www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Feasibility
of
ossicular
chain
reconstruction
with
resin
cement
夽
Fernando
de
Andrade
Quintanilha
Ribeiro,
Yumi
Tamaoki,
Gabriel
Wynne
Cabral
∗IrmandadedaSantaCasadeSãoPaulo,DepartamentodeOtorrinolaringologia,SãoPaulo,SP,Brazil
Received15October2015;accepted7February2016 Availableonline29April2016
KEYWORDS
Ossicularprosthesis; Cyanoacrylates; Resincements
Abstract
Introduction:Disjunctionofossicularchainisacommonfindinginmiddleearchronicdisease. Inadditiontoossicularinterposition,variousmaterialshavebeenusedforreconstruction,such asceramicprostheses,polyethylene,andtitanium.
Objective:Becauseofthehighcostoftheavailableoptions,theauthorsproposetoreconstruct theossicularchainwithresincement,amaterialtypicallyusedindentalreconstructionand fixation.
Methods:Twoanatomicalpartsofthetemporalboneswereused,creatingadisjunctionofthe ossicularchainbetweentheincusandstaplesandthenreconstructingwithresincement.These reconstructionswererepeatedfourtimesbythreedifferentsurgeonstoensurethefeasibility ofthemethod.
Results:Atotalof12reconstructionswerecarriedout,fourpersurgeon.Afterapplyingthe cement,itcouldbeverifiedbytouchthatthespacewasfilledproperlybytheusedmaterial. Properarticulationwithmotiontransfertotheentireossicularchainwasalsoobserved.
Conclusion:Resincementisasuitablematerialinthereconstructionofossicularchaininjury, anditisinexpensiveandtechnicallysimple.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
夽 Pleasecitethisarticleas:RibeiroFA, TamaokiY,CabralGW.Feasibilityofossicularchainreconstructionwithresincement.BrazJ
Otorhinolaryngol.2017;83:132---6. ∗Correspondingauthor.
E-mail:[email protected](G.W.Cabral).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.02.014
PALAVRAS-CHAVE
Próteseossicular; Cianoacrilatos; Cimentosresinosos
Viabilidadedareconstruc¸ãodacadeiaossicularcomcimentoresinoso
Resumo
Introduc¸ão: Éfrequenteadisjunc¸ãodacadeiaossicularnasdoenc¸ascrônicasdaorelhamédia. Além deinterposic¸ões ossiculares, vários materiais já foramutilizadoscoma finalidadede reconstruí-la,comoprótesesdecerâmica,polietilenoetitânio.
Objetivo: Devido ao alto custo das opc¸ões existentes, propomos reconstruira cadeia com cimentoresinoso,materialusadonormalmentenareconstruc¸ãoefixac¸ãodentária.
Método: Serão utilizadasduas pec¸asanatômicas de ossos temporais, ondeserácriada uma disjunc¸ãodacadeiaentreabigornaeoestriboque,aseguir,seráreconstruídacomocimento resinoso.Estasreconstruc¸õesserãorepetidasquatrovezesportrêscirurgiõesdiferentes,para certificac¸ãodaviabilidadedométodo.
Resultados: Foram feitas um total de 12 reconstruc¸ões, quatro por cada cirurgião. Após aplicac¸ãodocimento,conseguimos,aotoque,perceberqueoespac¸ofoipreenchido adequada-mente pelomaterialempregado.Notamosaindaadequadaarticulac¸ãocomtransferênciade movimentoparatodaacadeiaossicular.
