w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Falls
and
their
association
with
physical
tests,
functional
capacity,
clinical
and
demographic
factors
in
patients
with
rheumatoid
arthritis
Mariana
de
Almeida
Lourenc¸o
a,∗,
Izabela
Roma
b,
Marcos
Renato
de
Assis
baUniversidadeEstadualPaulista(Unesp),SãoPaulo,SP,Brazil
bFaculdadedeMedicinadeMarília(Famema),Marília,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received25August2015 Accepted3August2016 Availableonline24October2016
Keywords:
Rheumatoidarthritis Accidentalfalls Posturalbalance Aptitudetests
a
b
s
t
r
a
c
t
Objective:Toevaluatetheoccurrenceoffallsreportedbyrheumatoidarthritispatientsand itsrelationtodiseaseactivity,functionalcapacityandphysicalfitness.
Materialsandmethods:Across-sectionalstudyconstitutedbyasampleof97rheumatoid arthritispatientsfromthecityofMarília(SP)from2012to2013,wereassessedfordisease activity.InstrumentsvalidatedforBrazilianpopulationinordertoevaluatephysicaland functionalcapacitywereused.Dataanalysiswascarriedoutwithdescriptivestatistics, SpearmancorrelationandChi-squaredtest,consideringp<0.05.
Results:88.7%werefemalesubjectswithameanageof56(±11.7)years.Themedian dura-tionofrheumatoidarthritiswas10years(P25=6andP75=17)andthemeanofdisease activitywas3.6(±1.3), whatwasconsidereda moderateactivity.Inthelast12months 37.1% ofpatientsexperiencedatleastonefall,witha totalof52episodes,andfearof fallingwasreportedby74.2%ofthem,butthiswasnotassociatedtotheoccurrenceof afall(2=1.19,p=0.27).Gender,numberofmedications,age,diseaseactivity,durationof
rheumatoidarthritis,functionalcapacity,andphysicaltestsshowednoassociationswith historyoffallsinthepastyear.
Conclusion: Itwasobservedthattheoccurrenceoffallsandthefearoffallingarequite commoninthispopulation.Theoccurrenceoffallsinthissampleofrheumatoidarthritis patientsbearsnorelationtodiseaseactivity,functionalcapacity,orphysicalfitnesstests.
©2016ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthor.
E-mail:[email protected](M.A.Lourenc¸o).
http://dx.doi.org/10.1016/j.rbre.2016.09.013
Ocorrência
de
quedas
e
sua
associac¸ão
com
testes
físicos,
capacidade
funcional
e
aspectos
clínicos
e
demográficos
em
pacientes
com
artrite
reumatoide
Palavras-chave:
Artritereumatoide Acidentesporquedas Equilíbriopostural Testesdeaptidão
r
e
s
u
m
o
Objetivo: Avaliaraocorrênciadequedasreportadasporpacientescomartritereumatoide (AR)esuaassociac¸ãocomaatividadedadoenc¸a,capacidadefuncionaleaptidãofísica.
Materiale métodos: Estudotransversal comuma amostrade 97 pacientescom ARem Marília(SP),entre2012e2013.Foramusadosinstrumentosvalidadosnapopulac¸ãobrasileira paraavaliarcapacidadefísicaefuncional.Análisedosdadoscomestatísticadescritiva, correlac¸õesdeSpearmanequi-quadrado,consideradop<0,05.
Resultados: Dospacientes,88%erammulheres,médiade56,anos(±11,7),durac¸ãomediana daARde10anos(P25=6eP75=17)emédiadaatividadedadoenc¸a3,6(±1,3).Nosúltimos12 meses,37,1%tiverampelomenosumaqueda(total52episódios),74,2%relatarammedode cair,porémsemassociac¸ãocomaocorrênciadequedas(2=1,19,p=0,27).Sexo,quantidade
demedicamentos,idade,atividadedadoenc¸a,durac¸ãodaAR,capacidadefuncionaletestes físicosnãoestãoassociadoscomhistóriadequedanoúltimoano.
Conclusões: Observou-sequeaocorrênciadequedaseomedodecairéfrequentenessa populac¸ão.AocorrênciadequedasnessaamostradepacientescomARnãoestárelacionada àatividadedadoenc¸a,àcapacidadefuncionaleatestesdeaptidãofísica.
