www.jped.com.br
ORIGINAL
ARTICLE
Association
between
general
and
abdominal
obesity
with
high
blood
pressure:
difference
between
genders
夽
,
夽夽
Alison
O.
Silva
a,
Micaelly
V.
Silva
a,
Lisley
K.N.
Pereira
a,
Wallacy
M.N.
Feitosa
a,b,
Raphael
M.
Ritti-Dias
c,
Paula
R.B.
Diniz
d,e,
Luciano
M.F.T.
Oliveira
a,b,d,e,∗aFaculdadeAssociac¸ãoCaruaruensedeEnsinoSuperioreTécnico(ASCES),Caruaru,PE,Brazil bGrupodePesquisaemSaúdePública(GPESP),Caruaru,PE,Brazil
cHospitalIsraelitaAlbertEinstein,SãoPaulo,SP,Brazil
dNúcleodeTelessaúde,UniversidadedePernambuco(UPE),Recife,PE,Brazil eUniversidadeFederaldePernambuco(UFPE),Recife,PE,Brazil
Received8March2015;accepted27May2015 Availableonline12December2015
KEYWORDS
Hypertension; Adolescent; Prevalence
Abstract
Objective: Toassesstheassociationbetweengeneralandabdominalobesitywithhighblood pressureinadolescentsofbothgendersfromthepublicschoolsystem.
Methods: This was an epidemiological, descriptive, exploratory study, with a quantitative approachandlocalscopewhosesampleconsistedof481highschoolstudents(aged14---19), selectedbyusingarandomclustersamplingstrategy.Bloodpressurewasmeasuredthrough theuseofautomatedmonitorandwasconsideredhighwhenthepressurevalueswereator abovethe95thpercentile.Theanalyseswereperformedusingthechi-squaredtestandbinary logisticregression.
Results: Theprevalenceofhighbloodpressurewas6.4%,anditwashigheramongboys(9.0%vs. 4.7%,p<0.05).Therewasnosignificantdifferencebetweengeneral(p=0.903)andabdominal obesity(p=0.157)whengenderswerecompared.Afteradjustingforage,highbloodpressure was associatedwith general(OR=6.4;p<0.001)andabdominalobesity (OR=7.0;p<0.001)
夽 Pleasecitethisarticleas:SilvaAO,SilvaMV,PereiraLK,FeitosaWM,Ritti-DiasRM,DinizPR,etal.Associationbetweengeneraland abdominalobesitywithhighbloodpressure:differencebetweengenders.JPediatr(RioJ).2016;92:174---80.
夽夽
StudycarriedoutatFaculdadeAssociac¸ãoCaruaruensedeEnsinoSuperioreTécnico(ASCES),Caruaru,PE,Brazil.
∗Correspondingauthor.
E-mail:[email protected](L.M.F.T.Oliveira). http://dx.doi.org/10.1016/j.jped.2015.05.007
onlyamongboys,whencomparingthefourthquartilewiththefirstquartileofbodymassindex (≤18.6kg/m2vs.≥23.5kg/m2)andwaistcircumference(≤69cmvs.≥80.1cm).
Conclusion: Itwasobservedthatgeneralandabdominalobesityareassociatedwithhighblood pressureonlyinboys,regardlessofage.
©2015SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Hipertensão; Adolescente; Prevalência
Associac¸ãoentreaobesidadegeraleabdominalcomapressãoarterialelevada: diferenc¸aentregêneros
Resumo
Objetivo: Analisar a associac¸ão entre obesidade geral e abdominal com a pressão arterial elevadaemadolescentesdeambososgênerosdarededeensinopúblico.
Métodos: Trata-se de um estudo epidemiológico, descritivo, exploratório, com abordagem quantitativaeabrangênciamunicipal cujaamostrafoiconstituídade481estudantes(14-19 anos)doensinomédio,selecionadopormeiodeumaestratégiadeamostragemaleatóriade cluster.Apressãoarterialfoimedidaatravésdautilizac¸ãodeequipamentosautomáticos,sendo considerada elevada quandoos valores pressóricosestivessem iguais ouacimado percentil 95. Asanálises foramrealizadas através doteste de Qui-quadradoe daregressão logística binária.
