o rta n t c li n i c a l a n d la b o ra to ry m a n i f e sta ti o n s re se m b li n g th o se o f d ysp e p ti c syn d ro m e , i n te sti n a l p se u d o - o b stru c ti o n a n d b a c te ri a l o ve rgro wth i n th e sm a ll i n te sti n e . Ch a ga si c e n te ro p a th y a lso i n vo lve s p e c u li a r f u n c ti o n a l c h a n ge s, e sp e c i a lly th o se re la te d to m o to r a c ti vi ty o f th e o rga n a n d to i n te sti n a l a b so rp ti o n o f c a rb o h yd ra te s. In p ra c ti c e , th e d i a gn o si s i s b a se d o n ra d i o gra p h i c d o c u m e n ta ti o n o f d i la ti o n o f vi sc e ra l se gm e n ts. Tre a tm e n t c o n si sts o f c li n i c a l c o n tro l o f th e a b o ve syn d ro m e s a n d , e ve n tu a lly, a p p ro p ri a te su rgi c a l o p e ra ti o n s.
Ke y-words: Ch a ga s’ d i se a se . Ch a ga si c e n te ro p a th y. Ph ysi o p a th o lo gy o f th e sm a ll i n te sti n e .
RESUMO
O c o m p ro m e ti m e n to d o s ó rgã o s o c o s d o a p a re lh o d i ge sti vo p o d e o c o rre r n o s p o rta d o re s d a f a se c rô n i c a d a d o e n ç a d e Ch a ga s. O m e c a n i sm o b á si c o é a d e stru i ç ã o d o s n e u rô n i o s d o si ste m a n e rvo so e n té ri c o . Co n q u a n to o m e ga e sô f a go e o m e ga c ó lo n se ja m a s e x p re ssõ e s m a i s n o tá ve i s e e stu d a d a s d a f o rm a d i ge sti va d a d o e n ç a d e Ch a ga s, o e n vo lvi m e n to d o i n te sti n o d e lga d o ( e n te ro p a ti a c h a gá si c a ) é m e n o s f re q ü e n te e m e n o s c o n h e c i d o d o q u e o d a s d u a s e n ti d a d e s m e n c i o n a d a s. A e n te ro p a ti a c h a gá si c a p o d e se r re sp o n sá ve l p o r i m p o rta n te s m a n i f e sta ç õ e s c lí n i c a s e la b o ra to ri a i s q u e se a sse m e lha m à s da s sí n dro m e s di spé pti c a , de pse u do - o b stru ç ã o i n te sti n a l e de su pe rc re sc i m e n to b a c te ri a n o n o i n te sti n o d e lga d o . A e n te ro p a ti a c h a gá si c a ta m b é m a c a rre ta p e c u li a re s a lte ra ç õ e s f u n c i o n a i s, p a rti c u la rm e n te re la c i o n a d a s à a ti vi d a d e m o to ra d o ó rgã o , b e m c o m o , à a b so rç ã o i n te sti n a l d e c a rb o i d ra to s. Na p rá ti c a , o d i a gn ó sti c o f u n d a m e n ta - se n a d o c u m e n ta ç ã o ra d i o grá f i c a d a e c ta si a d e se gm e n to s d a ví sc e ra . O tra ta m e n to c o m p o rta o c o n tro le c lí n i c o d a s sí n d ro m e s a c i m a m e n c i o n a d a s e , e ve n tu a lm e n te , o p e ra ç õ e s c i rú rgi c a s a p ro p ri a d a s.
Pal avr as-chave s: Do e n ç a d e Ch a ga s. En te ro p a ti a c h a gá si c a . Fi si o p a to lo gi a d o i n te sti n o d e lga d o .
1 . De par tame nto de Clínic a Mé dic a da Fac uldade de Me dic ina de Rib e ir ão Pr e to da Unive r sidade de São Paulo , Rib e ir ão Pr e to , SP.
Addr e ss to: Dr. Ulysse s G. Me ne ghe lli. Av. Sumar é 4 1 4 , 1 4 0 2 5 - 4 5 0 Rib e ir ão Pr e to , SP, B r azil Fax: 5 5 1 6 6 3 3 -6 6 9 5
e -mail: ugme ne gh@ fmr p. usp. b r Re c e b ido par a pub lic aç ão e m 2 5 /3 /2 0 0 4 Ac e ito e m 2 /4 /2 0 0 4
Chagas’ disease is provoked by the protozoon Trypa no so m a
c ru zi, Chagas, 1 9 0 9 . The ac ute fo rm o f the disease c an be
partic ularly severe or even lethal, but may also be non-apparent or may be c onfused with other ac ute infec tious diseases. More
frequently the disease is diagnosed during the c hronic phase,
many years after the ac ute phase, when the major and most
c o mmo n manife statio ns o f the dise ase ar e due to c ar diac involvement ( arrhythmias, disorders of nerve impulse conduction,
cardiomegaly, heart failure and sudden death) and/o r dige stive
tr a c t in vo lve m e n t ( dys ph a gia , m e ga e s o ph a gus , in te s tin a l
c o n s tipa tio n , m e ga c o lo n ) . Th e pr e do m in a n c e o f o n e o r
ano ther o f these manifestatio ns is the basis fo r the rec o gnitio n o f th e c a r dia c1 0 a n d dige s tive5 6 fo r m s o f th e dis e a s e , a s
o ppo s e d to th e in de te r m in a te fo r m . Th e la tte r fo r m is
c ha r a c te r ize d b y: 1 . a po s itive s pe c ific s e r o lo gic te s t o r
po sitive de m o nstr atio n o f the par asite ; 2 . ab se nc e o f any sympto m and/o r sign o f the dise ase ; 3 . no r mal c o nve ntio nal
image s2 8. Ho we ve r, it must b e c o nside r e d as a tr ansito r y fo r m
o f the dise ase , sinc e ab o ut 2 -5 % o f patie nts with this fo r m pr o gr e ss to the sympto matic c ar diac and/o r dige stive dise ase
e ac h ye ar1 6 5 8 .
The etiology of megaesophagus and megacolon, which are
endemic in South America and especially in the rural zones of
Brazil, was only linked to Chagas’ disease more than 4 0 years after th e dis c o ve r y o f th e dis e a s e , b a s e d o n s e r o lo gic1 9 a n d
histopathological2 5 studies, on experimental reproduction of the
disease in laboratory animals4 4, and on patient follow-up after the
ac ute phase o f the disease5 4 . Altho ugh megaeso phagus and
megacolon are the most common and most expressive digestive
manifestations of the chronic phase of Chagas’ disease, others occur
less fr equently, suc h as megaduo denum, megaj ej unum and
megaileum. In addition, dysfunc tion of the small intestine of Chagasic patients can be demonstrated by functional tests even in
the absence of symptomatic manifestations. The involvement of
the small intestine by Chagas’ disease may be c alled Chagasic
enteropathy and it can occur in the dilated or non-dilated form.
The pathogenesis of dysfunction and dilation of segments of
the digestive tract in Chagas’ disease is based on denervation of the complex network of intramural neurons, today known as enteric nervous system, that controls many of the functions of the digestive
tract2 0 . The destruction of intramural neurons in megaesophagus
and megacolon was identified many years ago5 1 7 and was later
c o n fir m e d b y m e tic ulo us n e ur o n a l c o un ts pe r fo r m e d in megaesophagus and in non-dilated esophagus, in the stomach , in
different parts of the small intestine, in megacolon, and in non-dilated colon of Chagasic patients2 4. Recently, new counts were
done considering the neuronal hypertrophy that occurs in Chagasic
megac olon and the authors found that denervation was greater than 5 5 % in 7 6 .5 % o f c ase s1, c o nfir ming e ar ly studie s b y
Koeberle2 4.
The mec hanisms determining the degenerative lesions of the
neurons and even their c omplete destruc tion in the visc era of
the digestive trac t of Chagasic patients are still inc ompletely understood. They act starting from the acute phase of the disease2 3
but c ontinue during the c hronic phase. It was first proposed
that a neurotoxin released by the parasite near the foc al points
o f infe c tio n dur ing the ac ute phase o f the dise ase was a preponderant determinant of neural injury2 3. The possibility that
the inflammatory proc ess itself may be the c ause of denervation
or that denervation may result from the partic ipation of spec ific c ellular and humoral responses to T. cruzi developed by the
host, including autoimmunity, has been raised since then6 4 9 6 0 6 2 6 4.