©2016ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Rheumatoidarthritis(RA)isasystemicinflammatory, autoim-mune, chronic, progressive disease of unknown etiology, which can lead to bone destruction and to deformity.1–3
Patients suffering from RA may have muscle weakness, reducedmobility,posturalinstability,proprioceptive,postural balance,andgaitchanges,whichareknownriskfactorsfor falls.4–14
Theoccurrenceoffallshasbeenreported assomething between 14.3%7 and 54%5 in patients with RA. This great
rangecan beexplainedbythelackofcriteria andof stan-dardsinthestudies,inadditiontoafew studiesinvolving fallsandRA.SomestudiesinpatientswithRAhaveshown anassociationoffallswithhigherdisease activity,reduced functional capacity, and with physical fitness and balance tests.4,5,7–9,11,14–17
The impact of the falls reaches physical, psychosocial, economicandfamilyaspects.Thelesionsrangefromsmall abrasions to fractures, particularly in osteoporotic bone (a common comorbidity in patients with RA).5,7,9,11,15–17 By
being a frequent event, the characterization and identifi-cation of patients are fundamental, in order to establish specificprogramsandinterventionsforitspreventioninthis population.
IntheBrazilianpopulation,wefoundonlyonestudyof Mar-quesetal.18onfallsinpatientswithRA,whichshowsthelack
ofnationalstudiesinordertocharacterizethesepatients.In viewofthis,theaimofthisstudywastoevaluatethe occur-renceoffallsinpatientswithRAandtheirrelationshiptoage, diseasedurationandactivity,physicalassessmenttests,and functionalcapacity.
Materials
and
methods
ThestudywasapprovedbytheHumanResearchEthics Com-mittee ofthe Faculdade de Medicina de Marília (FAMEMA) undertheProtocol672/12.Allsubjectsreceivedoraland writ-tenexplanationsandparticipatedinthestudyaftersigning theInformedConsentForm.
A cross-section study was performed, with our con-venience sample comprising 97 patients of both genders diagnosedwithRA,followedinFAMEMARheumatology Out-patient Clinic. To calculate the sample size, the following formula19wasused:
Z12−˛/2P(1−P)
d2 , where
- Z1−˛/2=1.96,for˛=0.05(typeIerror);
- P=the expected proportion of falls in the RA popula-tion,considering35%(anintermediatevaluebetweenthe extremesof15%and55%foundintheliterature);
- d=aprecisionof10%.
The sample size obtainedby this formulawould be 87 patients;weadded10%tocompensateforlossesandrefusals, totaling96patients,buttherewerenorefusalsastothe par-ticipationinthisstudy.
Theinclusioncriteriawere:(a)adiagnosisofRAaccording to the American College of Rheumatology (ACR) classifi-cation criteria of 1987 or to the classification criteria for RA of 2010 from ACR/EULAR (European League Against Rheumatism)1,20,21;(b)ageover18;(c)physicalabilityto
comprehension limiting the interview; (b) severe visual or hearingimpairment.
Patients were evaluated bya rheumatologist (M.R.A.) to confirmthediagnosisofRA,andatthattimemeasurements ofdiseaseactivitywerecarriedout.Patientsunderwentblood samplingperformedbyanurse(I.R.),andthenwerereferred totakemedicalhistoryandaspecificinterviewaboutfalls,as wellastotheapplicationofphysicaltestsbyaphysiotherapist (M.A.L.).
For identification of the falls in the last 12 months, a questionnaire prepared by the researchers was used. The definition adopted for a fall was “an unintentional displacementofthebodytoalevelbelowthestarting posi-tion, with the inability of correction in a timely manner, determined by multifactorial circumstances and affecting stability”.22 The questions concerned the occurrence and
descriptionofthefalls,beingconsideredthelast12months (quantity,location,reason,thetimeofoccurrence,the activ-ity involved, consequences, and the presence of fear of falling).