Resultados: Aprevalênciadepressãoarterialelevadafoide6,4%,sendomaiorentreosrapazes (9,0% vs. 4,7%, p<0,05). Não foi observada diferenc¸a significante entre aobesidade geral (p=0,903)eabdominal (p=0,157)quandocomparadososgêneros.Apósojustepelaidade, apressãoarterialelevadafoiassociadacomaobesidadegeral(OR=6,4;p<0,001)e abdom-inal(OR=7,0;p<0,001)apenasentreosrapazes,quandocomparadooquartoquartilcomo primeiroquartildoíndicedemassacorporal(≤18,6Kg/m2Vs≥23,5Kg/m2)edacircunferência
dacintura(≤69cmVs≥80,1cm).
Conclusão: Foiobservado queaobesidade geraleabdominal estáassociadacom apressão arterialelevadaapenasentreosrapazes,independentementedaidade.
©2015SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Todososdireitos reservados.
Introduction
Highblood pressure(HBP) is considered a majorrisk fac-torforcardiovasculardiseaseforadults,aswellaschildren and adolescents.1,2 Its diagnosis and early treatment can
prevent the occurrence of future adverse cardiovascular
events,sinceHBPinchildhoodisapredictorofhypertension
inadulthood.3 InBrazil,theprevalence ofHBPinchildren
rangesfrom2.5%4to44.7%5;asitisasymptomatic,the
iden-tificationandtreatmentofHBPisoftenneglected.6
By consensus,general and abdominalobesity are
con-sidered aspredisposing factors for HBPonset7;moreover,
excessbodyfat accumulationinthe earlystages oflifeis
associatedwiththeonsetof cardiovascularandmetabolic
diseasesinadulthood.8However,thereisevidence
demon-strating thatbody fat distributionis moreimportant than
obesity alone.9,10 Inthis sense,it has been observed that
abdominal fat accumulation is closely related to HBP,
and it is considered the biggest contributor to metabolic
complicationsoftheobesepopulation.11
Another factor that can influence blood pressure (BP)
valuesisthedifferencebetweengenders.12,13 Studieshave
confirmedthatboyshavehigherBPthangirls.14---16However,
theassociationbetweenobesityandHBPisusuallyassessed,
but the interaction in relation to gender is not tested,
andthisfactorcandistortthefoundresults.1,16Therefore,
theobjectiveof thisstudywastoanalyzethe association
betweengeneralandabdominalobesitywithHBPin
adoles-centsfrompublicschools,whileconsideringthedifference
betweengenders.
Methods
Thiswasa descriptivestudywithaquantitative approach thatintegratedaschool-basedcross-sectional epidemiolog-ical survey of municipal scope. The sample consisted of studentsaged14---19years,ofbothgenders,enrolledinthe state public high schools in the city of Caruaru, state of Pernambuco,Brazil.Thetotalpopulationwasestimatedat 8833youngindividualsdistributedin15schools,according totheStateSecretariatofEducationandCulture.
Toselecttherequiredsample,atwo-stagerandom clus-tersamplingstrategywasused,and‘‘school’’and‘‘class’’ represented,respectively,thesampleunitsinthefirstand secondstage.AllpublicschoolsinthecityofCaruaruwere considered eligible for inclusion in the study. In the first stage,school density was usedas the stratification crite-rionineach microregionof thecity(GerênciaRegionalde Educac¸ão --- Gere),according totheir size. In the second stage, the density of classes in the selected schools was considered by school shift (day and night) as a criterion tochoose, by drawing lots, those in which the question-naireswouldbeapplied.Allstudentsintheselectedclasses wereaskedtoparticipatein thestudy,regardless oftheir age. Aftertheir application, thequestionnaires answered bystudentsolderthantheestablishedage(19years)were excluded.