However, until now there is no definitive proof that autoimmunity
is the primary c ause of the events oc c urring in c hronic Chagas’
disease and one area of agreement that has emerged in rec ent years is that parasite persistenc e is required for disease6 2. In
situ PCR analysis performed in murine models of Chagas’ disease
has de mo nstr ate a c o r r e latio n b e twe e n the pe r siste nc e o f
parasites and the presenc e of disease in musc le tissue7 1 . The
observation that T. cruzi infec tion c an be re a ctiva te d in patients
with therapeutic or pathologic al immunosuppression also favors
the point of view that c hronic Chagas’ disease is a parasite-induc ed disorder6 4.
I n th i s p r e s e n ta ti o n , Ch a ga s i c e n te r o p a th y wi l l b e
a p p r o a c h e d fr o m th e vi e wp o i n t o f i n vo l ve m e n t o f th e duo de num, j e j unum and ile um alo ne o r in c o mb inatio n, due
to Chagas’ disease in the c hr o nic phase. Chagasic enter o pathy
is muc h le ss fr e que nt and le ss studie d than e so phage al and
c o lo n dise ase o f the same e tio lo gy. Ho we ve r, studie s o n this type o f dise ase ar e impo r tant to e xpand k no wle dge ab o ut the
dige stive fo r m o f Chagas’ dise ase , to inc lude it amo ng the
c ause s o f the inte stinal pse udo -o b str uc tio n syndr o me and o f
b ac te r ial o ve r gr o wth in the small inte stine , and mainly fo r ade quate diagno sis and tr e atme nt.
STRUCTURAL CHANGES
Small bowel dysfunc tion and dilation are mainly due to the
lesions and destruc tion of neurons of the enteric nervous system
in the invo lved visc era. In experimentally infec ted animals,
denervation of the submuc osal and myenteric plexuses of the small b o we l has b e e n c o nfir me d3 4 4 2. The same o c c ur s in
n a tu r a lly in fe c te d c a ts a n d do gs2 6. Th e p e r c e n ta ge s o f
denervation shown in Table 1 were detec ted in humans with
the c hronic phase of Chagas’ disease and with no dilation of any segment of the small bowel. In c ases of enteric m e ga s,
denervation is likely to reac h muc h higher perc entages, as also
o b ser ved in megaeso phagus and megac o lo n. The c o mplete
disappearanc e of intramural neurons has been doc umented in c ases of megaduodenum5 2.
Ta ble 1 - Percent reductio n in the num ber o f neuro ns o f the enteric nervo us system o f the sm a ll bo wel o f pa tients with chro nic Cha ga s’ disea se.
Submucosal plexus ( %) Myenteric plexus ( %)
Duodenum1 3 50 50
Jejunum4 33 36
Ileum1 4
42 51
As a consequence of denervation, the duodenum becomes
hypersensitive to cholinergic agents. Intraluminal application of
acetylcholine in the proximal small intestine provokes more intense
and more prolonged motor activity than in normal individuals3 6.
This type of response to acetylcholine or to one of its analogues
can be a way to demonstrate intramural denervation. The Mecholyl
( metacholine) test performed with manometric monitoring of the
duodenum showed hyperac tive reac tions in 7 0 % of Chagasic
patients with megaesophagus, as opposed to only 1 0 % of Chagasic
patients without m e ga s, demonstrating that duodenopathy is more
frequent in patients with clear involvement of other segments of
the digestive tube by the disease5 7.
Elec tron mic rosc opy reveled that the neuronal lesions of
the jejunum are less intense than those of the megaesophagus
or megac olon and that the remaining c ells show ultrastruc tural
lesio ns6 1. The least damaged c ells sho w an inc r ease in the
n um b e r a n d vo lum e o f o s m o ph ilic gr a n ule s s ugge s tin g
hyper sec r etio n o f neur o tr ansmitter s, per haps r eflec ting the
c omplexity of the disorder of neuroregulation of the func tions
interstitial fibrosis in smooth musc le has also been rec orded6 1.
Hypertrophy of the c irc ular and longitudinal musc ulatur e has b e e n de te c te d in the duo de num5 2 .
The final result of denervation of the enteric nervous system
determined by Chagas’ disease is dilation of the involved organ,
the most expressive manifestation of the digestive form of the
disease. Koeberle2 3 proposed that, as a consequence of damage to
intramural innervation, motor unc oordination of the involved
visceral organ occurs, followed by delayed transit of its content,
stagnation and retention, continuous distention of muscle fibers
whic h bec ome hypertrophied, and finally dilation m e ga. He considered the functional status of the visceral organ to be an
important factor in the determination of the m e ga. According to
the cited author, the m e ga will develop only if the functional activity
of the visceral organ is continuously required. He proposed that dilation of the esophagus and colon occurs more frequently than
dilation of other viscera of the digestive tube because more demands
are made on these organs since, in contrast to other segments and
espec ially the small bowel, they work with solid material. He considered the presence of a defect in sphincter function to be an
impo r tant fac to r in the de ve lo pme nt o f the m e ga, as is the
c ase fo r megaesophagus, but not an essential one, c iting the
megaduodenum and megajejunum as proof. He also stated that the degree of denervation and of the corresponding functional
disorder may affec t the duration of the time needed for the
development of the m e ga. However, other fac tors have been
considered to participate in the pathogenesis of the m e ga s6 0. The
detection of m e ga s in the small bowel is not frequent, but the
megaduodenum is considered to be the segment of the digestive
tube that is most often found to be dilated after the colon and
esophagus; in most cases the dilation is restricted to the duodenal cap. In a series of 8 0 0 autopsies, 1 8 5 cases of megacolon, 1 5 8 of
m e gae so phagus and o nly 2 0 o f m e gaduo de num and 4 o f
megajejunum were detected2 4. Dilation of the ileum is extremely
rare5 9 . Dilation of the segments of the small bowel is frequently
associated with megaesophagus and/or megacolon5 2 5 7. When a
r a dio lo gic a l m e th o d is us e d, h o we ve r, th e in c ide n c e o f
megaduodenum increases. Fonseca1 8 detected dilation of the first
portion of the duodenum in 3 0 % of cases of megaesophagus.
PATHOPHYSIOLOGY
Mo tility. The func tion most c onsistently found to be altered
in Chagasic enteropathy is motor ac tivity, whic h greatly depends
on the regulatory ac tivity of the enteric nervous system. Although dilation of the duodenum, jejunum and ileum is not frequent,
the motor impairment of segments of the small bowel is high
in the digestive form of Chagas’ disease. Radiologic al studies
performed many years ago revealed a high inc idenc e of c hanges
in tonus and transit time in the duodenum, jejunum and ileum
of patients with megaesophagus1 8 6 5 . Manometry of the proximal
small bowel of Chagasic patients has also revealed frequent
mo tility ab no r malities b o th under fasting and po stpr andial
c o nditio ns, espec ially in tho se with megaeso phagus and/o r
megac olon3 5 4 5 4 6. This fac t agrees with the high prevalenc e of a
positive denervation test ( Mec holyl) found in the small bowel
of patients with Chagasic megaesophagus5 7.
Normally, during fasting the small intestine presents successive
cycles of motor activity known as migrant motor complex ( MMC) . At intervals of 8 0 to 1 2 0 minutes a set of repeated contractions of
frequency identical to the basic electric rhythm ( BER) ( 1 2 /min)
occurs in the duodenum. These contractions cover a segment of
about 2 5 cm and migrate in a caudal direction, and their frequency is progressively reduc ed, reac hing 7 -8 /min in the ileum. The
ve lo c ity o f m igr atio n o f the se t o f c o ntr ac tio ns is ab o ut 6 to
8 c m /m in in the duodenum-proximal jejunum. The duration of
the sequence of contractions at the recording point is about 5 min in the proximal jejunum. This type of motor activity is phase 3 of
the MMC and is followed by phase 1 , c harac terized by motor
quiescence and refractoriness, which lasts 1 5 to 6 0 minutes. The
motor activity then reappears gradually in the form of distinct period of intermittent and apparently irregular phasic contractions ( phase
2 ) until it culminates in a new phase 3 . The motor activity of the
interdigestive period has been proposed to be important to lead to
the colon non-absorbed food remains, secretions and cell detritus which, if retained, would favor excessive bacterial proliferation.
The patte r n o f c o ntr ac tio ns that c har ac te r ize s the MMC is
immediately interrupted by food ingestion, with the occurrence of
a motor activity comparable to phase 2 of the MMC and called postprandial or fe d pattern. The duration of MMC interruption by
a meal depends on the composition and the physical properties of
the food ingested1 2; fe d pattern duration of about 1 8 0 , 3 6 0 and
4 1 0 minutes occur in healthy individuals after meals of 6 3 0 , 1 ,2 6 0 and 2 ,5 0 0 kJ, respectively2 2.
