REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Comparison
between
magnesium
sulfate
and
dexmedetomidine
in
controlled
hypotension
during
functional
endoscopic
sinus
surgery
Adnan
Bayram
a,∗,
Ays
¸e
Ülgey
a,
Is
¸ın
Günes
¸
a, ˙Ibrahim
Ketenci
b,
Ays
¸e
C
¸apar
a,
Aliye
Esmao˘
glu
a,
Adem
Boyacı
aaDepartmentofAnesthesiology,MedicalFaculty,ErciyesUniversity,Kayseri,Turkey
bDepartmentofOtorhinolaryngology,MedicalFaculty,ErciyesUniversity,Kayseri,Turkey
Received9December2013;accepted27April2014 Availableonline24May2014
KEYWORDS Controlled hypotension; Dexmedetomidine; Functional
endoscopicsinus surgery;
Magnesiumsulfate
Abstract
Backgroundandobjectives: Itiscrucialtodecreasebleedingduringfunctionalendoscopicsinus
surgery.Ourprimarygoalwastoinvestigatetheeffectsofmagnesiumsulfateand
dexmedeto-midineusedforcontrolledhypotensiononthevisibilityofthesurgicalsite.
Methods:60patientsagedbetween18and65yearswereenrolled.Inthemagnesiumsulfate
group (Group M), patients were administered 40mg/kg magnesium sulfatein 100mLsaline
solutionover10minastheintravenousloadingdose10minbeforeinduction,withasubsequent
10---15g/kg/hinfusionduringsurgery.Inthedexmedetomidinegroup(GroupD),patientswere
administered 1g/kgdexmedetomidine in100mLsalinesolution astheloading dose10min
before surgery and0.5---1g/kg/h dexmedetomidine duringsurgery. Deliberatehypotension
wasdefinedasameanarterialpressureof60---70mmHg.
Results:BleedingscorewassignificantlydecreasedinGroupD(p=0.002).Meanarterial
pres-surevaluesweresignificantlydecreasedinGroupDcomparedtothatinGroupM,exceptforthe
initialstage,afterinductionand5minafterintubation(p<0.05).Thenumberofpatientswho
requirednitroglycerinewassignificantlylowerinGroupD(p=0.01)andsurgeonsatisfactionwas
significantlyincreasedinthesamegroup(p=0.001).Aldreterecoveryscore≥9durationwas
significantlyshorterinGroupD(p=0.001).Therewasnodifferencebetweenthetwogroupsin
termsofrecoveryroomverbalnumericalratingscale.
Conclusions: Dexmedetomidinecan providemore effectivecontrolled hypotensionandthus
contributetoimprovedvisibilityofthesurgicalsite.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights
reserved.
∗Correspondingauthor.
E-mails:[email protected],[email protected](A.Bayram). http://dx.doi.org/10.1016/j.bjane.2014.04.003
PALAVRAS-CHAVE Hipotensão
controlada; Dexmedetomidina; Cirugiafuncional endoscópicadosseios paranasais;
Sulfatodemagnésio
Comparac¸ãoentredexmedetomidinaesulfatodemagnésioemhipotensão controladadurantecirurgiafuncionalendoscópicadosseiosparanasais
Resumo
Justificativaeobjetivos: Diminuirosangramentoduranteacirurgiafuncionalendoscópicados
seiosparanasaiséessencial.Nossoobjetivoprimáriofoiinvestigarosefeitosde
dexmedeto-midinaesulfatodemagnésio,usadosparaocontroledahipotensão,sobreavisibilidadedo
sítiocirúrgico.
Métodos: Foramincluídos noestudo 60 pacientes entre18 e 65 anos. Nogrupo sulfato de
magnésio(GrupoM),receberam40mgdesulfatodemagnésioem100mLkg−1desoluc¸ãosalina
durante10minutoscomo dosede carga intravenosa10minutos antesdainduc¸ão einfusão
subsequentede10-15gkg−1h−1duranteacirurgia.Nogrupodexmedetomidina (GrupoD),
receberam1gkg−1dedexmedetomidinaem100mLdesoluc¸ãosalinadurante10minutoscomo
dosedecarga10minutosantesdacirurgiae0,5-1gkg−1h−1dedexmedetomidinadurantea
cirurgia.Hipotensãocontroladafoidefinidacomopressãoarterialmédiade60-70mmHg.