Data collection was carried out from June to Novem-berof 2014. The questionnaireswere collectively applied in the classroom, without the presence of their tea-chers, and the students were continuously assisted by fiveresearchers (two professors and three undergraduate students),toclarify doubts when fillingoutthe question-naires. The study was approved by the Ethics Committee inResearchwithhuman beingsof FaculdadeAsces (CAAE-22210913.8.0000.5203/CEP-ASCES: 072403/2013). Subject participationwasvoluntaryandanonymous,andapassive parentalconsentformwasobtained.
Personal information, as well as socioeconomic and sociodemographic variables, were acquired through the translatedandadaptedversionoftheGlobalSchool-based StudentHealthSurvey(GSHS),proposedbytheWorldHealth Organization(WHO).Attheanthropometricmeasurements, alladolescentsworelightclothingandwerebarefoot.Body mass wasmeasured in an electronic Beurer scale (Beurer GmbH,Ulm,Germany)withamaximumcapacityof150kg andaccuracyof100g.Heightwasmeasuredusingaportable stadiometer(Wiso,SC,Brazil)withanaccuracyof0.5cm. Body mass index (BMI) was calculated by dividing body weightinkilogramsbythesquareofheightinmeters.Waist circumference (WC) wasdetermined asthe minimum cir-cumferencebetweentheiliaccrestandthelastrib,usinga non-extendablemetrictape(Sanny,SP,Brazil)graduatedin millimeters.AfterthecalculationsofBMIandwaist circum-ference,thedatawerecategorizedintoquartilesasusedin apreviousstudywithadolescents.17
Bloodpressurewasmeasuredusinganautomated
oscil-lometricdevice(OmronHEM-742,OmromHealthcare,INC,
IL, USA) was used, which was previously calibrated and
validatedfor adolescents.18 Cuff adjustment followedthe
recommendations of the American Heart Association.19
Three blood pressure measurements were taken, after a
one-minuteintervalbetweenthem,carefullyfollowingthe
protocolsrecommended by the VI Brazilian Guidelines on
Hypertension,20 aswellasin relationtothepositioningof
thearm and body, priorrest, instrument calibration,size
ofthesphygmomanometercuff,numberof measurements
taken,andthechoiceofthevalueusedtodetermine
preva-lence.
RegardingtheBPvalueused,thefirstmeasurementwas
discardedandthemeanofthelasttwomeasurementswas
used,bothforthesystolicanddiastolicpressure.The
crite-riausedtoclassifythesubjectswerethoseestablishedby
theNationalHighBloodPressureEducationProgram21;thus,
for the agegroup 14---17years, HBPwasconsidered when
thesystolicbloodpressure(SBP)ordiastolicbloodpressure
(DBP)wasequaltoorgreaterthanthe95thpercentileofthe
TaskForceReportHighBloodPressureinChildrenand
Ado-lescents,1996referencetablesforageandgender,adjusted
for the height percentile of the assessed adolescent. For
studentsaged18---19,thevaluesusedforyoungadultswere
consideredasparameters.
Thefinal datatabulationwasperformed usingthe
Epi-Data program, version 3.1 (Epidata Association, Odense,
Denmark),apublicdomainsystem,whichwasalsousedto
carryouttheelectronicproceduresfor dataentrycontrol
through the check function (controls). In order todetect
errors, data entry wasrepeated and, usingthe duplicate
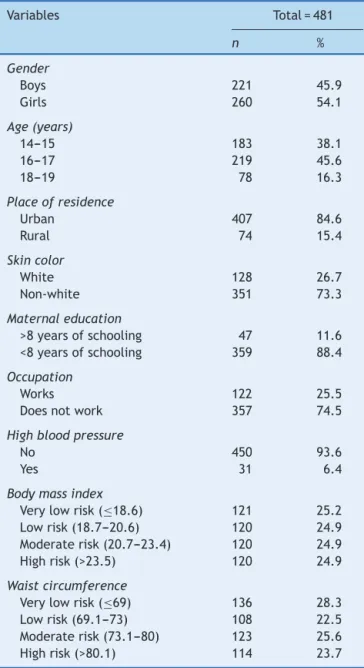
Table 1 Socioeconomic anddemographic characteristics and prevalence of high blood pressure and general and abdominalobesityinhighschoolstudentsfromstatepublic schools,Pernambuco,Brazil,2014.
