r e v b r a s o r t o p . 2016;51(4):471–474
SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Case
Report
Transtriquetral
perihamate
fracture-dislocation:
case
report
夽
Frederico
Barra
de
Moraes
∗,
Rodrigo
Cunha
Ferreira,
Stéphanie
Zago
Geraldino,
Renato
Silva
Farias,
Ricardo
Pereira
da
Silva,
Mário
Yoshihide
Kuwae
UniversidadeFederaldeGoiás(UFG),FaculdadedeMedicina,Goiânia,GO,Brazila
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received24October2014
Accepted1December2014
Availableonline4July2016
Keywords:
Carpalbones/injuries
Bonefractures
Dislocations/radiography
Handtrauma/radiography
a
b
s
t
r
a
c
t
Thewristisaregionthatisveryvulnerabletoinjuriesoftheextremities.Amongthese
injuries,fracturesofthepyramidalbone(ortriquetrum)inassociationwithdislocationof
thehamateandcarpalinstabilityareuncommon.Theyaregenerallycorrelatedwith
high-energytraumaandmaybeassociatedwithneurovasculardeficits,muscle-tendondisorders,
skinlesionsorinjuriestoothercarpalbones.Thus,inthisreport,oneoftheserarecases
oftranstriquetralperihamatefracture-dislocationwithcarpalinstabilityispresented,
diag-nosedbymeansofradiographyontherightwristofthepatientwhopresentedpain,edema
andlimitationofflexion-extensionofthecarpusaftertraumatotheregion.Thestagesof
attendingtothecasearedescribed,fromtheinitialconsultationtothesurgicaltreatment
andphysiotherapy,whichculminatedinrestorationofthestrengthandrangeofmotionof
thewrist.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora
Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Fratura-luxac¸ão
transtriquetral
peri-hamato:
relato
de
caso
Palavras-chave:
Ossosdocarpo/lesões
Fraturasósseas
Luxac¸ões/radiografia
Traumatismosdamão/radiografia
r
e
s
u
m
o
Opunhoéumaregiãomuitovulnerávelatraumasdeextremidade.Entretaislesões,as
frat-urasdopiramidal(outriquetrum),associadasàluxac¸ãodohamatoeàinstabilidadecarpal,
sãopoucofrequentes.Geralmenterelacionadasatraumatismosdealtaenergia,podemestar
associadasadéficitneurovascular,miotendíneo,lesõesdepeleouemoutrosossosdocarpo.
Assim,nesterelato,apresenta-seumdessescasosrarosdefratura-luxac¸ãotranstriquetral
peri-hamatocominstabilidadecarpal,diagnosticadasporradiografiasdopunhodireitode
umpacientequeapresentavador,edemaelimitac¸ãodaflexoextensãodocarpoapóstrauma
夽
StudyconductedattheUniversidadeFederaldeGoiás(UFG),FaculdadedeMedicina,HospitaldasClínicas,DepartamentodeOrtopedia
eTraumatologia,Goiânia,GO,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](F.B.Moraes).
http://dx.doi.org/10.1016/j.rboe.2016.06.006
2255-4971/©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Thisisanopenaccessarticle
472
rev bras ortop.2016;51(4):471–474naregião.Asetapasdoatendimentoforamdescritasdesdeaconsultainicialatéo
trata-mentocirúrgicoeafisioterapia,queculminaramcomarestaurac¸ãodaforc¸aedaamplitude
demovimentodopunho.
©2015SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier
EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Fractures of the pyramidal bone(or triquetrum) in
associ-ation withdislocationofthe hamateand carpal instability
areuncommon,usuallyrelatedtohigh-energytrauma,and
may beassociatedwithneurovascular deficit, skinlesions,
myotendinous or even other carpal bones injuries. Early
diagnosis and treatment of these injuries can prevent
complications.1 Indeed, the stability of the bone-ligament
structureofthecarpusisessentialforitsproperfunctioning.2
Thisstudyaimedtoreportararecaseoftranstriquetral
peri-hamatefracture-dislocationanditstreatment.
Case
report
A27year-oldmalemanuallaborer,right-handed,presented
totheemergencyroomwithseverepain(VAS=7)intheright
wrist, edema ++/4+, with limited carpal flexion-extension
withoutskinlesionsorneurovasculardeficit.Hereported
hav-ingsufferedadirecttraumatotherightwristonthesameday,
whichhadbeencrushedbetweentwoironbarsatwork.Pain
wasmoreintenseonpalpationoftheulnarregionofthewrist,
withaslightcrackleandinstability.