Resultados: OvolumedesangramentodiminuiusignificativamentenogrupoD(p=0,002).Os
valoresdapressãoarterialmédiaforamsignificativamentemenoresnoGrupoD,emcomparac¸ão
comoGrupoM,excetonoestágioinicial,pós-induc¸ãoecincominutospós-intubac¸ão(p<0,05).
No Grupo D, onúmero depacientes quenecessitou denitroglicerina foi significativamente
menor(p=0,01)eograudesatisfac¸ãodocirurgiãofoisignificativamentemaior(p=0,001).O
tempoderecuperac¸ãoparaatingiroescoredeAldrete≥9foisignificativamentemenorno
grupoD(p=0,001).Nãohouvediferenc¸aentreosdoisgruposemrelac¸ãoaosescoresdaescala
numéricadeclassificac¸ãoverbalnasaladerecuperac¸ão.
Conclusões:Dexmedetomidina pode proporcionar um controle mais eficaz da hipotensão e
contribuir,assim,paraumamelhorvisibilidadedosítiocirúrgico.
©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos
direitosreservados.
Introduction
Controlled hypotension is performed in order to reduce bloodlossandtheneed fortransfusionduringthesurgery andtoimprovevisibilityofthesurgical sitebydecreasing the arterial pressure until hypotension is reached.1 The
primary surgical treatment for chronic rhinosinusitis is functional endoscopicsinus surgery (FESS). Intraoperative bleeding can diminish the visibility of the surgical site, leadingtoan increasedrate of complications. Therefore, improvingthevisibilityofthesurgicalsitebyreducing bleed-ingduringFESSisanimportantissueforanesthesiologists.2
Incontrolledhypotension,severalagents havebeen used, eitheraloneorincombinationwitheachother;however,an idealagentforinducingcontrolledhypotensioncannotbe asserted.Theideal agentusedfor controlledhypotension musthavecertaincharacteristics,suchaseaseof adminis-tration,ashortonsettime,aneffectthatdisappearsquickly whenadministrationisdiscontinued,rapidelimination with-outtoxicmetabolites,negligibleeffectsonvitalorgans,and predictableanddose-dependenteffects.1,3---5
Dexmedetomidineis ahighlyselective␣2-adrenoceptor agonist with sedative, anxiolytic, and analgesic char-acteristics. Dexmedetomidine mediates central ␣2A and imidazolinetype1receptors.Theactivationofthese cen-tralreceptorsresultsinadecreaseinnorepinephrinerelease andleadstoadecreaseinbloodpressureandheartrate.6
Ithas been reportedthat magnesium sulfate isa good agentforcontrolledhypotension,andthatitstabilizesthe cell membrane and intracytoplasmic organelles by medi-ating the activation of Na+-K+ ATPase and Ca++ ATPase enzymes,whichplayaroleintransmembraneionexchange duringthedepolarizationandrepolarizationphases.5,7,8 In
addition, Mg++ inhibits the release of norepinephrine by blockingtheN-typeCa++channelsatnerveendingsandthus decreasethebloodpressure.9
Thereareseveralstudieswhichhaveassessedthe effec-tiveness of dexmedetomidine and magnesium sulfate in controlledhypotension.Thesetwoagentshavebeen com-paredwithotherhypotensiveagentsintermsoftheirrolein hypotensiveanesthesia,buttothebestofourknowledge, nostudycomparingthese twoagents witheachother has beencitedinthescientificliterature.2,5,7,10
Ourprimarygoalinthisstudywastocomparetheeffects ofdexmedetomidineandmagnesiumsulfateagentsonthe visibilityofthesurgicalsite;oursecondarygoalwasto com-parethesetwoagentsintermsofsatisfactionofthesurgeon, recoveryperiod,adverseeffectsandpostoperative analge-sia.