Variables Total=481
n %
Gender
Boys 221 45.9
Girls 260 54.1
Age(years)
14---15 183 38.1
16---17 219 45.6
18---19 78 16.3
Placeofresidence
Urban 407 84.6
Rural 74 15.4
Skincolor
White 128 26.7
Non-white 351 73.3
Maternaleducation
>8yearsofschooling 47 11.6 <8yearsofschooling 359 88.4
Occupation
Works 122 25.5
Doesnotwork 357 74.5
Highbloodpressure
No 450 93.6
Yes 31 6.4
Bodymassindex
Verylowrisk(≤18.6) 121 25.2
Lowrisk(18.7---20.6) 120 24.9
Moderaterisk(20.7---23.4) 120 24.9
Highrisk(>23.5) 120 24.9
Waistcircumference
Verylowrisk(≤69) 136 28.3
Lowrisk(69.1---73) 108 22.5
Moderaterisk(73.1---80) 123 25.6
24.4 30
25
20
15
10
5
0
25.4 24.0
23.5
9.0
4.7
∗
Boys
Girls
High waist circumference
High blood pressure
Pre
va
lence
, %
High body mass index
Figure1 High riskprevalencerates ofgeneral(BMI>23.5) andabdominal (WC>80.1) obesityand highbloodpressure (per-centile>95th)inhighschoolstudentsofbothgendersfromstatepublicschools,Pernambuco,Brazil,2014.
*p<0.05.
filecomparisonfunction,typing errorsweredetected and corrected.
Data analysis was performed using SPSS (SPSS Inc. StatisticsforWindows,Version10.0,IL,USA).Frequency dis-tributionwasobservedinthedescriptiveanalysis.Pearson’s chi-squaredtestwasusedintheinferentialanalysisto ana-lyzetheisolatedassociationbetweenHBPandgeneraland abdominalobesity,thedifferencebetweentheBP ofboys andgirls,andgeneralandabdominalobesitybetweenboys andgirls,aswellastoanalyzethevariablesinthemodel, explorethepotentialconfounders,andidentifytheneedfor statisticaladjustmentoftheanalyses.
Inthemultivariateanalysis,binarylogisticregressionwas used,byestimatingtheoddsratio(OR)and95%confidence intervalstoexpressthedegreeofassociationbetweenthe independentvariables(generalandabdominalobesity)and thedependentvariable(HBP),usingadjustmentforage,as performed inother studies.22,23 Inadditiontothe
biologi-calplausibility,theagevariableshowed,inrelationtoBP,
a statistical significance level<0.20 (p<0.20), a criterion
usedforentryinthestatistical modelusingthebackward
method.Afterobtainingthepredictivevariablesofthefinal
model,theinteractionoccurrencewastested.The
signifi-cancelevelwassetatp<0.05foralltests.
Skincolor,maternal levelofschooling,occupation,and
placeof residence didnot enterthestatistical model, as
theyhadastatisticalsignificancelevel<0.20inrelationto
BHP: p=0.764, p=0.884, p=0.259,and p=0.526,
respec-tively.
Results
Nineschoolsofthepublicstateeducationalsystemlocated inthe city ofCaruaru wereassessed.Of the569 students whowere in class onthe day of data collection, 31 ado-lescentsrefusedtoparticipateand26werenotallowedto participateinthestudybytheirparentsorguardians, total-ing57refusals.Datawerecollectedfrom512adolescents; however,thefinalsample,correspondingtostudentsaged
between14and19years,comprised481students,ofwhom 54.1%werefemales.Thecharacteristicsoftheadolescents areshowninTable1.