A clear manometric abnormality detected in the proximal small
bowel of fasting Chagasic patients is the reduction in the velocity
of propagation of phase 3 ( Figure 1 ) . The calculated length of the
intestinal segment in phase 3 was lower than normal and duration of phase 3 was also shown to be longer in the jejunum but not in
the duodenum, in comparison to normal. These alterations mainly
occurred among patients with megaesophagus and/or megacolon.
These alterations of the phase 3 of the MMC observed in the
manometric recordings of fasting motility of the small intestine of Chagasic patients are detailed in Table 24 6.
Ta ble 2 - So m e cha ra cteristics o f pha se 3 o f the MMC o bserved by sm a ll intestine m a no m etry o f fa sting pa tients with Cha ga s’ disea se with a nd witho ut digestive pa tho lo gy46.
Phase 3 of MMC Controls subjects Chagas’ disease patients
Velocity of propagation 9 .4 ( 6 .1 - 2 4 .0 ) all 4 .7 ( 1 .6 - 1 8 .0 ) *
( cm/min) wit m e ga 4 .5 ( 1 .6 - 1 5 .0 ) * *
no m e ga 7 .9 ( 6 .0 - 1 8 .0 )
Calculated length ( cm) 4 2 .4 ( 2 9 .6 - 7 8 .4 ) all 2 9 .8 ( 1 1 .7 - 8 9 .2 ) * * *
with m e ga 2 7 .8 ( 1 1 .7 - 8 9 .2 ) * * *
no m e ga 4 7 .5 ( 2 6 .6 - 5 4 .8 )
Duration ( min)
Duodenum 4 .6 ( 1 .8 - 7 .0 ) all 5 .6 ( 3 .8 - 1 2 .3 )
Jejunum 4 .4 ( 3 .1 - 5 .6 ) all 6 .5 ( 3 .0 - 2 2 .3 ) * * * * *
* P< 0 .0 0 1 compared with controls. * * P< 0 .0 2 compared with patients without m ega and P > 0 .0 0 2 compared with controls. * * * P< 0 .0 3 compared with controls.
* * * * P< 0.05 compared with patients without m ega and P > 0.02 compared with controls. * * * * * P< 0 .0 0 4 compared with controls.
The frequency of contraction during the activity fronts is normal
in Chagas’ disease4 6. Considering that when an activity front reaches
a segment of the small bowel its mechanical contraction has the same rate as the basic electric rhythm ( BER) of the segment1 1, it
may be concluded that the small intestinal BER is essentially normal
in Chagas’ disease even in patients with the above mentioned
fasting motor abnormalities of this organ.
Another remarkable c hange observed in the motor ac tivity of the small intestine of Chagasic patients is the non-interruption
of the MMC by the ingestion of a meal of approximately 5 3 0 kc al
( Figures 2 and 3 ) , whic h exc lusively oc c urs in patients with
megaduodenum and/or megajejunum3 5, or an attenuation of
the responses to the meal revealed by prolonged manometry
of the small bowel4 5.
Fi gu re 2 - Re c o rd i n gs o f d u o d e n a l a n d je ju n u m m o ti li ty a ro u n d 3 0 m i n u te s a f te r th e e n d o f i n ge sti o n o f a 5 3 0 k c a l m e a l. Di sta n c e b e tw e e n th e p o i n ts o f re c o rd i n gs: 3 0 c m . Wh i le th e c o n tro l p a ti e n t (A) sh o ws a c h a ra c te ri sti c f e d p a tte rn , th e p a ti e n t wi th Ch a ga si c e n te r o p a th y (B) s h o w s a typ i c a l p h a s e 3 o f th e f a s ti n g s ta te , i n d i c a ti n g th a t f e e d i n g d o e s n o t d i s r u p t th e s m a ll i n te s ti n e i n te rd i ge sti ve m o to r p a tte rn .
Fi gu re 3 - Co n d e n se d p re se n ta ti o n o f m a n o m e tri c tra c i n gs f o r th e je ju n u m o f a n o rm a l p e rso n (A) a n d o f a p a ti e n t wi th Ch a ga si c m e ga je ju n u m (B) o ve r a p e ri o d o f a p p ro x i m a te ly 3 3 0 m i n u te s d u ri n g wh i c h a m e a l wa s c o n su m e d . Th e tra c i n g f o r th e n o rm a l je ju n u m sh o ws th a t b e f o re th e m e a l th e re we re f o u r p e ri o d s d u ri n g wh i c h m o to r a c ti vi ty re a c h e d a f re q u e n c y o f 1 2 wa ve s /m i n ( th e sa m e a s f o r BER) wh i c h c o rre sp o n d to p h a se 3 o f MMC. Am o n g th e 3 p h a se s, p h a se 1 i s i d e n ti f i e d b y q u i e sc e n c e a n d p h a se 2 b y a c ti vi ty o f m e d i u m i n te n si ty. Af te r th e m e a l, th e i n te rd i ge sti ve p a tte rn i s re p la c e d b y i n te n se a c ti vi ty d e vo i d o f th e c yc li c c o n f i gu ra ti o n o f th e i n te rd i ge sti ve p e ri o d . Th e tra c i n g o b ta i n e d f o r th e p a ti e n t wi th m e ga je ju n u m sh o ws th a t i n ge sti o n o f th e m e a l d i d n o t i n te rru p t th e MMC, si n c e a sh o rt p e ri o d o f q u i e sc e n c e a f te r th e m e a l w a s f o llo w e d b y a se t o f c o n tra c ti o n s o c c u rri n g a t a f re q u e n c y o f 1 2 w a ve s/m i n , typ i c a l o f p h a se 3 o f MMC4 9.
Co nside r ing that Chagas’ dise ase may b e se e n as a natur al
h u m a n m o d e l o f d e n e r va te d d i ge s ti ve vi s c e r a3 3, th e s e
mano me tr ic findings pe r mit a sugge stio n o f a physio lo gic al natur e: the integr ity o f the enter ic ner vo us system in the small
inte stine is ne c e ssar y fo r the no r mal migr atio n o f the MMC
as we ll as fo r its inte r r uptio n b y fo o d inge stio n.
Ga s tr ic e m ptyin g o f liq uids is dis tur b e d in Ch a ga s ic
patie nts with a c le ar c o mpr o mise o f the duo de num. Gastr ic e m ptying o f an iso to nic de xtr o se so lutio n studie d b y the
sc intigr aphic metho d sho wed that the ear ly phase o f emptying
in a gr o up o f patie nts with me gaduo de num is ab no r mally
ac c e le r ate d in c o mpar iso n with patie nts with Chagas’ dise ase b ut witho ut me gaduo de num and with he althy vo lunte e r s. An
inc r e ase d duo de nal r e c e ptivity is suppo se d to b e the c ause
o f this ab no r mality6 8.
Tr ansit time studie s using sc intigr aphy me tho ds and a
c o nventio nal H
2 breath tec hnique were perfo rmed in Chagasic
patie nts with at le ast o ne manife statio n o f the dige stive fo r m
o f the dise ase , b ut with no signific ant r e te ntio n o f liquids in
the e so phagus. The se studie s sho we d a de laye d ar r ival o f the
te st me al to the c e c um asso c iate d with slo w tr ansit in the
distal small b o we l6 9.
The c hanges in small bowel motility c aused by intramural
denervation may create conditions that favor bacterial proliferation
due to content stagnation. In fact, hyperproliferation of aerobic
bacteria and the presence of anaerobic bacteria in the small bowel
have been documented in patients with Chagasic megaesophagus
and/or megacolon, with the number of colonies being as high in
some cases as those occurring in patients with the clinical syndrome
participation of changes in gastric secretion was excluded, the abnormality was attributed to disorders of loc al motility3 0. In
support of this hypothesis, it was observed that two cases of Chagasic megajejunum with clearly detectable alterations upon manometry
and with c onfirmed bac terial overgrowth in the small bowel
developed the typical clinical syndrome of bacterial overgrowth ( chronic diarrhea, evidence of malabsorption and improvement
with antibacterial treatment)9. The accumulation of fecal material
in the dilated colon can facilitate bacterial proliferation in the small
bowel, as suggested by the observation that surgical removal of
the megac o lo n c auses a dec r ease in the pr o ximal j ej unum microflora in 8 3 % of the patients5 1.