Toassessdiseaseactivity,theDiseaseActivityScore (DAS-28),whichcountsjointswithpainandswellingin28joints, theoverallself-assessmentofhealthobtainedwiththeuse ofavisualanalogscale(VAS)from0to100,andthe erythro-cytesedimentationrate,giveninmillimetersperhour(mm/h) througha hemosedimentation techniqueperformed atthe BloodCenterofFAMEMA.23–26
The Health Assessment Questionnaire (HAQ),27,28
vali-datedin BrazilbyFerraz et al.,29 was usedtoevaluatethe
functionalcapacityandthefollowingteststomeasure phys-icalcapacity:(a)BergBalanceScale(Berg),proposedbyBerg etal.in1989andvalidated inBrazil byMiyamoto,30 which
evaluatesthebalanceofthepatientin14representative situ-ationsofhis/herdailyroutine;30–32(b)the“TimedUpandGo”
(TUG)test,proposedbyPodsiadloandRichardsonin1991to evaluatebalanceinthesittingposition,thetransferfrom a sittingpositiontoastandingposition,stabilityinambulation, andchangesinthegaitcoursewithouttheuseof compen-satorystrategies;31,33,34(c)6-minWalkTest(6MWT)developed
byBalkein1963andcurrentlyusedtoevaluatethefunctional capacityandexercisetolerance;35–37(d)theGuralnikTest
Bat-teryorShortPhysicalPerformanceBattery(SPPB)developed byJackM.GuralnikandvalidatedinBrazilbyNakano,38used
toevaluatestaticbalance,walkingability,andtheabilityto getupfromachair.39,40
Descriptivestatisticswereperformed,withthe presenta-tionofcentraltendencyanddispersionmeasures,according tothenatureofthedistributionofvariables(mean,median, standarddeviation,andpercentiles)forthecharacteristicsof the sample,description of the falls, and test scorevalues. Tocheckthenormalityofthedata,theKolmogorov–Smirnov testwasapplied.Asthedatawere nonparametric,a corre-lationwith the Spearmantest forthe number offallsand physical,functionalanddiseaseactivitywascarriedout.The followingvalueswereadoptedtointerpretthestrengthof cor-relations:0.0–0.3insignificant;0.3–0.5low;0.5–0.7moderate; 0.7–0.9 high,and 0.9–1.0 veryhigh.41 As tothe association
between groups (fallers and non-fallers) and the variables pharmacologicagents, fear offalling, and gender, the Chi-squared test was used. A significance level ofp<0.05 was
adoptedandall analyseswere performedusingtheSPSSv. 21program.
Results
Ninety-seven patientsparticipatedinthis study;theywere mostly women, married, Caucasian subjectsshowing over-weight, according to body mass index (BMI) (Table 1). All patientsareinuseofatleastonepharmacologicalagentfor RA,and27(27.8%)areusingadisease-modifyingdrug.
Diseasedurationrangedfrom2to40yearswithamedian of10years(P25=6andP75=17),characterizinganestablished diseaseinthesamplestudied.ThemeanforDAS28was3.6 (±1.3),avaluerelatedtoadiseaseinmoderateactivity(>3.2 and≤5.1).26ThemedianofHAQwas0.6(1stand3rdquartiles,
0.1–1.5),whichindicatesamildtomoderatedisability.28
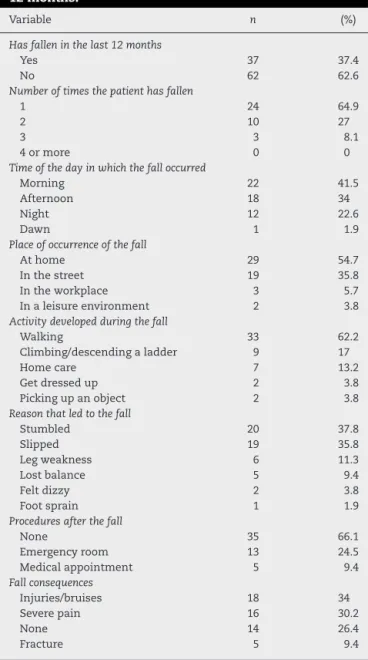
Inthe12monthsprecedingtheinterview,aboutathirdof patientsexperiencedoneormorefalls,totaling52episodes. Nopatienthad4ormorefallsinthepastyear,andthe occur-renceofonlyoneepisodewasthemostfrequentvalueduring thisperiod.Fallsoccurredmorefrequentlyduringtheday,at home,asthesubjectwaswalking,bystumblingorslipping. Inmostepisodes,thepatientdidnotvisitthedoctororthe emergencyroombutsufferedsomekindofinjury/abrasion, orseverepain(Table2).
Fear of falling was reported by 74.2% of patients, both amongthose who sufferedfalling episodesinthe previous
Table1–Samplecharacteristics.