TheprevalenceofHBPwas6.4%,beinghigheramongboys
(9.0% vs. 4.7%, p<0.05). There was no significant
differ-encebetweengeneral(p=0.903)andabdominal(p=0.157)
obesitywhengenderswerecompared,asshowninFig.1.
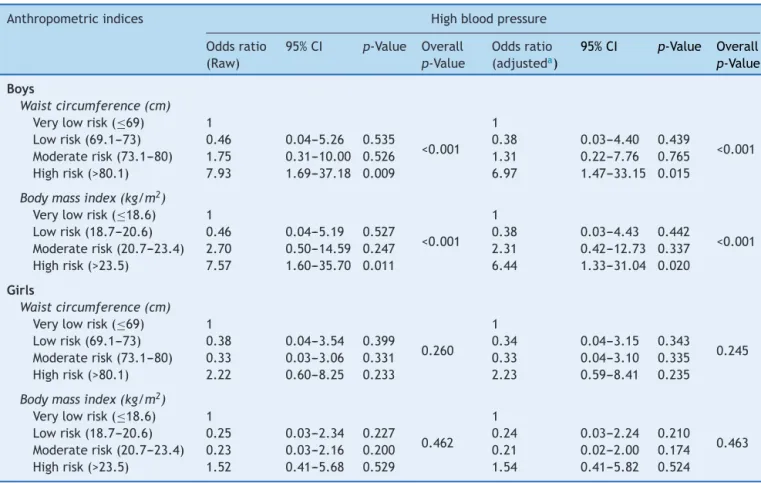
After adjustingfor age, as shown in Table 2, HBP was
associatedwithgeneral(OR=6.44;p=0.001)andabdominal
(OR=6.97; p=0.001) obesity only in boys, when
compar-ing the fourth quartile with the first quartile of the BMI
(≤18.6kg/m2) vs. ≥23.5kg/m2) and waist circumference
(≤69cmvs.≥80.1cm).
Discussion
Thisstudy aimedtoanalyzetheassociationbetween gen-eralandabdominalobesitywithHBPinadolescentsofboth genders.Themainfindingswere:(i)theprevalenceofHBP washigherinboys;(ii)therewasnosignificant difference between general and abdominal obesity when comparing genders; and (iii) HBP was associated with general and abdominalobesityonlyinboys.
TheprevalenceofHBPobservedinthisstudywas6.4%, lower than that found in other studies with adolescents using the HBP>95th percentile as a criterion for HBP diagnosis.14,15,24---26 However, methodological differences,
numberofmeasurements,andthedifferentreference
crite-ria are the main causes of the great variability found in
HBPprevalenceamongtheinvestigations.Inthisstudy,the
authorschosetousegreateraccuracywhendiagnosingHBP,
consideringthata highermethodologicalstringencybased
onthehypertensionguidelinemayresultinalower
preva-lenceofHBP.27
As in other studies,14---16 boys had higherBP than girls.
Inthissense,studiesusingambulatoryBPmonitoring
tech-niquesinchildrenshowedthatwithincreasingage,thereis
anincreaseinbloodpressureinbothboysandgirls;however,
Table2 Rawandadjustedoddsratiobetweenhighbloodpressureandgeneralandabdominalobesity(quartiles)inhighschool studentsofbothgenders,fromstatepublicschools,Pernambuco,Brazil,2014.