Materials
and
methods
whowereselectedforFESS,betweenJanuary2012andJuly 2013.Thisstudywasapprovedbythelocalethicscommittee (No: 2011-221), andinformed consent wasobtained from the patients. The study was conducted according to the DeclarationofHelsinki.Patientswithkidney,liver, hemato-logicalandneuromusculardiseases,diabeticneuropathyor anyknownallergyhistorytostudiedagentswereexcluded fromthestudy.Thosewithabodyweightexceedingtheideal bodyweightbymorethan30%andthosereceivingcalcium channel blockers, non-steroidal anti-inflammatory drugs, agentsaffecting neuromuscularblockage,andagents con-traindicatedforcontrolledhypotensionwerealsoexcluded fromthestudy.Patientsandtheirrelativeswereinformed for verbal numerical rating scale (NRS) (0: no pain, 10: severe pain) at the preoperative patient examination. All patients were administered a 5mL/kg/hour intra-venous(i.v.)isotonicsolution(LactatedRinger)infusion2h before the induction, which was continued during the surgery.
Afterthepatientsweretakenintotheoperatingroom, meanarterial pressure (MAP),heart rate(HR), peripheral oxygensaturation(SpO2)andendtidalcarbondioxidewere monitored(DatexOhmedaS/5,Helsinki,Finland); hemody-namicdataweremeasuredevery5min.Hemodynamicdata wererecordedattheinitialphase,aftertheinduction, 5, 10,15,30and45minafterintubation,and1and5minafter extubation.
Patients were divided into two groups by choosing randomly from sealed envelopes. The study participants, operation nurse and theotorhinolaryngologist constituted the ‘blind’ study group. An anesthetist who did not take partintheintra-operativefollow-uppreparedthemedicine used. For topical vasoconstriction and local anesthesia, 1/1000 epinephrine soaked cotton was placed in the nasal cavity for 5min. A solution containing 40mg/2mL lidocainehydrochloride+0.025mg/2mLepinephrine (Jeto-caine,Adeka,Istanbul,Turkey)wasappliedtothenasalside ofboth themedialandlateralconchaeatthesamedose. To the patients in Group M, 40mg/kg i.v. magnesium sul-fate(OSEL, ˙Istanbul,Turkey)in100mLsalinesolutionwas appliedasaloadingdose10minbeforetheinduction and then titrated at an infusion rate of 10---15mg/kg/hour to maintain MAP within the target range during surgery. To thepatientsingroupD,1g/kgi.v.dexmedetomidine (Pre-cedex; Hospira, Rocky Mount, NC, USA) in 100mL saline solutionwasapplied10minbeforesurgeryandthentitrated at an infusion rate of 0.5---1g/kg/hour tomaintain MAP withinthetargetrangeduringsurgery.Thesedosageswere based on a previous study,5,10---12 whereas the magnesium
and dexmedetomidine infusion rates were chosen to sus-tainthetargetMAPandavoidtheserioushemodynamicside effects.
Deliberate hypotension was defined as an MAP of 60---70mmHg7;50gnitroglycerinewasappliedinthe
pres-enceof MAP exceeding70mmHgand 5mg ephedrinewas appliedinthepresenceofMAPunder55mmHg. Bradycar-diawasdefinedasaheartratedecreasedbymorethan20% oftheinitialheartrate;0.5mgi.v.atropinewasappliedto patientswhodevelopedbradycardia.
Neuromuscular stimulus was monitored via accelome-try of the right adductor pollicis muscle in all patients (TOF-Guard®;Biometer,Denmark).Afterplacingthesurface
electrodesontheulnarnerveareaofthewrist,2.5mg/kg propofol and 1g/kg fentanyl i.v. were administered in order to induce anesthesia. After achieving unconscious-ness,singlemuscletwitch auto-calibration atthelevel of 100% was performed withthe use of supramaximal stim-ulus (60mA) before rocuronium injection. To the patient 0.6mg/kgi.v.rocuroniumwasinjectedandorotracheal intu-bation was performed after achieving T1=0%. Anesthesia wasmaintainedwith50%nitrousoxideand50%oxygen,and 5---6%desflurane wasadjusted toachieve atarget Bispec-tralIndex(BIS)between40and60.TheBISelectrodeswere placedontheforeheadandwereconnectedtoanA-2000BIS monitoringsystem(AspectMedicalSystemInc.Natick,MA, USA).The presenceof hypertensionor tachycardia during anesthesia,whileBISwasbetween40and60,wasattributed toinsufficientanalgesiaandabolusdoseoffentanyl1g/kg wasgiven.