Variable Value
Patients,n 97
Gender,n(%)
Female 86(88.7%)
Male 11(11.3%)
Age(years)
Mean±SD 56.0±11.7
Minimum–maximum 23–88
Weight(kg)
Mean±SD 68.7±15.5
Minimum–maximum 34.3–109.2
Height(m)
Mean±SD 1.57±0.08
Minimum–maximum 1.37–1.78
BMI(kg/m2)
Mean±SD 27.5±5.3
Minimum–maximum 15.3–40.0
Medicines(numberof)
Mean±SD 4.5±1.9
Minimum–maximum 1–10
Maritalstatus,n(%)
Single 17(17.5%)
Married 61(62.9%)
Divorced 10(10.3%)
Widow(er) 9(9.3%)
Race,n(%)
White 60(61.9%)
Brown 25(25.8%)
Black 12(12.3%)
Table2–Characterizationofthereportedfallsinthelast 12months.
Variable n (%)
Hasfalleninthelast12months
Yes 37 37.4
No 62 62.6
Numberoftimesthepatienthasfallen
1 24 64.9
2 10 27
3 3 8.1
4ormore 0 0
Timeofthedayinwhichthefalloccurred
Morning 22 41.5
Afternoon 18 34
Night 12 22.6
Dawn 1 1.9
Placeofoccurrenceofthefall
Athome 29 54.7
Inthestreet 19 35.8
Intheworkplace 3 5.7
Inaleisureenvironment 2 3.8
Activitydevelopedduringthefall
Walking 33 62.2
Climbing/descendingaladder 9 17
Homecare 7 13.2
Getdressedup 2 3.8
Pickingupanobject 2 3.8
Reasonthatledtothefall
Stumbled 20 37.8
Slipped 19 35.8
Legweakness 6 11.3
Lostbalance 5 9.4
Feltdizzy 2 3.8
Footsprain 1 1.9
Proceduresafterthefall
None 35 66.1
Emergencyroom 13 24.5
Medicalappointment 5 9.4
Fallconsequences
Injuries/bruises 18 34
Severepain 16 30.2
None 14 26.4
Fracture 5 9.4
yearandthosewhodidnotsufferanyfall,butwithno sig-nificantassociation(p=0.274)withthe fallsreportedinthe last12months(Table3).Also,therewasnosignificant associa-tionbetweenfearoffallingandage(p=0.289),diseaseduration (p=0.071)anddiseaseactivity(p=0.082).Patientswithafear offallinghadgreaterfunctionalimpairmentmeasuredbythe
Table3–ResultsofphysicaltestsTUG,Berg,6MWTand SPPB.
Results Minimumand maximum
Berg(median,P25–P75) 53(49–56) 15–56 TUG(median,P25–P75) 9.3(7.7–12.2) 5.5–39.4
SPPB(median,P25–P75) 10(8–12) 1–12
6MWT(Mean±SD) 376.7±111.9 120–620
Berg,BergBalanceScale;6MWT,6-minwalktest(inmeters);TUG, TimedUpandGo(inseconds);SPPB,ShortPhysicalPerformance Battery; P25,25thpercentile;P75,75th percentile;SD,standard deviation.
HAQ(p=0.004)andapoorerperformanceon6MWT(p=0.002), TUG(p=0.007)and SPPB(p=0.020)testswhencomparedto thosewhostatedthatwerenotafraidoffalling.
Nosignificantassociationwasfoundbetweenthe
occur-renceoffallsinthelast12monthsandage(=0.070,p=0.498), diseaseactivity(=0.050,p=0629),durationofRA(=−0015, p=0.888)andfunctionalcapacity(=0.167,p=0.102).Also,the amountofdrugstakendailyandpatientgenderhadno asso-ciationwiththepresenceoffallsinthelastyear(Table4).
Theworstperformanceinphysicaltestswasassociated witholderage,longerdiseaseduration,andincreaseddisease activity.Functionalcapacitywasshowntobemoderately asso-ciatedwithperformanceinallphysicaltests,indicatingthat thelimitationoffunctionalactivitiesreflectsapoorer perfor-manceonthesetests.Therewasnoassociationbetweenthe numbersoffallswithanyofthephysicalperformancetests (Table5).
Discussion
Thepercentageofpeoplewhohavesufferedfallsinaperiod of12monthsrangedfrom14.3%7to54%5(18.8%,16 26.9%,17
30.2%,1830.9%,1033%,1135.2%,836.4%,12,1437.1%,4242%,13and
50%9). In this study,about 37% ofthe participants
experi-encedatleastonefallinthelast12months,similartothe 30.2%foundinanotherstudyonaBrazilianpopulation.18This
annualincidenceisconsideredhighwhencomparedtothe estimatedincidenceforeldersover65(28–35%),andover75 (32–42%)years.22
AswasreportedbyStanmoreetal.,12therewasa
predomi-nanceoffallsathome,probablybecausethesesubjectsspend
Table4–Associationsofreportedfallswiththenumberofmedications,thepresenceoffearoffalling,andgender.