Abso rptio n. This function has not been extensively studied in
Chagas’ disease. It was first observed that Chagasic patients,
especially those with clear involvement of the digestive tube as revealed by megaesophagus or megacolon, presented abnormal
responses to the oral glucose tolerance test ( GTT)5 5, and to the
galactose3 9 and xylose4 1 overload test. The abnormal response to
an oral overload with these monosaccharides was characterized by a high peak of their concentration in blood 3 0 minutes after
ingestion, followed by a rapid fall. Abnormal GTT curves were detected in about 6 5 % of patients with digestive tube m e ga s3 2. On
the other hand, the responses to an intravenous glucose overload did not differ between Chagasic patients and controls4 0. These facts
suggest that rapid monosac c haride absorption may oc c ur in Chagas’ disease, explaining the abnormalities observed when an overload of these substanc es was administered orally. Another
possibility c ould be that the rapid gastric emptying of the test solution immediately after ingestion may expose the proximal small
bowel to an excessive amount of monosaccharide, forcing rapid absorption. Favoring this hypothesis, it was demonstrated that an
accelerated emptying of the liquid contained in the gastric cavity oc c urs probably due to the loss of the ability of the Chagasic stomach to accommodate to distention4 8.
I n o r de r to te st dir e c tly the a b so r ptio n a b ility o f the
pr o ximal small b o we l o f Chagasic patie nts, the me tho d o f
c o ntinuo us inte stinal pe r fusio n with an indic ato r o f var iatio n
in dilutio n was use d. Gluc o se so lutio ns o f fo ur diffe r e nt
in c r e a s in g c o n c e n tr a tio n s ( 0 . 5 , 1 . 0 , 2 . 5 , a n d 5 % ) we r e
infused at a c onstant flow through a tube plac ed in the distal
duodenum or proximal jejunum over a standardized period of
time, and samples were collected 3 0 cm downstream from the point
of infusion. One percent polyethylene glycol ( PEG 4 0 0 0 ) was added
to the infused glucose solution. PEG determination in each distal
sam ple was ne c e ssar y to c o r r e c t the var iatio n o f gluc o se
concentration due to glucose dilution occurring along the chosen
intestinal segment. This method permitted an estimate of the
amount of glucose absorbed between the point of infusion and the
point of aspiration. Considering that gluc ose absorption is a
function of its concentration in the solution in contact with the
muc osa until reac hing a saturation point ( Mic haelis-Menten
kynetics)2 1, the data obtained were used to study the kinetics of
glucose absorption and to construct a dose-response type of curve.
The intestinal segment under study in Chagasic patients with an
abnormal GTT was found to show kinetic characteristics indicating
a greater capacity for glucose transport ( greater Vmax) , but less
affinity ( greater Km) than controls ( Figure 4 )3 6 3 7 . The curves in
Figure 4 were drawn by plotting the c orresponding values of
perfused glucose ( g/min) and absorption velocity ( g/3 0 cm/min) c alc ulated from the regression line equations. These c urves
demonstrate that for a given amount of glucose in the intestine,
Fi gu re 4 - Re la ti o n b e twe e n glu c o se a b so rpti o n ra te s a n d glu c o se c o n c e n tra ti o n s i n the pe rf u se d so lu ti o n i n the sm a ll b o we l. The se c urve s we re c a lc ula te d fro m the re gre ssio n line e q ua tio ns. The ve rtic a l do tte d lin e s m a rk the lim its o f the glu c o se c o n c e n tra tio n e n c o u n te re d i n the du o de n u m du ri n g the i n i ti a l pha se s o f the GTT36 37.
when the glucose administered is above 0 .2 5 g/min, the transfer of
sugar to the blood is greater in Chagasics than in controls. During
the first 3 0 minutes of the GTT the fluid c ollec ted through a duodenal probe has a glucose concentration from 7 to 1 1 g/1 0 0 ml.
In Figure 4 these values were situated between the two vertical
dotted lines which enclose a region where the curves show a clear
differenc e in absorption rate between Chagasic s and c ontrol individuals. Thus, an epithelium with a greater absorption capacity
permitting monosaccharide hyperabsorption may explain, at least
in part, the abnormal GTT of Chagasic patients. It has been proposed
that this dysfunction in glucose absorption may be determined by the intramural denervation of the small bowel demonstrated in
Chagas’ disease3 2 3 8. Also we may assume that the accelerated gastric
emptying of a glucose solution observed in Chagasic patients4 8 may
have an adaptive action in their intestinal absorptive epithelium inducing a high capacity to absorb in order to avoid the undesirable
effect of a high osmolarity in the lumen of the small intestine by a
local high carb o hydr ate c o nc e ntr atio n.
The 1 3 1I o le ic ac id te st use d at the time to study lipid
ab so r ptio n sho we d lo w r adio ac tivity c ur ve s in b lo o d afte r ingestio n in 3 0 % o f the Chagasic patients studied. Co nsidering
that mo st o f the se patie nts sho we d no r mal gastr ic e mptying
as e valuate d b y a r adio lo gic al me tho d, it was c o nc lude d that
the dise ase may c ause a slo w lipid ab so r ptio n b ut witho ut affe c ting the to tal amo unt ab so r b e d sinc e fe c al r adio ac tivity
wa s n o r m a l3 7. I n te s tin a l a b s o r ptio n wa s la te r s tudie d in
Chagasic patie nts b y the intr aj e j unal administr atio n o f 1 3 1I
o le ic ac id. Sinc e no diffe r e nc e s in r e sults we r e o b se r ve d b etween Chagasic patients and c o ntr o ls, it was c o nc luded that
the ab no r malitie s o b se r ve d in the o r al te st we r e pr o b ab ly
due to de laye d gastr ic e mptying o f the te st me al inge ste d4 7.
Se c re ti o n . The muc o sa o f the small b o we l c o ntains c e lls
r e gulato r y ac tio ns b o th lo c ally and at a distanc e . Intr amur al
denervatio n wo uld be expec ted to have so me effec t o n this
secretion. However, it was observed that Chagasic patients with
clear impairment of the digestive tract shown by megaesophagus
did not present any abnormality in motilin, enteroglucagon or
gastric inhibitor peptide levels either under basal conditions or
after stimulation by an oral or intravenous glucose overload or by
insulin hypoglyc emia2 7. In another study on this same type of
patients, no changes in cholecystokinin, motilin or enteroglucagon
levels wer e detec ted in the basal state o r after intr aveno us
administr atio n o f sec r etin asso c iated o r no t with duo denal
instillation of phenylalanine4 3.
Im m une functio n. It is known that one of the targets of the
e n te r ic n e r vo us s ys te m a r e th e im m un o m o dula to r y a n d
inflammatory c ells of the gut2 0. However, there are only a few
publications about the relationship between the involvement of
the digestive tube by Chagas’ disease and the immune system of
the inte stine . Spe c ific IgA antib o dy c lasse s we r e de te c te d
predominantly in patients with the digestive form of the disease
( 9 2 %) in contrast with 2 0 % of patients with the cardiac form and
2 1 .4 % of patients with the indeterminate form5 0. Elevation of serum
IgA levels in Chagas’ disease was observed only in patients with
concomitant dilation of the esophagus and colon while Chagasic
patients with the cardiac or indeterminate forms of the disease did
not show this abnormality7. Considering that the small bowel has
the greater c onc entration of IgA-produc ing c ells in the entire
digestive tract, it was supposed that the Chagasic patients with
megaesophagus and megacolon could also have an involvement
of the small intestine which would be the responsible for the higher
serum IgA levels observed7. Patients with Chagasic enteropathy,
defined by organ dilatation or motor abnormality, presented higher
serum IgA levels than patients without enteropathy8. Secretory IgA
in the intestinal aspirate showed concentrations above the levels
described for normal control individuals referred to in literature;
however, there were no differences when the results of patients
with Chagasic enteropathy were compared to those of patients who
did not present enteropathy8.
CLINICAL MANIFESTATIONS AND DIAGNOSIS
The c linic al manifestatio ns o f Chagasic enter o pathy o c c ur
afte r the de ve lo pme nt o f dilatatio n o f o ne o r mo r e o f the
anato mic al se gme nts o f the small b o we l, The y ar e almo st
a l wa ys a s s o c i a te d wi th c o n c o m i ta n t s ym p to m s o f
m e gae so phagus and/o r m e gac o lo n. The pr e se nc e o f o nly
mo to r o r abso rptive dysfunc tio n o f the small bo wel, detec table
b y spe c ial te sts, do e s no t se e m to b e suffic ie nt to pr o vo k e
sympto ms o r signs o f signific anc e to the patie nt. The r e is no
systematic desc r iptio n o f the manifestatio ns o f Chagasic small
bowel m e ga s. Investigators of the digestive form of Chagas’
disease have reported only few personally observed c ases5 3 5 7 6 7.
