Arq. NeuroPsiquiatr. vol.58 número4
Texto
Imagem

Documentos relacionados
nosocomial pneumonia in critically ill trauma patients.. Risk factors for ICU-acquired pneumonia. Impact of previous antimicrobial therapy on the etiology and outcome
Group V patients had widespread interictal spiking, non-localizatory surface ictal recordings, some electroclinical suggestion of a posterior quadrant seizure onset and normal MRI
We evaluated the frequency of seizure recurrence and its risk factors following complete or partial antiepileptic drug (AED) withdrawal in seizure free patients for at least two
Unilateral EEG findings did not correlate with bet- ter surgical outcome; all 4 patients (9.8%) with bilat- eral EEG findings were seizure-free after surgery. We noted a
We used the chi-square test to analyze the correlation of epilepsy variables (age at seizure onset, epileptic syndrome, type of seizure, seizure frequency, period without
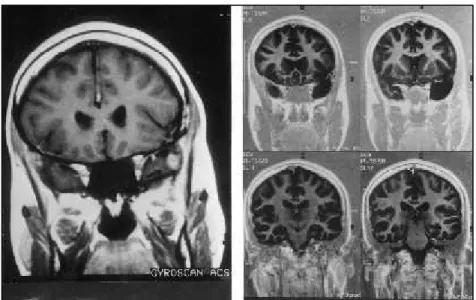
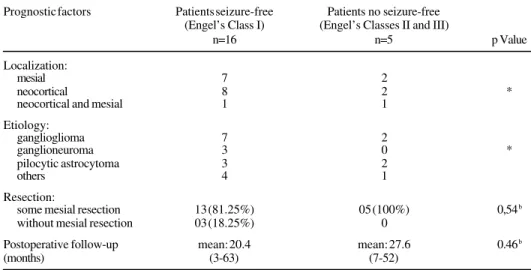
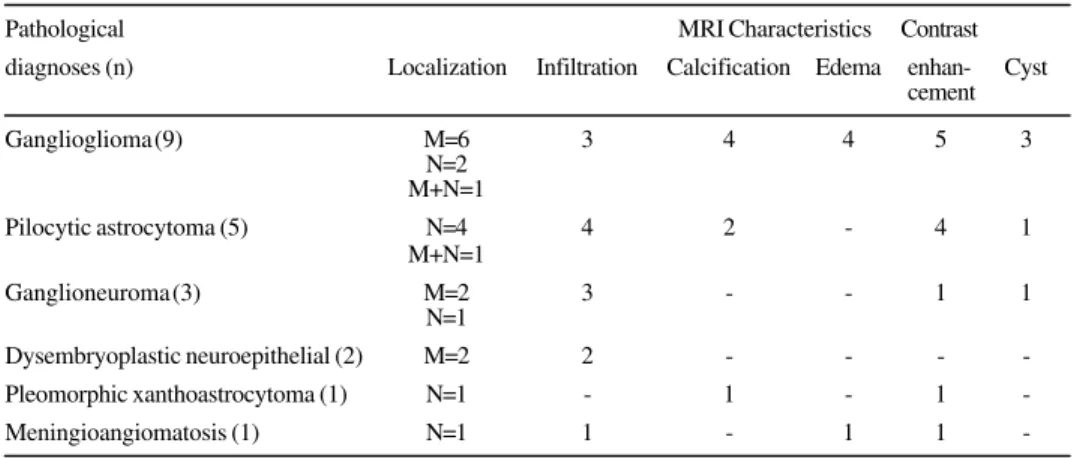
Objective: To present a surgical series of patients with low grade temporal gliomas causing intractable epilepsy, focusing on long-term seizure outcome.. Method: A
The aim of the present study was to investigate the influence of age at surgery and seizure onset on the surgical outcome of TLE-MTS patients treated at a Brazilian tertiary
Patterns of seizure control in patients with mesial temporal lobe epilepsy with and without hippocampus sclerosis. Fischer RS, Acevedo C, Arzimanoglou A, Bogacz A, Cross