Occurrenceoffalls 2 p
No(n) Yes(n)
Medicines Upto3 24 8
3.002 0.083
4ormore 37 28
Fearoffalling Yes 43 29
1.199 0.274
No 18 7
Gender Female 55 31
0.370 0.543
Male 6 5
Table5–Associationsbetweenage,durationofRA, DAS28,HAQandnumberoffallsversus physical
performancetests.
Berg 6MWT TUG SPPB
Age −0.392a −0.315a 0.322a −0.335a
DurationofRA −0.233a −0.261a 0.160 −0.179 DAS28 −0.420a −0.286a 0.329a −0.433a
HAQ −0.575a −0.534a 0.546a −0.687a
Numberoffalls −0.141 −0.051 0.072 −0.139
RA,rheumatoidarthritis;DAS28,DiseaseActivityScore28;HAQ, HealthAssessmentQuestionnaire;Berg,BergBalanceScale;6MWT, 6-minwalktest(inmeters);TUG,TimedUpandGo(inseconds); SPPB,ShortPhysicalPerformanceBattery;Age(inyears);Duration ofRA(inyears).Spearmancorrelation.
a p<0.05.
mostoftheir timeindoors,duetoamorelimitedlifestyle, wherethesetofphysicallimitations,functionaldependence, and fear force the patient to refrain from work activities, leisure,andsocialparticipation.Anotherexplanationistheir greatfamiliaritywith the homeenvironment, wherethose existingextrinsicriskfactorsfortheoccurrenceoffallsare underestimated.
Inthisstudy,aminority(32.7%)soughtsomekindof spe-cialized care after the fall; this finding is similar to that observedinthestudiesbyFesselandNevitt10(31%)and
Stan-more et al.12 (26%). This is perhaps explained by the low
severity ofthese injuries, that indeed were minor lesions, abrasions,andpain,asoccurredinthereviewedstudies.8,10,12
RApatientsareatincreasedriskofosteoporoticfracture, whichresultsfromtheinteractionbetweenanincreasedbone fragility(low bonedensity) and trauma, and the fall is an importantcausativefactorinadultsofallageswithRA.We observedahigherincidence(9.6%)offracturesfromfallsin ourpatients,whencomparedtootherstudiesthatrangefrom 1.1%to5%,aswellasintheelderly,whosefracturesoccurin about5%offalls.9,11,16,22
Thefearoffallingcausespatientstochangetheir behav-ior,includingadecreaseinrecreationalactivities.8,10Thisfear
canleadtoacycleinwhichthepatientphysically commit-tedbyRAgoesontoavoidriskysituationsandbecomesless active,whichworsenshis/herphysicalcapacityandincreases thechancesofafuturefall.Nonationaldatawasfoundto quantifythefearoffallingamongapopulationwithRA; how-ever,weconsiderthepercentagefoundinourstudyasbeing high(74.2%), whencomparedwiththe percentageofother countries(20.6%,446.2%,1750.5%,1059.8%,8and66.7%7).
According to Duyur C¸akat et al.,7 patients with fear of
fallingsufferfromthediseaseforlongerperiodsoftimeand produceworsescoresontheBeckDepressionScale,besidesa poorerphysicalperformance.Itwasfoundthatpatientswith fearoffallingshowedworsephysical/functionalcapacity, per-hapsbecausethesesubjectsdidnotperformthetestsattheir maximumcapacity,whichhamperstosomeextenttheresults ofphysicaltests.