Par tic ular ly o utstanding in this r e spe c t is the r e po r t b y Raia
e t al5 2 o f 1 1 c ase s o f me gaduo de num.
The r e is a wide gamut o f c linic al e xpr e ssio ns o f e c tatic
Chagasic enter o pathy, r anging fr o m the ab senc e o f sympto ms, with de te c tio n o nly b y r adio lo gic al e xaminatio n indic ate d fo r
o the r pur po se s, to signs and sympto ms b e lo nging to at le ast
thr e e type s o f syndr o m e s: dyspe ptic syndr o m e , inte stinal
ps e udo - o b s tr uc tio n s yn dr o m e , a n d b a c te r ia l o ve r gr o wth syndr o me o f the small b o we l. It may b e state d that c linic al
manife statio ns te nd to b e mo r e e xpr e ssive and se ve r e the
gr e ate r the e xte nt o f dilatio n o f the small b o we l.
Within the dyspeptic picture, patients with m e ga s of the small
bowel may present a sensation of postprandial fullness and
discomfort in the epigastrium5 7 6 7. Pain, which is not always present,
may vary in intensity and type and may occur during the early or
late postprandial period. Raia et al5 2 5 3 pointed out that the clinical
pic ture of megaduodenum c an be that of gastric stasis of a
progressive nature, characterized by vomiting of food ingested many
hours before, dehydration, epigastric pain and visible gastric
peristalsis, and lesions of the duodenal and gastric mucosa, and
includes the possibility of bleeding and even stomach rupture.
Another important c omplic ation is represented by esophageal mucosa injuries due to prolonged contact with material stagnating
in the stomach, with reflux into the esophagus. In a case observed
by us, reflux disease was present in a particularly severe form
since it was facilitated by a previous surgical intervention in the
c ar dia fo r the tr e atm e nt o f m e gae so phagus. I t sho uld b e
remembered that gastric stasis in the absenc e of small bowel
dilation in Chagasic patients may be due to gastropathy of the same
etiology5 3 7 0. As previously mentioned, cases of megajejunum are
rare. In the few c ases we observed, the c ondition was always
assoc iated with megaduodenum. Megajejunum has also been
reported to occur separately or associated with megaileum5 3 5 7 6 7.
Patients with megajejunum may be asymptomatic or may
present well defined clinical signs and symptoms such as intestinal
pseudo-obstruc tion assoc iated or not with syndrome of bac terial
o ve r gr o wth in the small b o we l. Ab do minal diste ntio n, the
presenc e of c ontinuous pain or of c ramps, the visible peristalsis,
the intestinal c onstipation and the detec tion of fluid levels in
small bo wel lo o ps by simple abdo minal radio graphy in the
orthostatic position are the elements c omposing the pic ture of
pseudo-obstruc tion of the small bowel.
The o c c ur r e nc e o f c o ntinuo us c hr o nic diar r he a o r o f
diar r he a alte r nating with pe r io ds o f inte stinal c o nstipatio n
o r o ther sympto ms o f pseudo -o bstruc tio n suggests a diagno sis
o f b ac te r ial o ve r gr o wth in the small b o we l. This hypo the sis
is reinforced when there is evidence of intestinal malabsorption
such as weight loss and clinical and laboratory signs of steatorrhea,
anemia or hypocalcemia. The diagnosis of bacterial overgrowth
may be c onfirmed by the demonstration of stric tly anaerobic
bacteria in the upper portions of the small bowel, where they are
not normally found, or by the increased number of colonies in
duodenal aspirates9 6 6 67. The hydrogen breath test may also indicate
the presence of bacterial overgrowth9 2 9 5 1 6 6 6 7. The presence of a
high hydrogen rate in expired air when the patient is still fasting
also indicates the syndrome of bacterial overgrowth of the small
improvement of the patient with antibiotic treatment may be
considered to be a positive diagnostic test for the syndrome9.
The patient with megaileum described by Santos et al59 presented
chronic diarrhea, abdominal distention and signs and symptoms of
intestinal subocclusion resolved by clinical treatment. In summary,
clinical manifestations similar to those of megajejunum.
The diagno sis o f dilatio n o f sm all b o we l se gm e nts due
to Chagas’ dise ase is c o nfir m e d b y standar d r adio lo gic al examination of the duodenum or the entire small bowel. This
examination permits the identific ation of the duodenal c ap or of
other segmental dilations of the duodenum, the megajejunum,
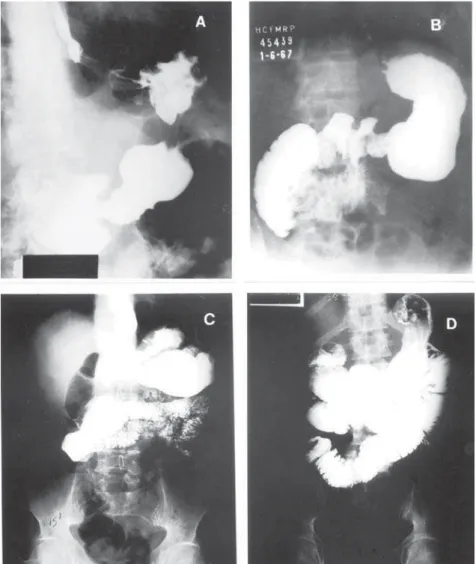
megaileum, and total dilation of the small bowel ( Figure 5 ) . These examinatio ns ar e also useful fo r the o b ligato r y differ ential
diagnosis with organic c auses of intestinal obstruc tion.
Endosc opic examination is indic ated for the diagnosis of
c hanges in the muc osa of the esophagus, stomac h and duodenum
consequent to stasis, which may range from inflammation to ulcer
and bleeding, and may also aid the differential diagnosis with
organic c auses of stomac h and duodenum obstruc tion. It may
also indic ate the diagnosis of megaduodenum.
For an etiologic al diagnosis it is indispensable to c onfirm
serologically the presence of Chagas’ disease by immunofluorescence
or by any other test with good performance.
The diffe r e ntial diagno sis o f dilate d Chagasic e nte r o pathy
c an b e made with a wide var ie ty o f unc o mmo n dise ase s3 1 3 4.
Ho we ve r, the c o nc o mitant me gae so phagus and me gac o lo n
and/o r Chagas he ar t dise ase , e pide m io lo gic al data and a
po sitive se r o lo gic te st c le ar ly po int to the diagno sis.
TREATMENT
Wh e n th e pa tie n t o n ly pr e s e n ts dys pe ptic s ym pto m s ,
tr e atme nt may b e limite d to die tar y adj ustme nts, e spe c ially
with the r e c o mme ndatio n o f b land me als fr e e o f sub stanc e s
that ir r itate the muc o sa, r e duc tio n o f the amo unts o f fatty
fo o ds, me als o f small vo lume , and go o d fo o d mastic atio n.
Altho ugh the e ffic a c y o f pr o k ine tic m e dic a tio ns in the se
patho lo gic al c o nditio ns is unk no wn, the use o f do mpe r ido ne
at habitual do ses c o uld be attempted. In the presenc e o f reflux
e so phagitis, pr o to n pump inhib ito r s ar e indic ate d e ve n fo r
c o ntinuo us use , the same applying to the pr e se nc e o f mar k e d gastr itis o r duo de nitis.
Surgical treatment of megaduodenum is reserved for cases in which stasis is clinically important and consists of duodenojejunal
anastomosis close to the duodenojejunal angle, this being the type of operation most frequently performed by Raia et al5 2 5 3. Rezende57
pointed out that surgical treatment should be indicated only in
c ases in whic h the sympto ms ar e unequivo c ally due to the megaduodenum and not only on the basis of radiological findings. In cases of megajejunum or megaileum, partial enterectomy may be indicated if the respective dilated segments are not extensive5 7.
The operations, however, should be avoided when long segments of the small bowel are dilated. In these cases, clinical treatment of the obstructive episodes should be instituted, with interruption of
o r al fe e ding, c o ntinuo us gastr ic aspir atio n, c o r r e c tio n o f dehydration and of electrolyte disorders and, eventually, the use of total parenteral nutrition5 7 6 7.