Volume-controlled mechanical ventilation was per-formedwithanend-tidalcarbondioxidepressurebetween 35and40mmHg(AvanceS/5,GEDatex-Ohmeda,Helsinki, Finland). Patients were intraoperatively warmed with an underbodyheatedblanket (Astoped Duo120 controlunit, Stuttgart, Baden-Wurttemberg, Germany). Skin tempera-ture of the patient measured on the adductor pollicis musclewasmaintainedabove32◦
C.Anesophageal temper-ature probe was inserted into the lower esophagus after the intubation for measuring the core temperature, and normothermia wasaccomplished with the use of warmed intravenousfluids (enFlow IVFluid/Blood warmer system, Lexington,MA,USA)duringthesurgery.Inthepresenceof T1exceeding25%ofthecontrolvalue,0.15mg/kg rocuro-niumwas applied in orderto maintain the T1 under 10% during surgery. Magnesium sulfate and dexmedetomidine infusions were discontinued at the end of the surgery. Then,0.02mg/kgatropineand0.04mg/kgneostigminewas applied in order to antagonize the neuromuscular block-ageinthepresenceofT1responsesexceedingthecontrol valueby 25%.The periods betweenstopping the anesthe-sia and extubation and between extubation and opening theeyes witha loud verbal stimuluswere determined as theextubationdurationandeyeopeningduration, respec-tively. Patients were extubated when BIS≥70. The time passinguntilanAldretepost-anesthesiarecoveryscore≥9 was defined as the recovery period.13 Aldrete score was
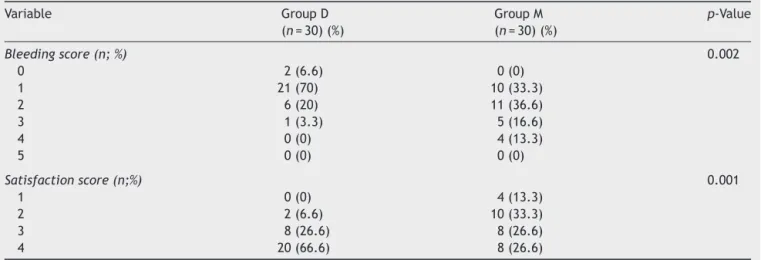
evaluated by an anesthetist who was ‘blind’ in terms of patient groups every 15min for 60min. Patients with an Aldretescore≥9weretransferredtotheward.Allpatients wereoperated bythesamesurgeon,andsurgical sitewas rated according toa 6-point scale every 5min by him in terms of bleeding and dryness (Table 1)14: 0=no
bleed-ing; 1=minor bleeding, no aspiration required; 2=minor bleeding,aspirationrequired;3=minorbleeding,frequent aspirationrequired;4=moderatebleeding,visibleonlywith the aspiration; and 5=severe bleeding, continuous aspi-ration required, very hard to perform surgery. Surgeon satisfactionwasscoredbythesamesurgeonwitha4-point scale:1=bad,2=moderate,3=good,4=excellent.
Table1 Categoryscaleforassessmentofintraoperativesurgicalfieldandsurgeonsatisfactionscore.
Variable GroupD
(n=30)(%)
GroupM
(n=30)(%)
p-Value
Bleedingscore(n;%) 0.002
0 2(6.6) 0(0)
1 21(70) 10(33.3)
2 6(20) 11(36.6)
3 1(3.3) 5(16.6)
4 0(0) 4(13.3)
5 0(0) 0(0)
Satisfactionscore(n;%) 0.001
1 0(0) 4(13.3)
2 2(6.6) 10(33.3)
3 8(26.6) 8(26.6)
4 20(66.6) 8(26.6)
GroupD,dexmedetomidinegroup;GroupM,magnesiumsulfategroup
Datashowthenumberofcasesandthepercentagerate.pvaluecalculatedusingChi-squaretest.
Bleedingscore:0=nobleeding;1=slightbleeding-nosuctionofbloodrequired;2=slightbleeding-occasionalsuctioningrequired.