Conclusão:Ocimentoresinosoéummaterialviávelnareconstruc¸ãodelesõesdacadeia ossic-ular,eproporcionaummétodotecnicamentesimplesedebaixocusto.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Despiteisolatedreportsdatingfromthe19thandearly20th centuries,thedevelopmentofglueandself-adhesive sub-stancesforuseinhealthcarehaditsrealmomentumafter 1940, with theuse of plasma enrichedwith heterologous and homologousfibrinogen in the manufactureof biologi-caladhesives.1Thefirstdescriptionoftheuseofsynthetic
adhesives in medicine dates back to 1958, when epoxy (or epoxyline)wasusedtojoinbone tissuein experimen-tal fractures.2 But it was from the 1960s onwards, with
theadventofcyanoacrylates,thatresearchusingsynthetic adhesivesinmedicinehaditsbigboost.3
Originallydiscoveredin1949byHarryCoover, cyanoacry-lateswerecommerciallyreleasedonlyin1958,andin1959 itsapplicabilitywasreportedforclosing tissueinjuries.3,4
They are commonly used in medicine and have proven their applicability in clinical and experimental studies. In otorhinolaryngology, specifically in the area of ear surgery, experiments with the use of self-adhesive sub-stancesbeganaround1960.The mainareasofapplication focusedontheuseofadhesivesforsofttissueunion,such as skin, fascia, and tympanic membrane, ossicular chain reconstruction,andadherencebetweenprosthesesand mid-dle ear structures.5 Another derivative of cyanoacrylate
widelyinvestigatedforuseinotologicsurgerywas 2-butyl-cyanoacrylateorHistoacryl.Intheearly1970s,experiments withdogsusedHistoacryltojointhetemporalfasciatothe tympanicmembrane,createan interpositionbetween the bone/cartilageand stapesfootplate, andcreate an inter-positionbetween hammer andstirrup.These experiments indicatedthatHistoacryl,whenusedinsmallamounts,was not harmful to the inner and middle ear structures and degradedinashortperiodoftime,creatingastableunion betweentissues.5Otherderivativesofcyanoacrylateswere
alsousedtorepairfacialnerveindogs6andinrevision
sur-geriesforfixingastapedectomyprosthesistotheremainder oftheanvil,withgoodfunctionalresults.7
Asforthematerialsavailableforossicularchain recon-struction,autologousstructuressuchastympanicossicles, mastoid cortical bone, and tragal cartilage are still the most used options, despite the emergence of various metalprostheses,suchasgold, steel wire, platinum, and titanium; plastics, such as silicone,polyethylene, polyte-trafluoroethylene; and ceramics, such as ceramic oxide, carbon, calcium phosphate ceramic, hydroxyapatite, and glazed ceramic.8---10 All these synthetic materials have in
common the disadvantage of being expensive, making theiruse impractical in many centers.More recently, the introduction of ceramics and cements commonly used in restorationanddentalfillingshasbeenreportedinotology withagoaltoperformossicularchainreconstructionmore quicklyand easily.Among these,approximately tenyears ago the use of ceramic glass ionomer was relatively well studied,buttheresultsarestillveryvariableandsometimes inconsistent.11
Resincementwasfirstdevelopedindentistryasan alter-native to conventional cementation. The introduction of thisnewmaterialoffereddentistsanewtoolfor cement-ing that was easier to use than previous materials, and had great adhesiveness and esthetics.12 Currently,
vari-ous resin cements have been introduced in the market andare classified intotwo categories. Conventionalresin cements,whichdonothaveaninherentadhesiontotooth structureand requirethe use ofan adhesive system; and the self-adhesive resin cements, which do not require a prioradhesivetreatmentofdentalsubstrate.12,13TheRelyX
Unicem---3MESPE®wasthefirstself-adhesiveresincement,
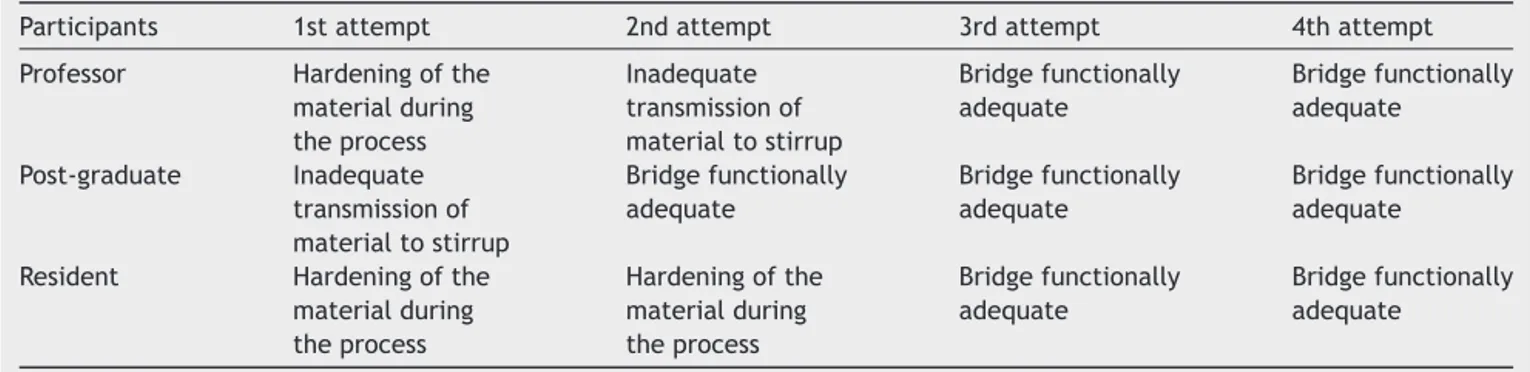
Table1 Proceduresperformed.