B ac ter ial o ver gr o wth syndr o me o f the small b o wel sho uld b e tr e a te d wi th a n ti m i c r o b i a l d r u g s ( te tr a c yc l i n e , c hlo ramphenic o l, c ephalo spo rin, metro nidazo le, etc ) , usually
a t s im ila r o r e ve n lo we r do s e s th a n th o s e us e d fo r th e tr e atme nt o f infe c tio us pr o c e sse s, fo r 3 o r 4 we e k s. B ac te r ial se nsitivity te sts do no t always indic ate the b e st antib io tic fo r
e ac h c ase . Sinc e the mo to r ab no r mality is pe r siste nt, the pe r io dic use o f antimic r o b ial age nts may b e ne c e ssar y. If the pic tur e is no t r e so lve d with a give n antib io tic , indic ating b ac te r ial r e sistanc e , it is ne c e ssar y to switc h to ano the r o ne .
Asso c iate d nutr itio nal diso r de r s due to the malab so r ptio n pr o vo k e d b y b ac te r ial o ve r gr o wth sho uld also b e c o r r e c te d.
Co ns ide r ing tha t pa r a s ite pe r s is te nc e is r e q uir e d fo r dise ase e vo lutio n in the c hr o nic phase , it is suppo se d that a r e duc tio n o f par asitic b ur de n pr o duc e d b y c he mo the r apy o r any o the r pr o c e dur e c o uld e nhanc e anti-T. c ru zi immunity and will b e b e ne fic ial to the patie nt6 2. This hypo the sis le ads
to the sugge stio n that an e ffic ie nt pr e ve ntive me asur e against mo r e se ve r e manife statio ns o f the dise ase , suc h as c ar diac manifestatio ns and dilatio n o f the o r gans o f the digestive tube, c o uld b e ac hie ve d b y c he mo the r apy if indic ate d in the r e c e nt c hro nic phase ( infec tio n ac quired in the last 1 0 years) , mainly in pa tie n ts with th e in de te r m in a te fo r m o f th e dis e a s e . Ho we ve r mo r e e ffic ie nt and le ss to xic dr ugs ar e r e quir e d1 5.
REFERENCES
1 . Adad SJ, Canç ado CG, Etc hebehere RM, Teixeira VP, Gomes UA, Chapadeiro E,
Lopes ER. Neuron c ount reevaluation in the myenteric plexus of c hagasic
megac olon after morphometric neuron analysis. Virc hows Arc hive s 4 3 8 : 2 5 4
-2 5 8 , -2 0 0 1 .
2 . Alc â n ta r a FG, Co s ta RB . J e j un o pa tia c h a gá s ic a . Re vis ta B r a s ile ir a de
Me dic ina 2 3 : 3 1 6 - 3 1 7 , 1 9 6 6 .
3 . Alc ântar a FG, Olive ir a J AM. De str uiç ão ne ur o nal no ple xo de Aue r b ac h
e m r ato s c hagásic o s c r ô nic o s. Re vista do Instituto de Me dic ina Tr o pic al
de São Paulo 6 : 2 0 7 - 2 1 0 , 1 9 6 4 .
4 . Alc ântar a FG, Olive ir a J AM. Fase c r ô nic a da mo lé stia de Chagas no r ato
Wistar. Pe squisas quantitativas do s ne ur ô nio s no ple xo de Me issne r. Re vista
do Instituto de Me dic ina Tr o pic al de São Paulo 6 : 2 0 4 - 2 0 6 , 1 9 6 4 .
5 . Amo r im M, Co r r e a Ne tto A. Histo pato lo gia e pato ge ne se do me gae so fago e me gar r e to ( Co nside r aç õ e s e m to r no de um c aso de “Mal de e ngasgo ”) . Annae s da Fac uldade de Me dic ina de São Paulo 8 : 1 0 1 - 1 2 7 , 1 9 3 2 .
6 . Andr ade SG, Andr ade ZA. Do e nç a de Chagas e alte r aç õ e s ne ur o nais no ple xo de Aue r b ac h. Re vista do Instituto de Me dic ina Tr o pic al de São Paulo 8 : 2 1 9 - 2 1 4 , 1 9 6 6 .
7 . Andr ade - Sá NM. De te r minaç ão do s níve is sé r ic o s de imuno glo b ulina da c lasse IgA e m pac ie nte s c o m as dife r e nte s fo r mas c línic as da fase c r ô nic a da do e nç a de Chagas. Re vista de Pato lo gia Tr o pic al 2 7 : 1 0 7 - 1 5 2 , 1 9 9 8 .
8 . An dr a de - Sá NM. I gA s é r ic a e I gA s e c r e tó r ia in te s tin a l n a e n te r o pa tia c hagásic a. Te se de do uto r ado . Unive r sidade de São Paulo , Fac uldade de Me dic ina de Rib e ir ão Pr e to , Rib e ir ão Pr e to , 2 0 0 3 .
9 . Apr ile LR O, Me n e gh e lli UG. Sín dr o m e do s upe r c r e s c im e n to b a c te r ia n o n o i n t e s t i n o d e l g a d o n o m e g a j e j u n u m c h a g á s i c o . Ar q u i vo s d e Gastr o e nte r o lo gia de São Paulo 3 2 : 7 1 - 7 8 , 1 9 9 5 .
1 0 . Chagas C. No va e ntidade mo r b ida do ho me m. Re sumo ge r al de e studo s etiolojic os e c linic os. Memórias do Instituto Oswaldo Cruz 3 : 2 1 9 -2 7 5 , 1 9 1 1 .
1 1 . Chr iste nse n J , Sc he dl HP, Clifto n J A. The small inte stine b asic e le c tr ic al r hythm ( B ER) in man. Gastr o e nte r o lo gy 4 6 : 7 7 3 - 7 7 4 , 1 9 6 4 .
1 2 . Co h e n S , S n a p e J r WJ . Mo ve m e n t o f th e s m a l l a n d l a r ge i n te s ti n e . I n: Sle ise nge r MH, Fo r dtr an JS ( e ds) Gastr o inte stinal Dise ase s, 4th e ditio n,
WB Saunde r s Co . Fo ur th e ditio n, Philade lphia ( USA) , p. 1 0 8 8 -1 1 0 5 , 1 9 8 9 .
1 3 . Co sta RB , Alc ântar a FG. Duo de no patia c hagásic a. Re vista B r asile ir a de Me dic ina 2 3 : 1 5 8 - 1 6 0 , 1 9 6 6 .
1 4 . Co sta RB , Alc ântar a FG. Ple xo s sub muc o so e mio e nté r ic o do íle o humano na mo lé stia de Chagas. Re vista B r asile ir a de Me dic ina 2 3 : 3 9 9 - 4 0 0 , 1 9 6 6 .
1 5 . Co ur a JR, Castr o SL. A c r itic al r e vie w o n Chagas dise ase c he mo the r apy. Me mó r ias do Instituto Oswaldo Cr uz 9 7 : 3 - 2 4 , 2 0 0 2 .
1 6 . Dias J CP. The inde te r minate fo r m o f human c hr o nic Chagas’ dise ase : a c lin ic a l e pide m io lo gic a l r e vie w. R e vis ta da So c ie da de B r a s ile ir a de Me dic ina Tr o pic al 2 2 : 1 4 7 - 1 5 6 . 1 9 8 9 .
1 7 . Etze l E. Ne ur o pato lo gia do me gae so fago e me gac o lo . Annae s da Fac uldade de Me dic ina de São Paulo 1 0 : 3 8 3 - 3 9 5 , 1 9 3 4 .
1 8 . Fo nse c a LC. Se mio lo gia r adio ló gic a da disc ine sia func io nal do duo de no . Ar q uivo s de Cir ur gia Clínic a e Expe r ime ntal 1 5 : 1 7 6 - 2 0 0 , 1 9 5 2 .
1 9 . Fr e itas J LP. Co ntr ib uiç ão par a o e studo do diagnó stic o da m o lé stia de Chagas po r pr o c e sso s de lab o r ató r io . Te se de do uto r ado . Unive r sidade de
São Paulo , São Paulo , SP, 1 9 4 7 .
2 0 . Go yal RK, Hir ano I. The e nte r ic ne r vo us syste m. Ne w England J o ur nal o f Me dic ine 3 3 4 ; 1 1 0 6 - 1 1 1 5 , 1 9 9 6 .
2 1 . Ho ldswo r th CD, Dawso n AM. The ab so r ptio n o f mo no sac c har ide s in man. Clinic al Sc ie nc e s 2 7 : 3 7 1 - 3 7 9 , 1 9 6 4 .