Anthropometricindices Highbloodpressure
Oddsratio (Raw)
95%CI p-Value Overall p-Value
Oddsratio (adjusteda)
95%CI p-Value Overall p-Value Boys
Waistcircumference(cm) Verylowrisk(≤69) 1
<0.001 1
<0.001 Lowrisk(69.1---73) 0.46 0.04---5.26 0.535 0.38 0.03---4.40 0.439
Moderaterisk(73.1---80) 1.75 0.31---10.00 0.526 1.31 0.22---7.76 0.765 Highrisk(>80.1) 7.93 1.69---37.18 0.009 6.97 1.47---33.15 0.015
Bodymassindex(kg/m2) Verylowrisk(≤18.6) 1
<0.001 1
<0.001 Lowrisk(18.7---20.6) 0.46 0.04---5.19 0.527 0.38 0.03---4.43 0.442
Moderaterisk(20.7---23.4) 2.70 0.50---14.59 0.247 2.31 0.42---12.73 0.337 Highrisk(>23.5) 7.57 1.60---35.70 0.011 6.44 1.33---31.04 0.020
Girls
Waistcircumference(cm) Verylowrisk(≤69) 1
0.260 1
0.245 Lowrisk(69.1---73) 0.38 0.04---3.54 0.399 0.34 0.04---3.15 0.343
Moderaterisk(73.1---80) 0.33 0.03---3.06 0.331 0.33 0.04---3.10 0.335 Highrisk(>80.1) 2.22 0.60---8.25 0.233 2.23 0.59---8.41 0.235
Bodymassindex(kg/m2) Verylowrisk(≤18.6) 1
0.462 1
0.463 Lowrisk(18.7---20.6) 0.25 0.03---2.34 0.227 0.24 0.03---2.24 0.210
Moderaterisk(20.7---23.4) 0.23 0.03---2.16 0.200 0.21 0.02---2.00 0.174 Highrisk(>23.5) 1.52 0.41---5.68 0.529 1.54 0.41---5.82 0.524
CI,confidenceinterval. aAdjustedforage.
thesameage.28Corroboratingthesefindings,alongitudinal
studyof1267adolescentsfoundthatmaleadolescentswere
morelikelytodevelopHBPintheirlifetime.12
Oneofthemajorriskfactorsforhypertensionisgeneral
obesity.2,16 Asystematicreviewwithmeta-analysisshowed
thatobesechildrenhadbloodpressurelevelsapproximately
40% higher than children with normal weight.2 Regarding
body fat location, an association between general and
abdominal obesity with HBP, through BMI and WC, was
observedinastudywithadolescents;however,sample
strat-ificationbygenderwasnotperformedattheanalysisandthe
interactionbetweenvariableswasnottested.24
Usually,thereisacorrelationbetweenapossibleincrease
in blood pressure in boys and a higher prevalence of fat
accumulationintheabdominalregion,but curiously,even
with no difference between general and abdominal
obe-sitywhencomparinggenders,itwasobservedthattheHBP
wasassociatedwithgeneralandabdominalobesityonlyin
boys.TheseresultsaresimilartothoseobservedbyPayeb
etal.23 Ina study carriedout in Iran with13,486
adoles-cents,thoseauthorsfoundahigherpercentageofobesityin
girls,althoughtheHBPvalueswerehigherinboys.
ApossibleexplanationforthehigherHBPinboysisthat
sex hormones play an important role in BP regulation,29
as increased levels of gonadal hormones may occur
dur-ing childhoodand adolescence and these can modify the
synthesis,release,andbioactivityofthesefactors,
induc-ing vascular relaxation and consequently influencing BP.13
Moreover, Landazuri et al.30 verified that the levels of
angiotensin-convertingenzyme(ACE)wereincreasedinboys
aged11---17years,whiletheyweredecreasedingirlsofthe
same age group. ACE wasthe main enzyme of the
renin-angiotensinsystem,whichinturnplaysanimportantrolein
heartfunctionandBPregulation.Thesignificantreduction
inACEactivityobservedingirls,butnotinboys,indicates
thatestradiolandtestosteronemayhaveadiverseinfluence
onangiotensinconvertingenzyme(ACE)activityinhumans,
particularlyinrelationtoHBP.
Thestudyhasstrengthsandlimitations thatdeserveto
bementioned.The cross-sectionaldesignandthe
correla-tivenatureofthedatapreventusfromestablishingacausal
associationbetweenHBPandobesity.Moreover,the
adoles-cents’ maturationalage,a pointwhich mayberelatedto
hormonalrelease,wasnotassessed.Amongthestrengths,
thisstudyhadarepresentativesample;thesampling
proce-dureswereestablishedtoensurethatthesampleconsisted
of adolescent students that attended schools at different
schoolshifts,andmethodologicalstringencywasemployed
whencollectingBPdata.