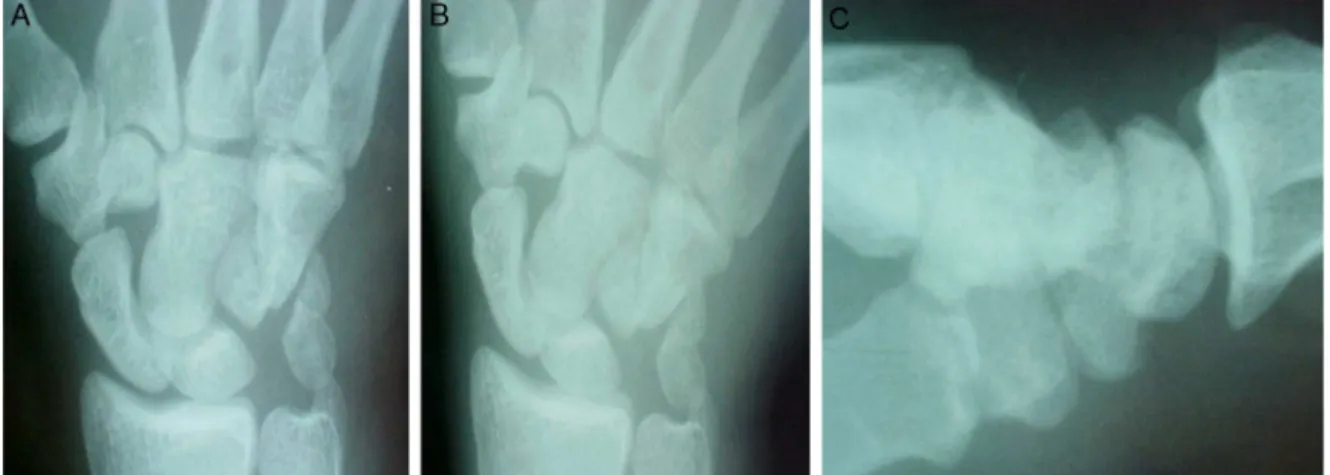
Rightwristradiographsweremadeintrueanteroposterior,
ulnardeviation,andprofileviews,whichindicatedfractureof
thepyramidalandinstabilityofthehamate(Fig.1).
Patientunderwent surgery; a dorsal incision wasmade,
followedbyanopenreductionofthehamate-capitate
insta-bilityandreductionofpyramidalfracture,whichwerefixed
withKirschnerwires.Capsulorrhaphyandrepairof
hamate-capitate and lunotriquetral ligaments were alsoperformed
(Fig.2).Thewristwasimmobilizedinashortarmcastforfour
Fig.1–RightwristX-raysintrueanteroposterior(A),ulnardeviation(B),andprofileincidences(C),showingpyramidal
fractureandinstabilityofthehamate.
weeks,andK-wireswereremovedaftereightweeks.
Physi-caltherapywasinitiatedafterthefourthweek.Eightmonths
aftersurgery,patientwasasymptomatic,withrestoredrange
ofmotionandstrength,comparabletothecontralateralside,
withadecreaseinthelast10◦inextensionandflexiononthe
rightwrist(Fig.3).
Discussion
Thewristhasacomplexanatomy,developedforahighly
spe-cializedfunction,andatthesametimeitisveryexposedto
extremity traumathroughvariousmechanisms. Thecarpal
bones and ligaments promote a multiplanar mobility and
maintainstabilityinthevariousmovementsperformedbythe
wrist,suchasflexion,extension,radialandulnardeviation,
pronosupination,andcircumduction.3,4
Traumamechanismofthisinjurydiffersfromthetheoryby
Mayfieldetal.5,6ofprogressiveperilunateinstabilityingreater
arc injuries, wherethe trauma energypasses through the
carpalbonesandligamentsfromtheradialtotheulnarside
instages,whichwouldbeexplainedinstage3,with
lunotri-quetralligamentrupturewithoutsemilunardislocation.The
injurydescribedinthepresentpatientindicatestheexistence
ofagreater arcinjuryinreverse, from ulnartoradial.The
radialcarpalboneswerespared.7
Moreover,itiscertainthatthepatienthadcarpal
instabil-ity,whichisadisturbanceofthestaticanddynamicbalance
between joints under physiological loads and movements.