2 2 . Ke llo w J E. Ma no m e tr y. In : MM Sc hus te r, MD Cr o we ll, Ko c h KL ( e ds ) Sc huste r Atlas o f Gastr o inte stinal Mo tility in He alth and Dise ase , 2nd editio n,
B C De c k e r Inc , Hamilto n, Canada, pp. 2 1 9 - 3 6 , 2 0 0 2 .
2 3 . Ko e b e r le F. Ente r o me galy and c ar dio me galy in Chagas dise ase . Gut 4 : 3 9 9 -4 0 5 , 1 9 6 3 .
2 4 . Ko e b e r le F. Ch a ga s ’ dis e a s e a n d Ch a ga s ’ s yn dr o m e ; th e pa th o lo gy o f Ame r ic an tr ypano so miasis. Advanc e s in Par asito lo gy 6 : 6 3 - 1 1 6 , 1 9 6 8 .
2 5 . Ko e b e r le F, Nado r E. Etio lo gia e pato ge nia do me gae so phago no B r asil. Re vista Paulista de Me dic ina 4 7 : 6 4 3 - 6 6 1 , 1 9 5 5 .
2 6 . Ko e b e r le GAF. O ple xo mie nté r ic o na mo lé stia de Chagas e m gato s e c ãe s c o m infe c ç ão natur al. Te se de do uto r ado . Unive r sidade de São Paulo , Fac uldade de Me dic ina de Rib e ir ão Pr e to , 1 9 6 3 .
2 7 . Lo ng RG, Alb uq ue r q ue RH, Pr ata A, B ar ne s AJ , Adr ian TE, Chr isto fide s ND, B lo o m SR. Re spo nse o f plasma panc r e atic and gastr o inte stinal ho r mo ne s
to o r al and intr aveno us gluc o se and insulin hypo glyc emia in Chagas’ disease Gut 2 1 : 7 7 2 - 7 7 7 , 1 9 8 0 .
2 8 . Mac edo VO. Fo r ma indeter minada da do enç a de Chagas. In : Dias JCP, Co ur a JR, ( e ds) , Clinic a e Te r apê utic a da do e nç a de Chagas, Edito r a FIOCRUZ,
Rio de j ane ir o , p. 1 3 5 - 1 5 1 , 1 9 9 7 .
2 9 . M a c h a d o WM . S m a l l i n t e s t i n e f l o r a i n c h a g a s i c p a t i e n t s wi t h m e ga e s o p h a gu s a n d/o r m e ga c o l o n : s tu dy u s i n g th e H2 b r e a th te s t.
3 0 . Mac hado WM, Mo r ae s- Filho J PP, Santo s MAA, B e ttar e llo A. J e j unal flo r a o f patie nts with me gao e so phagus se c o ndar y to Chagas’ dise ase . Tr ansac tio ns o f the Ro yal So c ie ty o f Tr o pic al Me dic ine and Hygie ne 8 3 : 1 9 9 - 2 0 1 , 1 9 8 9 .
3 1 . Mann SD, De b insk i HS, Kam m MA. Clinic al c har ac te r istic s o f c hr o nic idio pathic inte stinal pse udo -o b str uc tio n in adults. Gut 4 1 : 6 7 5 -6 8 1 , 1 9 9 7 .
3 2 . Me ne ghe lli UG. Estudo s so b r e a ab so r ç ão inte stinal de glic o se , xilo se e á c ido o lé ic o 1 3 1 I n a fo r m a c r ô n ic a da m o lé s tia de Ch a ga s . Te s e de do uto r ado . Unive r sidade de São Paulo , Fac uldade de Me dic ina de Rib e ir ão Pr e to , Rib e ir ão Pr e to , 1 9 6 9 .
3 3 . Me ne ghe lli UG. Chagas’ dise ase : a mo de l o f de ne r vatio n in the study o f digestive tr ac t mo tility. B r azilian Jo ur nal o f Medic al and B io lo gic al Resear c h 1 8 : 2 5 5 - 2 6 4 , 1 9 8 5 .
3 4 . Me ne ghe lli UG, Apr ile LRO. Distúr b io s mo to r e s do inte stino de lgado . In: Castr o LP, Vaz Co e lho LG ( e ds) Gastr o e nte r o lo gia, Me dsi, Rio de Jane ir o , p. 1 0 4 9 - 1 0 6 8 , 2 0 0 4 .
3 5 . Me ne ghe lli UG, Apr ile LRO, Olive ir a RB , Mar tine lli ALC, Tr o nc o n LEA, Dantas RO. Fe e ding do e s no t disr upt the inte r dige stive mo to r patte r n in c hagasic me gaduo de num and me gaj e j unum. In : Ac ta Gastr o e nte r o lo gic a La ti n o a m e r i c a n a : R e s u m o s d o XXI I I Co n gr e s s o P a n a m e r i c a n o d e Enfe r me dade s Dige stivas, B ue no s Air e s, Ar ge ntina, p4 7 , 1 9 9 3 .
3 6 . Me n e gh e lli UG, Go do y RA, Pa do va n W. Hipe r r e a tivida de do in te s tin o delgado à ac etilc o lina na fo r ma c r ô nic a da mo léstia de Chagas. In : Resumo s
do XX Co ngr e sso B r asile ir o de Gastr o e nte r o lo gia, São Paulo , p. 2 0 , 1 9 6 8 .
3 7 . Me ne ghe lli UG, Iazigi N, Vie ir a CB , Pado van W, Go do y RA. O te ste do ác ido
o lé ic o 1 3 1 I na fo r ma c r ô nic a da mo lé stia de Chagas. Re vista Go iana de Me dic ina 1 8 : 7 5 - 9 0 , 1 9 7 2 .
3 8 . Meneghellli UG, Pado van W, Lima Filho , EC, Go do y RA. Intestinal ab so r ptio n o f gluc o se in c hr o nic Chagas’ dise ase studie d b y the c o ntinuo us pe r fusio n
te c hniq ue . Ar q uivo s de Gastr o e nte r o lo gia de São Paulo 8 : 1 0 9 - 1 1 8 , 1 9 7 1 .
3 9 . Me ne ghe lli UG, Re is LCF. Estudo s so b r e o me tab o lismo do s hidr ato s de c a r b o n o n a m o lé s tia de Ch a ga s . I I I . A pr o va de s o b r e c a r ga o r a l de
galac to se . Re vista da Asso c iaç ão Mé dic a B r asilile ir a 1 3 : 3 - 1 0 , 1 9 6 7 .
4 0 . Me n e gh e lli UG, R e is LCF, Vic h i FL, Lim a Filh o EC. Es tudo s s o b r e o
me tab o lismo de hidr ato s de c ar b o nio na mo lé stia de Chagas. IV. Pr o vas intr ave no sas de to le r ânc ia à glic o se e à to lb utamida. Re vista Paulista de
Me dic ina 7 5 : 2 8 1 - 2 8 8 , 1 9 6 9 .
4 1 . Me ne ghe lli UG, Vie ir a CB , Pado van W, Go do y RA. O te ste da d- xilo se na
mo lé stia de Chagas. Ar q uivo s de Gastr o e nte r o lo gia de São Paulo 8 : 1 9 1 -1 9 8 , -1 9 7 -1 .
4 2 . Me ne ze s H, Olive ir a J SM. A m o tilida de inte stina l ( duo de no ) de r a to s c hagásic o s c r ô nic o s. Re vista B r asile ir a de Me dic ina 2 3 : 7 7 9 -7 8 2 , 1 9 6 6 .
4 3 . M o t t CB , Gu a r i t a D R , S i p a h i AM , B e t t a r e l l o A. Ho r m ô n i o s gastr o e nte r o panc r e átic o s e m po r tado r e s da do e nç a de Chagas c r ô nic a. Re vista do Ho spital das Clínic as da Fac uldade de Me dic ina de São Paulo
4 4 : 6 3 - 7 2 , 1 9 8 9 .
4 4 . Okumur a M, Co r r ea Neto A. Pr o duç ão exper imental de “megas” em animais
ino c ulado s c o m Tr ypano so ma c r uzi. Re vista do Ho spital das Clínic as da Fac uldade de Me dic ina de São Paulo 1 6 : 3 3 8 - 3 4 1 , 1 9 6 1 .
4 5 . Olive ir a RB , Castillo T, Wingate DL, Me ne ghe lli UGl. Chagas dise ase as a
mo de l fo r the ide ntific atio n o f small b o we l mo to r ab no r malitie s in e nte r ic ne ur o pathy. Gastr o e nte r o lo gy 1 0 8 : A5 9 2 , 1 9 9 5 .
4 6 . O l i ve i r a R B , M e n e g h e l l i UG, Go d o y R A, D a n ta s R O , P a d o va n W.