Sur-gicalfieldnotthreatened;3=slightbleeding-frequentsuctioningrequired.Bleedingthreatenssurgicalfieldafewsecondsaftersuction
isremoved;4=moderatebleeding-frequentsuctioningrequired.Bleedingthreatenssurgical fielddirectly aftersuction isremoved;
5=severebleeding-constantsuctioningrequired.Bleedingappearsfasterthancanberemovedbysuction.Surgicalfieldseverely
threat-enedandsurgerynotpossible.
Satisfactionscore:1=poor;2=moderate;3=good;4=verygood.
Statisticalanalysisandstudysamplesize calculation
All statistical analyses were performed R 3.0.2 software
(www.r-project.org). Student’s t test was used for the
comparison of hemodynamic parameters and duration of anesthesia,operation,extubation,eyeopening,andAldrete recoveryscore≥9.Mann---WhitneyUtestwasusedforthe comparisonofNRSvalues;Chi-squaretestwasusedto com-paresurgeonsatisfactionandvisibilityofthesurgicalsite, whileFisher’sexacttestwasusedincomparisonof brady-cardia, hypotension, vomiting, shivering, and number of patients requiring fentanyl and nitroglycerine administra-tion.To determine the changes over time in each group, weusedrepeatedmeasures ANOVA,andmultiple compar-isonswerecorrectedusingBonferroni’smethod.p<0.05was definedasstatisticallysignificant. Samplesize calculation wasbasedontheinitialpilotstudy.Since␣,andaverage differencevalues were calculated as0.05, 0.20 and 0.5, respectively, (1.1±0.56 and1.6±0.69) for 10patients in eachgroupintermsofthe20thminbleedingscore,a min-imumof25patientswerecalculatedasnecessaryforeach group.
Results
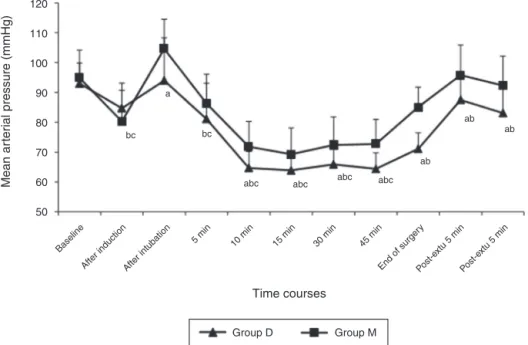
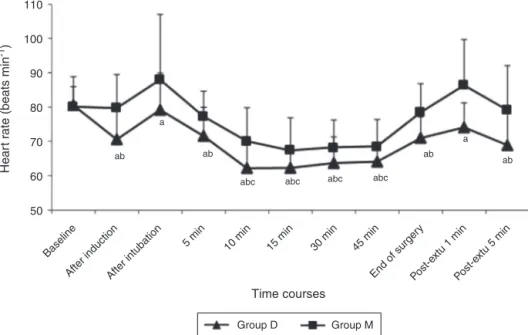
Sixtypatients were enrolledin the study andall patients completedthe study.Demographic data, BISvalues,total rocuroniumnecessity, duration of operation and anesthe-sia were similar in each group (p>0.05) (Table 2). MAP wassignificantly lowerinGroup Dthan inGroup Mforall measurementsexcepttheinitialstage,afterinductionand 5minafterintubation(p<0.05)(Fig.1).HRwassignificantly lowerinallmeasurementsexcepttheinitialstageinGroup
D comparedtoGroup M(p<0.05)(Fig.2). Bleedingscore wassignificantlydecreasedingroupD(p=0.002)(Table1, Fig.3).SurgeonsatisfactionwassignificantlybetterinGroup D(p:0.001)(Table1).
There was no significant difference between the two groupsintermsofbradycardia,hypotension,vomiting, shiv-ering and fentanyl necessity.Nitroglycerine necessity was significantlylowerinGroup D(p=0.01)(Table2).Thetwo groups weresimilarin terms ofextubation andeye open-ingduration.The durationuntilreachinganAldretescore
≥9wassignificantlyshorterinGroupD(p=0.001)(Table2). There wasnodifferencein terms of the15th, 30th,45th and60thminNRSscores[GroupD=3(2---6);3(2---6);3(2---5); 3(2---4);GroupM=3(1---6);3(1---6);3(2---5);3(2---5)median (min---max)respectively](p>0.05).