Participants 1stattempt 2ndattempt 3rdattempt 4thattempt
Professor Hardeningofthe materialduring theprocess
Inadequate transmissionof materialtostirrup
Bridgefunctionally adequate Bridgefunctionally adequate Post-graduate Inadequate transmissionof materialtostirrup
Bridgefunctionally adequate Bridgefunctionally adequate Bridgefunctionally adequate
Resident Hardeningofthe materialduring theprocess
Hardeningofthe materialduring theprocess Bridgefunctionally adequate Bridgefunctionally adequate
color,andchemicalcomposition.Theseproductshavetwo pastesrequiringmanipulationthatmaybemanualby trit-urationin capsulesor by aself-mixing dispenser.There is littleinformationonthe adhesionmechanism of adhesive cements.Thematerial’sbasiccompositionisthemonomeric system Bis-GMA (Bisphenol-A glycidyl methacrylate®) in combination withlow viscosity monomers, in addition to inorganic fillers(glasswith metallic charge, SiO2)treated withsilane.14 Theyhavehighadhesiveness,
biocompatibil-ity,areeasetohandle,andhaveasimple-to-useprotocol.14
Although they are already widely used in dentistry with excellent results, having been indicated for bonding var-ioussubstrates such asenamel, dentin,amalgam, metal, andporcelain, therearefew studiesregarding itsclinical performanceinthisarea,andnostudyinthemedicalfield. Inotology,theerosionofthelong armoftheincusisa frequentfinding. In aquest for amoreanatomical recon-struction,the authorsassessed the feasibilityof ossicular chainreconstructionwithresincement, anaccessibleand inexpensivematerial.
Methods
Two surgical specimens of human temporal bones willbe used,officiallyprovidedbytheDepartmentofMorphologyof theinstitution,whichwillbehandledinthesurgicaltraining sessionintemporalbonesoftheDepartmentof Otolaryngol-ogy.Afterfixationinadissectionbasin,thetympanomeatal flap will be folded down and the incudo-stapedial joint exposed. After the disarticulation of the incudostapedial joint,the distal portion of long process of the incuswill becut withirisscissors,sothatthedistancebetweenthe remaining long process and the stapes superstructure is approximately 3mm. This is the distance typically found inclinicalcasesofdisarticulationbynecrosisofthedistal portionofthelongarmoftheincus.
The resincementsthat willbeusedaretheRelix® and
Bifix® preparations,usuallyfound in dentalsupply stores.
Bifix® has a mixer coupled tothe tube, but it usesmore
material. It has the advantage of a fine nozzle that can depositthemixturedirectlyintothespacetobefilledand costsapproximatelyU$45(USD).Relix® without themixer
is cheaper andcan be usedin more occasions;its costis approximatelyU$42.50(USD).The chainintegritymustbe
redoneusingtheabovementionedmaterials,whichwillbe interposedwiththeuseofaspatula.
Theprocedurewillbeperformedbythreesurgeonswith differentlevelsofexperience:aprofessor,apost-graduate, andaresident.Eachwillperformtheprocedurefourtimes, and the difficulties regarding cement handling, interven-tion time,and interposition functioningwill be analyzed. Asthecementinterpositioncanberemovedthrougha care-fulmechanicalprocedure,itcanberemadeseveraltimesin theavailableparts.
Results
The mixingtimeof theusedmaterials was40s.The max-imumtimeavailabletofilltheboneinterruptionwiththe materialsanditsappropriatemodelingbeforehardeningwas 1min.Thus,acreamywhitebridgewasformedbetweenthe ossicles, mimicking the normal bone. By moving both the malleusandtheincus,itwasobservedthatthemovement wasproperlytransferredtothestapes.Table 1shows the proceduresperformed.