Ab no r malitie s o f inte r dige stive mo tility o f the small inte stine in patie nts with Chagas’ dise ase . Dige stive Dise ase s and Sc ie nc e s 2 8 : 2 9 4 - 2 9 9 , 1 9 8 3 .
4 7 . Olive ir a RB , Me ne ghe lli UG, Pado van W, Dantas RO, Go do y RA. A ab so r ç ão in te s tin a l do á c ido o lê ic o 1 3 1 I a dm in is tr a do po r via in tr a j e j un a l e m c hagásic o s c r ô nic o s. Re vista Go iana de Me dic ina 2 4 : 1 - 1 6 , 1 9 7 8 .
4 8 . Olive ir a RB , Tr o nc o n LEA, Me ne ghe lli UG, Pado van W, Dantas RO, Go do y RA. I m pa ir e d ga s tr ic a c c o m m o da tio n to dis te n s io n a n d r a pid ga s tr ic
e mptying in patie nts with Chagas’ dise ase . Dige stive Dise ase s and Sc ie nc e s 2 5 : 7 9 0 - 7 9 4 , 1 9 8 0 .
4 9 . Pe tr i K, Eise n H. Chagas’ dise ase : a mo de l fo r the study o f auto immune
dise ase s. Par asito lo gy To day 5 : 1 1 1 -1 1 6 , 1 9 8 9 .
5 0 . Pr imave r a KSC, Ume zawa ES, Pe r e s B A, Camar go ME, Ho shino - Shimizu S. Cha ga s ’ dis e a s e : I gA, I gM a nd I gG a ntib o die s to T. c ru z i a m a s tigo te , tr ypo mastigo te and e pimastigo te antige ns in ac ute and diffe r e nt c hr o nic fo r ms o f the dise ase . Re vista do Instituto de Me dic ina Tr o pic al de São Paulo 3 2 : 1 7 2 - 1 8 0 , 1 9 9 0 .
5 1 . Quintanilha AGG, Santo s MAA, Avila- Cam po s MJ , Saad WA, Pino tti HW, Zilb e r ste in B . Cha ga sic m e ga c o lo n a nd pr o xim a l j e j unum m ic r o flo r a . Sc andinavian Jo ur nal o f Gastr o e nte r o lo gy 3 5 : 6 3 2 -6 3 6 , 2 0 0 0 .
5 2 . Raia AA, Ac quarone P, Correa Neto A. Contribuiç ão ao estudo da etiopatogenia do megaduo denum. Revista Go iana de Medic ina 7 : 1 -6 1 , 1 9 6 1 .
5 3 . R a i a AA, Ga m a - R o d r i g u e s J J . M e g a d u o d e n u m . I n : R a i a AA ( e d ) Manife staç õ e s dige stivas da mo lé stia de Chagas, Sar vie r, São Paulo , pp
1 9 1 -2 0 2 , 1 9 8 3 .
5 4 . Rassi A, Re ze nde JM, Do le s J. Caso de do e nç a de Chagas o b se r vado de sde o pe r ío do inic ial da infe c ç ão , c o m apar e c ime nto pr e c o c e de me gae so fago e me gac o lo . Re vista da So c ie dade B r asile ir a de Me dic ina Tr o pic al 2 : 3 0 3 -3 1 5 , 1 9 6 8 .
5 5 . Re is LCF, Olive ir a HL, Vie ir a CB . Cur vas glic ê mic as ano r mais o b se r vadas e m pac ie nte s c o m a fo r ma c r ô nic a da mo lé stia de Chagas. Re vista Go iana de Me dic ina 6 : 1 5 5 - 1 6 5 , 1 9 6 0 .
5 6 . Re ze nde J M. Fo r ma dige stiva da mo lé stia de Chagas. Re vista Go iana de Me dic ina 5 : 1 9 3 - 2 2 7 , 1 9 5 9 .
5 7 . Re ze nde JM. Manife staç õ e s dige stivas da do e nç a de Chagas. In: Dani R, Castr o LP ( e ds) Gastr o e nte r o lo gia Clínic a, 3 ª e diç ão , Guanab ar a-Ko o gan SA, Rio de J ane ir o , p. 1 7 2 9 - 1 7 5 5 , 1 9 9 3 .
5 8 . Rib e ir o ALP, Ro c ha MOC. Fo r m a inde te r m inada da do e nç a de Chagas: c o n s i de r a ç õ e s a c e r c a do di a gn ó s ti c o e do p r o gn ó s ti c o . R e vi s ta da So c ie dade B r asile ir a de Me dic ina Tr o pic al 3 1 : 3 0 1 - 3 1 4 , 1 9 9 8 .
5 9 . Santo s MR, So b r ado J r CW, Damião AOMC, Ro dr igue s J G, Ir ya KK, Pino tti HW, B e ttar e llo A, Mo r ae s Filho J PP. Me gaíle o c hagásic o . De sc r iç ão de um c aso . Re vista do Instituto de Me dic ina Tr o pic al de São Paulo 3 0 : 2 9 3 - 2 9 5 , 1 9 8 8 .
6 0 . Tafur i WL. Pato ge nia do s me gas. In: Castr o LP, Ro c ha PRS, Cunha AS ( e ds) Tó pic o s e m Gastr o e nte r o lo gia 2 . Me dsi, Rio de Jane ir o , p. 1 6 3 -1 7 3 , 1 9 9 1 .
6 1 . Tafur i WL, Mar ia TA, Lo pe s ER. Le sõ e s do ple xo mie nté r ic o do e sô fago , do j ej uno e do c o lo de c hagásic o s c r ô nic o s. Estudo ao mic r o sc ó pio eletr ô nic o . Re vista do Instituto de Me dic ina Tr o pic al de São Paulo 1 3 : 7 6 - 9 1 , 1 9 7 1 .
6 2 . Tar leto n RL. Chagas disease: a r o le fo r auto immunity? Tr ends in Par asito lo gy 1 9 : 4 4 7 - 4 5 1 , 2 0 0 3 .
6 3 . Tar le to n RL, Sun J , Zhang L, Po nstan Ml. De ple tio n o f T- c e ll po pulatio ns r e sults in e xac e r b atio n o f m yo c ar ditis and par asitism in e xpe r im e ntal Chagas’ dise ase . Infe c tio n and Immuno lo gy 6 2 : 1 8 2 0 - 1 8 2 9 , 1 9 9 4 .
6 4 . Tar le to n RL, Zhang L. Chagas dise ase e tio lo gy: auto immunity o r par asite pe r siste nc e ? Par asito lo gy To day 1 5 : 9 4 -9 9 , 1 9 9 9 .
6 5 . To le do PA, Fo nse c a LC. Radio lo gia do inte stino de lgado na ac alásia. O Ho spital 4 4 : 3 1 7 - 3 2 9 , 1 9 5 3 .
6 6 . To sk e s PP. B ac te r ial o ve r gr o wth o f the gastr o inte stinal tr ac t. Advanc e s in Inte r nal Me dic ine 3 8 : 3 8 7 - 4 0 7 , 1 9 9 3 .
6 7 . Tr o nc o n LEA. Do e nç a de Chagas: e nte r o patia. In : Castr o LP, Ro c ha PRS, Cunha AS ( e ds) Tó pic o s e m Gastr o e nte r o lo gia 2 . Me dsi, Rio de J ane ir o , pp. 2 2 9 - 2 4 4 , 1 9 9 1 .
6 8 . Tr o nc o n LEA, Apr ile LR, Olive ir a RB , Iazigi N. Ab no r mally r apid gastr ic e mptying o f an iso smo tic liq uid me al in patie nts with me gaduo de num.
Dige stive Dise ase s and Sc ie nc e s 4 5 : 2 1 4 5 - 2 1 5 0 , 2 0 0 0 .
6 9 . Tr o n c o n LEA, Olive ir a R B , R o m a n e llo LMF, R o s a - e - Silva L, Pin to MC, I a zigi N. Ab no r mal pr o gr e ssio n o f a liq uid me al thr o ugh the sto mac h and
small inte stine in patie nts with Chagas’ dise ase . Dige stive Dise ase s and Sc ie nc e s 3 8 : 1 5 1 1 -1 5 1 7 , 1 9 9 3 .
7 0 . Vie ir a CB , Go do y RA, Me ne ghe lli UG. Gastr o patia c hagásic a c r ô nic a: no vas pe r spe c tivas de diagnó stic o . Re vista da Asso c iaç ão Mé dic a B r asile ir a 1 5 : 3 8 3 -3 8 4 , 1 9 6 9 .