Discussion
Thisstudyrevealedthatdexmedetomidinewasmore effec-tivein performingcontrolledhypotensionduring FESSand thatitprovidedabettersurgicalsiteandsurgeon satisfac-tionandalowernecessityofadditionalhypotensiveagent thanmagnesiumsulfate.
In a study assessing the hypotensive effects of dexmedetomidine administered as a 0.4g/kg/hour i.v. infusion following a 1g/kg i.v. bolus dose in middle ear surgery,ithasbeenreportedthatsurgeonsatisfactionwas increased and inhalation agent necessity to decrease the MAPby upto30% wasdecreased inthedexmedetomidine administered patient group.15 Secondary decrease in the
Table2 Perioperativecharacteristicsanddata.
GroupD(n=30) GroupM(n=30) p-Value
Gender(F/M) 22/8 19/11 0.54a
Age(year) 45.1±11.1 39.5±11.3 0.77
Bodyweight(kg) 76.6±6.1 76.7±12.5 0.95
Durationofanesthesia(min) 67.4±20.5 72±17.3 0.39 Durationofsurgery(min) 55.9±18.3 61.5±17.3 0.26
Extubationtime(min) 4.5±2.3 5.8±2.9 0.08
Eyeopeningtime(min) 4.1±1.9 4.6±2.2 0.39
TimerequiredtoreachAldretescore≥9(min) 11.8±2.5 14.8±3.0 0.001
Bradycardia 4(13.3%) 1(3.3%) 0.35a
Hypotension 4(13.3%) 2(6.6%) 0.66a
Vomiting 1(3.3%) 4(13.3%) 0.35a
Shivering 1(3.3%) 3(10%) 0.61a
Fentanylnecessity 1(3.3%) 7(23.3%) 0.052a
Nitroglycerinenecessity 2(6.6%) 10(33.3%) 0.02a
Totalrocuroniumnecessity(mg) 53.4±11.4 49.9±9.57 0.205
GroupD,dexmedetomidinegroup;GroupM,magnesiumsulfategroup. Datashowthenumberofcasesormean±SDandthepercentagerate.
pvaluescalculatedusingStudent’st-testandp<0.05valueisshowninbold. a pvaluescalculatedusing
2test(Fisher’sexacttest)andp<0.05valueisshowninbold.
thissituation.Wealsoobservedthatbleedingatthe surgi-calsitewasdecreasedandsurgeonsatisfactionimprovedin thedexmedetomidine study group.Shams etal.16
demon-strated thatdexmedetomidine, administeredasa 1g/kg i.v.bolus anda0.4---0.8g/kg/hi.v. infusion,wassafefor controlled hypotensionand is effective in providing ideal surgicalfieldduringFESS.InastudybyGuvenetal.2
com-paring the hypotensive effects of dexmedetomidine and placeboagent,it wasconcludedthat dexmedetomidineis a safe and effective agent in controlled hypotension and can be an alternative to other agents. In another study
assessingtheeffectsofdexmedetomidine administeredas a 1g/kg i.v. bolus and a 0.7g/kg/hour i.v. infusion, it was stated that dexmedetomidine decreased bleeding at thesurgicalsite,improvedthevisibilityofthesurgicalsite anddecreased theneedforintraoperative fentanyl.10 The
analgesic effects of dexmedetomidine can be due to the activation of␣2B-adrenoceptors at the level of the dorsal horn of the spinal cordand the inhibition of substance P release.17Inourstudy,therewasnosignificantdifferencein
termsoffentanylneed;thislackofnecessitywasattributed tobothagentshavinganalgesiceffects.