This lossofstability, whichis relatedto boneand/or
liga-ment injuries, leads to alterations in the joint anatomical
relationships,affectingthebiomechanicalactivity,aswellas
rev bras ortop.2016;51(4):471–474
473
Fig.2–Radiographsoftherightwristinanteroposteriorincidencewithcastimmobilization(A),transtriquetralperihamate
fracture-dislocationfixedwithK-wires(B),andinprofile(C),showinggoodshaftandsatisfactoryreductionofthelesion.
Fig.3–Imageseightmonthspostoperativelyshowingrestoredrangeofmotionandstrength,butwithadecreaseinthelast
10◦inextensionandflexionoftherightwrist.
Thispattern ofcarpal injury was studied byGarci-Elias
etal.,9whoidentifiedlongitudinalandaxialcarpal
instabil-ities,subdivided intothreegroups: axial-ulnar,axial-radial,
andaxial-radial-ulnar.Thus,thereportedcasewouldbe
clas-sifiedasalongitudinalcarpalinstability,axial-ulnarsubtype,
specificallytranstriquetralperihamate.Itisimportanttonote
thatthecleavagelineinthediastasisbetweenthecapitate
andthehamatemaybesubtleandthediagnosismaybe
over-looked.
Wrist X-rays are usually sufficient for the diagnosis of
theselesions;indoubtfulcases,CTcanbetterassessfracture
lines, and magnetic resonance imaging can identify
liga-mentinjury.8,10 Impairmentofthemediannerveisfrequent
andcantriggercarpaltunnelsyndrome(compressionofthe
median nerve in the carpal tunnel area), characterized by
painwithburning,paresthesia,thenaratrophy,and
limita-tionofactivity.Nervedecompressionisrequired.Althougha
closedreductionandimmobilizationareinitiallypossible,
sur-gicaltreatmentshouldeventuallybeperformedtorestorethe
anatomyandstabilityofthecarpus,aswasdoneinthecase
reported.3–6,10–13
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.NaamNH,SmithDK,GilulaLA.Transtriquetralperihamate ulnaraxialdislocationandpalmarlunatedislocation.JHand SurgAm.1992;17(4):762–6.
2.Ozc¸elikA,GünalI,KöseN,SeberS,Omero ˘gluH.Wrist ligaments:theirsignificanceincarpalinstability.UlusTravma AcilCerrahiDerg.2005;11(2):115–20.
3.TrumbleTE.Principlesofhandsurgeryandtreatment. Philadelphia:Saunders;2000.
4.YeagerBA,DalinkaMK.Radiologyoftraumatothewrist: dislocations,fracturedislocations,andinstabilitypatterns. SkeletRadiol.1985;13(2):120–30.
5.MayfieldJK.Mechanismofcarpalinjuries.ClinOrthopRelat Res.1980;149:45–54.
6.MayfieldJK,JohnsonRP,KilcoyneRK.Carpaldislocations: pathomechanicsandprogressiveperilunarinstability.JHand SurgAm.1980;5(3):226–41.
7.LeungYF,IpSP,WongA,IpWY.Trans-triquetraldorsal perilunatefracturedislocation.JHandSurgEur. 2007;32(6):647–8.
8.SugawaraLM,YanaguizawaM,IkawaMH,TakahashiRD, NatourJ,FernandesARC.Instabilidadedocarpo.RevBras Reumatol.2008;48(1):34–8.
9.Garcia-EliasM,DobynsJH,CooneyWP3rd,LinscheidRL. Traumaticaxialdislocationsofthecarpus.JHandSurgAm. 1989;14(3):446–57.
474
rev bras ortop.2016;51(4):471–474reportswithintroductionofthetranslunatearcconcept.J HandSurgAm.2008;33(10):1770–6.
11.GrahamTJ.Theinferiorarcinjury:anadditiontothefamily ofcomplexcarpalfracture-dislocationpatterns.AmJOrthop (BelleMeadNJ).2003;32Suppl.9:10–9.
12.GreenDP.Carpaldislocationsandinstabilities.In:GreenDP, editor.Operativehandsurgery.3rded.NewYork:Churchill Livingstone;1993.p.917–8.