According to the data obtained during the study, it
wasobservedthatevenwithnodifferenceinfat
associated with HBP only in boys, regardless of age. The
resultsshowtheneedtostratifythesamplebygenderwhen
theaimisassessingBPinadolescents.Additionally,itwas
observedthatHBPinboysmaynotberelatedtothe
preva-lence of general and abdominalfat accumulation. In this
sense,itisrecommendedtocarryoutstudiesusinga
longi-tudinaldesigntoassesstheinfluenceofsexhormonesonBP
inadolescents.
Funding
TheresearchwasfundedbyFaculdadeASCESScientific Ini-tiationProgram.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.SinghalV,AgalP,KamathN.Theprevalenceofelevatedblood pressureandtheassociationofobesityinasymptomaticfemale adolescentoffsprings ofhypertensive and normotensive par-ents.JClinDiagnRes.2012;6:1158---61.
2.FriedemannC,HeneghanC,MahtaniK,ThompsonM,PereraR, WardAM.Cardiovasculardiseaseriskinhealthychildrenand itsassociation withbodymassindex: systematic reviewand meta-analysis.BMJ.2012;345:e4759.
3.Li S, Chen W, Srinivasan SR, Bond MG, Tang R, Urbina EM, et al.Childhood cardiovascularrisk factors and carotid vas-cularchangesinadulthood:theBogalusaHeartStudy. JAMA. 2003;290:2271---6.
4.deRezendeDF,ScarpelliRA,deSouzaGF,daCostaJO,Scarpelli AM,Scarpelli PA,et al.Prevalence of systemichypertension instudentsaged 7 to14years inthemunicipalityof Barba-cena,intheStateofMinasGerais,in1999.ArqBrasCardiol. 2003;81:381---6.
5.deAraújoTL, deLopes MV,CavalcanteTF, GuedesNG, Mor-eiraRP,ChavesES,etal.Análisedeindicadoresderiscopara hipertensãoarterialemcrianc¸aseadolescentes.RevEscEnferm USP.2008;42:120---6.
6.Brasil,MinistériodaSaúde.Hipertensãoarterialsistêmicapara oSistema Único de Saúde.(Série A. NormaseManuais Téc-nicos).In: Secretariade Atenc¸ão à Saúde Departamentode Atenc¸ão Básica, editor. Brasília: Ministério da Saúde; 2006. pp.7---84.
7.VasquesC, Mota M,Correia T, Lopes V. Prevalence of over-weight/obesityanditsassociationwithsedentarybehaviorin children.RevPortCardiol.2012;31:783---8.
8.WilliamsSM.Weightandheightgrowthrateandthetimingof adiposityrebound.ObesRes.2005;13:1123---30.
9.Hasselmann MH, Faerstein E, Werneck GL, Chor D, Lopes CS.Associac¸ãoentrecircunferênciaabdominalehipertensão arterialem mulheres: EstudoPró-Saúde.Cad SaudePublica. 2008;24:1187---91.
10.JardimPC,Gondim MdoR, MonegoET, MoreiraHG, Vitorino PV,SouzaWK,etal.Hipertensãoarterialealgunsfatoresde risco em uma capital brasileira. Arq Bras Cardiol. 2007;88: 452---7.
11.deMenezesTN,RochaFL,deOliveiraBelémPL,PedrazaDF. Obesidadeabdominal:revisãocríticadastécnicasdeaferic¸ão
edospontosdecortedeindicadoresantropométricosadotados noBrasil.CienSaudeColet.2014;19:1741---54.