Baseline
Afte r induction
After intubation
5 min 10 min
Time courses
Group D bc
a
bc
abc abc abc abc
ab ab
ab
Group M
Mean ar
ter
ial pressure (mmHg)
120
110
100
90
80
70
60
50
15 min 30 mi n
45 min
End of surger y
Po st-extu 5
min
Post-e xtu 5 min
Figure1 Meanarterialpressureforthegroups.ap<0.05significantdifferencebetweenthegroups(Student’sttest),bp:Group
dexmedetomidine, significantdifference inthegroup comparedto baselinevalues, cp: Groupmagnesium sulphate,significant
Baseline
After inductionAfter intubation
5 min 10 min
Time courses
Group D ab
a
ab
abc abc abc abc
ab
ab a
Group M
Hear
t r
ate (beats min
-1)
110
100
90
80
70
60
50
15 min 30 m in
45 min
End of surger y
Post-e xtu 1 min
Post-e xtu 5 min
Figure2 Heart ratevalues inthe groups. ap<0.05significant difference between the groups (Student’st test), bp:Group
dexmedetomidine,significant difference inthegroup compared to baselinevalues, cp:group magnesiumsulphate, significant
differenceinthegroupcomparedtobaselinevalues(repeatedmeasuresANOVAtestafterBonferroni’stest).
Groups
Marginal means of oper
ativ
e field b
leeding
Group M Group D
∗
32.5
1.5
0.5 2
1
0
Figure 3 Rating of bleeding quantity. p values calculated using2test(Fisher’sexacttest)(*p=0.001).
The use of different doses of magnesium to perform deliberatehypotensionhasbeenstudied.Inastudy compar-ingmagnesiumsulfatewithplaceboinpatientsundergoing FESS,itwasstatedthatcontrolledhypotensionwasachieved by using 40mg/kg i.v. bolus and 15mg/kg/hour i.v. infu-sionof magnesium sulfate and that the use of thisagent decreased bleeding and duration of surgery.5 Ryu et al.7
comparedmagnesiumsulfatewithremifentanilinpatients undergoing middle ear surgery. Magnesium sulphate was administered as a 50mg/kg i.v. bolus and 15mg/kg/hour i.v.infusioninthesamestudy.Theystatedthatcontrolled hypotensioncouldbeachievedwithbothagents, butthat magnesiumsulfateprovidedmoreeffectiveanalgesiainthe postoperativeperiod.Sincetherewasnosignificant differ-ence between the two groups in terms of NRS scores in
thisstudy,antinociceptive effectswereattributedtoboth agents.TheantagonisteffectofmagnesiumatN-methyl-d
-aspartate receptorsraisedinterest instudiessearchingits adjuvanteffectinperioperativeanalgesia.18
Kalra etal.19 compared magnesium sulfate with
cloni-dine,which is another␣2 receptorantagonist,in patients undergoinglaparoscopicsurgery;itwasstatedthatthe dura-tion untilachieving a replytoverbal stimulus waslonger in the magnesium sulfate patientgroup compared to the 1g/kg i.v.and1.5g/kgi.v. clonidinegroups,whichwas attributedtothedepressoreffectsofmagnesiumsulfateon the central nervous system. There was nosignificant dif-ferenceintermsofeyeopeningdurationbetweenthetwo groups. Furthermore the time until achieving an Aldrete score≥9wasshorterinthedexmedetomidinepatientgroup, suggestingthatdexmedetomidineresultsinasleepingeffect onlocuscoeruleus,similartothatofnormalsleeping,and thusresultsinafasterawakening.Therewasnodifference in terms of adverse effects and patient number requir-ingfentanyladministration.Nevertheless, theneedforan additionalnitroglycerinedose inordertoobtainadequate hypotensionwashigherinthemagnesiumsulfate group,a differencewhichwasattributedtotheagentdosesusedin thisstudy.Additionalstudiesconductedwithdifferentdoses cancontributetothissubject.
Inthisstudy,postoperativemagnesium sulfateand cal-ciumlevelswerenotmeasured,whichcanbeconsideredas one limitationof the study.The administrationof alarge dose of magnesium sulfate, for examplein thetreatment ofpreeclampsia,maycausetransienthypocalcaemiadueto renalcalciumlossortheinhibitionofparathyroidfunction.20
sulfate onpatientsundergoingmiddle earsurgery, no sig-nificantdifferencewasobservedbetweenthepreoperative andpostoperativeserummagnesiumsulfatelevels.7
Conclusions
Weconcludethatdexmedetomidineusedatthedoses men-tioned in the study provided controlled hypotension in a moreeffectiveandmorestablemannerinpatients undergo-ingFESS,andalsoincreasedsurgeonsatisfactionandquality ofsurgicalsite,whilenotprolongingtherecoveryperiod.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.DegouteCS.Controlledhypotension:a guidetodrugchoice. Drugs.2007;67:1053---76.