Discussion
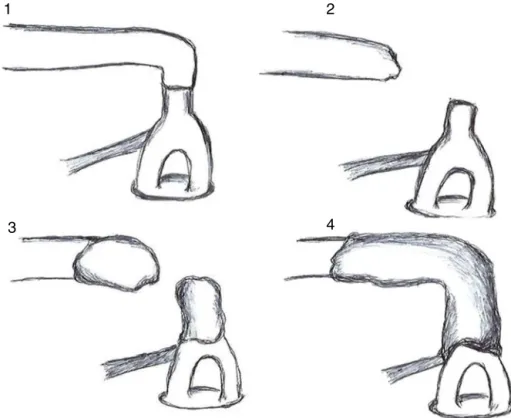
AsshowninTable1,theprocedurewasinitiallyperformed by theprofessor,whohad difficultyin managing thetime between the mixing of materials and their proper place-mentinfillingthedisjunction.Thiswasduetoanattempt todeposit thematerial onlywiththe useof a spatula,in whichithadgreatadherence;thisresultedinrapid harden-ing.Inthesecondattempt,withtheconcomitantuseofa pointer,thematerialwasremovedfromthespatulainsmall quantitiesandtakentotheareatobefilled. Thematerial wasthenplacedinterchangeablyinthestapesandincusto completethefilling,asshowninFig.1.
1
2
4
3
Figure1 Schematicdrawingofthefourattemptsatossicularchainreconstructionwithresincement.
couldleadtoitsfixation.Thesameoccurredatthefourth attempt.
The then-established procedure wasperformed by the otolaryngologist,whohaddifficultyinproperlypositioning thematerialonthestirruponthefirstattempt,butdidit correctlyinsubsequentattempts.Inthefirsttwoattempts, theresidentfacedearlyhardeningofthematerial,but prop-erlyhandleditinthetwosubsequentattempts.
Thus,threesurgeonswithdifferentexperiencesin oto-logicsurgerymanaged,withlittleinitialdifficultyandrapid learning,topromotetherestructuringoftheossicularchain injured by the erosion of the long process of the incus using resin cement. The same material can possibly be usedinotherproceduresofossicularchainreconstruction. However,additionalstudiesshouldbeconductedbeforeits application in human otologic surgery. In this line, there areongoingexperimentswithguineapigstoevaluateresin cementtoxicityandhearingrestorationafteritsusethrough BERA.
Conclusion
Resincementisaviablematerialforossicularinjury recon-struction.
Thereconstructionmethodisachievedwithlittletraining bysurgeons.
Theprocessisfinanciallyadvantageous.
Funding
This study wasapproved by the Ethics Committeeof the institution,registeredundertheNo.969.23412/03/2015.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.MorandiniW,OrtizV.Adesivosbiológicosemcirurgia.ActaCir Bras.1992;7:80---5.
2.SilvaLS,FigueiraNetoJB,SantosALQ.Utilizac¸ãodeadesivos teciduaisemcirurgias.BiosciJ.2007;23:108---19.
3.FagundesDJ,GoldenbergS.AdesivoemCirurgia.In:BurihanE, RamosRR,editors.Condutasemcirurgia.SãoPaulo:Atheneu; 2001.p.669---74.
4.Coover HW, Joyner FB, Shearer NH, Wicker TH. Chemistry andperformanceofcyanoacrylateadhesives.JSocPlastEng. 1959;15:413---7.
5.Siedentop KH.Reconstructionofossicles bytissueglue (His-toacryl)indog.Laryngoscope.1974;84:1397---403.
6.SiedentopK.H.,LoewyA.Facialnerverepairwithtissue adhe-sive.ArchOtolaryngol.1979;105:423---6.
7.Ribeiro FAQ, Doria S, Almeida R. Fixac¸ão da prótese de estapedotomia à cadeia ossicular com cianoacrilato. Relato de dois casos. Arquivos Int Otorrinolaringol. 2005;9: 76---80.
8.Dost P, Jahnke K. Biomaterials in reconstructive middle ear surgery. In: Jahnke K, editor. Middle ear surgery: recent advances and future directions. Stuttgart: Thieme; 2004. p. 56---72.
9.Shea J. PlastiporeTM total ossicular replacement prosthesis. Laryngoscope.1976;86:239---40.
11.BauerM,PytelJ,VónaI,GerlingerI.Combinationofionomer cementand bonegraftforossicularreconstruction. EurArch Otorhinolaryngol.2007;264:1267---73.
12.RadovicI,MonticelliF,GoracciC,VulicevicZR,FerrariM. Self-adhesive resin cements: a literature review. J Adhes Dent. 2008;10:251---8.
13.MansoAP,SilvaNR,BonfanteEA,PegoraroTA,DiasRA,Carvalho RM.Cementsandadhesivesforall-ceramicrestorations.Dent ClinNorthAm.2011;55:311---32.