12.DasguptaK,O’LoughlinJ,ChenS,KarpI,ParadisG,Tremblay J,et al.Emergenceofsex differencesin prevalenceofhigh systolicbloodpressure.Circulation.2006;114:2663---70. 13.Khalil RA. Sexhormones aspotentialmodulators ofvascular
functioninhypertension.Hypertension.2005;46:249---54. 14.BarrosMV,Ritti-DiasRM,HondaBarrosSS,MotaJ,AndersenLB.
Doesself-reportedphysicalactivityassociatewithhighblood pressureinadolescentswhenadiposityisadjustedfor?JSports Sci.2013;31:387---95.
15.Christofaro DG, Ritti-Dias RM, Chiolero A, Fernandes RA, CasonattoJ,deOliveiraAR.Physicalactivityisinversely asso-ciatedwithhigh bloodpressureindependentlyofoverweight in Brazilian adolescents. Scand J Med Sci Sports. 2013;23: 317---22.
16.Hoffmann M, Pio da Silva AC, Siviero J. Prevalência de hipertensãoarterialsistêmicaeinterrelac¸õescomsobrepeso, obesidade,consumoalimentareatividadefísica,emestudantes deescolasmunicipaisdeCaxiasdoSul.Pediatria(SãoPaulo). 2010;32:163---72.
17.KuschnirMC,Mendonc¸aGA.Riskfactorsassociatedwith arte-rial hypertension in adolescents. JPediatr (Rio J). 2007;83: 335---42.
18.Christofaro DG, Fernandes RA, Gerage AM, Alves MJ, Polito MD,OliveiraAR.Validac¸ãodomonitordemedida depressão arterialOmronHEM742em adolescentes.Arq BrasCardiol. 2009;92:9---14.
19.Pickering TG, Hall JE, Appel LJ, Falkner BE, Graves J, Hill MN, et al. Recommendations for blood pressure mea-surement in humans and experimental animals. Circulation. 2005;111:697---716.
20.Sociedade Brasileira de Cardiologia, Sociedade Brasileira de Hipertensão, Sociedade Brasileira de Nefrologia. VI Dire-trizes Brasileiras de Hipertensão Arterial. Arq Bras Cardiol. 2010;95:1---51.
21.NationalHighBloodPressureEducationProgramWorkinggroup on High Blood Pressure in Children and Adolescents. The FourthReport onthediagnosis,evaluation andtreatmentof high bloodpressure in childrenand adolescents. Pediatrics. 2004;114:555---76.
22.Flechtner-MorsM,NeuhauserH,ReinehrT,RoostH-P,Wiegand S,SiegfriedW,etal.Bloodpressurein57,915pediatricpatients whoareoverweightorobesebasedonfivereferencesystems. AmJCardiol.2015;115:1587---94.
23.Payab M, Kelishadi R, Qorbani M, Motlagh ME, Ranjbar SH, ArdalanG, et al. Associationofjunk foodconsumption with high bloodpressureand obesity inIranian childrenand ado-lescents: the CASPIAN-IV study. J Pediatr (Rio J). 2015;91: 196---205.
24.ChristofaroDG,Ritti-DiasRM,FernandesRA,PolitoMD,Andrade SM,Cardoso JR, et al. Detecc¸ãode hipertensão arterial em adolescentes através de marcadores de adiposidade geral e abdominal.ArqBrasCardiol.2011;96:465---70.
25.GomesJC.Oatualensinodaéticaparaosprofissionaisdesaúde eseusreflexosnocotidianodopovobrasileiro.RevistaBioética. 2009;4:53---64.
26.GrizLH,ViégasM,BarrosM,GrizAL,FreeseE,BandeiraF. Preva-lenceofcentralobesityinalargesampleofadolescentsfrom publicschoolsinRecife,Brazil.ArqBrasEndocrinolMetabol. 2010;54:607---11.
28.JacksonLV,ThalangeNK,ColeTJ.Bloodpressurecentilesfor GreatBritain.ArchDisChild.2007;92:298---303.
29.ReckelhoffJF,FortepianiLA.Novelmechanismsresponsiblefor postmenopausalhypertension.Hypertension.2004;43:918---23.