2.GuvenDG,DemiraranY,SezenG,etal.Evaluationofoutcomes inpatients given dexmedetomidine in functional endoscopic sinussurgery.AnnOtolRhinolLaryngol.2011;120:586---92. 3.MarchalJM,Gomez-LuqueA,Martos-CrespoF,etal.Clonidine
decreasesintraoperativebleedinginmiddleearmicrosurgery. ActaAnaesthesiolScand.2001;45:627---33.
4.PiperSN,SuttnerSW,MaleckWH,etal.Effectsofsodium nitro-prussideinducedcontrolledhypotensiononpancreaticfunction assessedbypancreatitis-associatedproteininpatients undergo-ingradicalprostatectomy.EurJAnaesthesiol.2002;19:609---13. 5.ElsharnoubyNM,ElsharnoubyMM.Magnesiumsulfateasa tech-niqueofhypotensiveanesthesia.BrJAnaesth.2006;96:727---31. 6.JoosteEH,MuhlyWT,IbinsonJW,etal. Acutehemodynamic changesafterrapidintravenousbolusdosingof dexmedetomi-dineinpediatrichearttransplantpatientsundergoingroutine cardiaccatheterization.AnesthAnalg.2010;111:1490---6. 7.RyuJH,SohnIS,DoSH.Controlledhypotensionformiddleear
surgery: a comparisonbetween remifentanil and magnesium sulfate.BrJAnaesth.2009;103:490---5.
8.KoinigH,WallnerT,MarhoferP,etal.Magnesiumsulfatereduces intra-andpostoperativeanalgesicrequirements.AnesthAnalg. 1998;87:206---10.
9.Shimosawa T, Takano K, Ando K, et al. Magnesium inhibits norepinephrine release by blocking N-type calcium chan-nels at peripheral sympathetic nerve endings.Hypertension. 2004;44:897---902.
10.Ayoglu H, Yapakci O, Ugur MB, et al. Effectiveness of dexmedetomidineinreducingbleedingduringseptoplastyand tympanoplastyoperations.JClinAnesth.2008;20:437---41. 11.AltanA,TurgutN,YildizF,etal.Effectsofmagnesiumsulphate
and clonidine onpropofol consumption, haemodynamics and postoperativerecovery.BrJAnaesth.2005;94:438---41. 12.Richa F, Yazigi A, Sleilaty G, et al. Comparison between
dexmedetomidineandremifentanilforcontrolledhypotension duringtympanoplasty.EurJAnaesthesiol.2008;25:369---74. 13.Aldrete JA, Vazeery A. Is magnesium sulfate an anesthetic?
AnesthAnalg.1989;68:186---7.
14.JacobiKE,BöhmBE,RickauerAJ,etal.Moderatecontrolled hypotensionwithsodiumnitroprussidedoesnotimprove surgi-calconditionsordecreasebloodlossinendoscopicsinussurgery. JClinAnesth.2000;12:202---7.
15.Nasreen F, Bano S, Khan RM, et al. Dexmedetomidine used toprovide hypotensiveanesthesia duringmiddleearsurgery. IndianJOtolaryngolHeadNeckSurg.2009;61:205---7.
16.Shams T, El Bahnasawe NS, Abu-Samra M, et al. Induced hypotensionforfunctionalendoscopicsinussurgery:a compara-tivestudyofdexmedetomidineversusesmolol.SaudiJAnaesth. 2013;7:175---80.
17.Khan ZP, Ferguson CN, Jones RM. Alpha-2 and imidazoline receptor agonists. Theirpharmacology and therapeutic role. Anaesthesia.1999;54:146---65.
18.DubéL,GranryJC.Thetherapeuticuseofmagnesiumin anes-thesiology,intensivecareandemergencymedicine:areview. CanJAnesth.2003;50:732---46.
19.Kalra NK,Verma A, Agarwal A, et al. Comparative studyof intravenouslyadministeredclonidineandmagnesiumsulfateon hemodynamicresponsesduringlaparoscopiccholecystectomy. JAnaesthesiolClinPharmacol.2011;27:344---8.