Regardingtheuseofpharmacologicaldrugs,nosignificant differencebetweenthegroupsoffallersandnon-fallerswas found,asinthe studyofSmuldersetal.13 Intheliterature
reviewed,itwasobservedthatagreaterriskoffallingisrelated
tothegreater amountofmedicationthatthe patienttakes (OR=1.4428),and tothe useofantidepressants(OR=2.0928)
andsteroids.14
Asintheliteratureonthissubject,althoughageisamajor riskfactor,beingcommonlyassociatedwiththepresenceof falls,thisfactorisnotassociatedwiththeoccurrenceoffallsin patientswithRA.4,7,9–15,17Apossibleexplanationforthis
find-ingisthatpeoplewithRA(notcontrolled,oralreadywiththeir sequels)haveriskfactorssimilartothephysiological charac-teristicsofaging,thatpredisposethesesubjectstothefalls. Thus,thesepatientsshowaprematureaging,atleastfrom thestandpointoftheirlocomotorsystem.Amongallstudies, onlythatofBugdaycietal.16 foundanassociationbetween
ageandtheoccurrenceoffalls;ontheotherhand,Schober etal.42foundthatolderagewasassociatedwithanincreased
riskoffallsinpatientswithRA,andsomestudiespointtothe needtofurtherinvestigatetherelationshipbetweenageand theoccurrenceoffallsinthispopulation.14,17
Regardingthediseaseduration,themeanoftheexamined studieswas11–17years,5,7–11,13,15,17 andourmedianwas10
years.Noassociationwasfoundbetweendiseasedurationand occurrenceoffallsinthisstudy(=−0015,p=0.888)aswellas inseveralotherstudies.5,9,11,13,17
Themean scoreofdisease activity (assessed by DAS28) foundinourstudy,3.6(±1.3),showsamoderateactivity,but noassociationwiththeoccurrenceoffalls(=0.050,p=0629). AsinStanmoreetal.12,14andinDuyurC¸akatetal.7studies,in
thegroupoffallersthescoreofdiseaseactivityishigher ver-susnon-fallers(3.7and3.5,respectively).Ontheotherhand, Hayashibaraetal.9foundnodifferenceinDAS28between
fall-ersandnon-fallers.
As Böhler et al.17 found, we observed an association
betweendiseaseactivityandperformanceinphysicaltests, indicating that patients with higher disease activity may havemoredifficultyinperformingphysicaltests,thusgetting worseresults.
In its vast majority, the studied sample shows a mild-to-moderate impairment byHAQ, and there isa moderate association between poor functional score and worst per-formance in physical tests; but an association with the occurrenceoffallscouldnotbedemonstrated.Accordingto Marqueset al.,18 functionaldisability,measuredbyHAQ,is
themainriskfactorforfallsinBrazilianpatientswithRA.The literatureshowsthatthosepatientswithhigherHAQscores are atgreater risk of falling, suffered a greater number of fallsinthelastyear,havemorefearoffalling(aswasfound inour sample),andhad apoorer performanceonphysical tests.4,5,7,10,13,14,17
This study has some limitations. Information on the occurrence of falls obtained by self-report tend to be underestimated(recallbias) andmany studiessuggestthat prospectivestudiesarecarriedout,wherethefallsare con-trolledbyacalendaroffallsand/orbyphonecalls,andover alonger period oftime than oneyear, as this periodmay notbesufficient todistinguishbetweenfallersversus non-fallers.9,10,12,13,15–17 Some studies11,12,14 show that samples
fromareference outpatientclinicmay notadequately rep-resentthepopulationwithRAingeneral:itisexpectedthat thesesamplespresentagreaternumberofseverecasesofRA; buteventhe mostseverecasescanbeinagoodcondition, thankstotheiraccesstoagoodtreatment.Thefactthatwe didnotconsiderthelevelofphysicalactivityofourpatients, andthewideagerangeofthesample,arealsolimitationsto thisstudy.
Theoccurrenceoffallsisacomplexmultifactorialevent whose predictioncan bedifficult, evenwiththe combined useofmeasuresofactivityofthedisease,functionality,and physicaltests. Physical tests were not associatedwith the occurrenceofpreviousfalls,andthissuggeststhat prospec-tivestudiesareneededinordertoassesstheabilityofthese andotherinstrumentsaspredictiveoftheoccurrenceoffalls inpeoplewithRA.
Conclusions
Ourresultsconfirmanincreasedprevalenceoffallsinpatients withRA;but withnoassociation withage,gender, disease durationandactivity,functionalcapacity,thenumberofdrugs used, andphysicalfitness tests.Physical testshaveshown anassociationwithage,diseaseduration andactivity,and, especially,functionalcapacity.
Funding
A Master’s degree fellowship from Coordenac¸ão de Aperfeic¸oamentodePessoaldeNívelSuperior(CAPES).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. MotaLMH,CruzBA,BrenolCV,PereiraIA,FronzaLSR,Bertolo MB,etal.ConsensodaSociedadeBrasileiradeReumatologia 2011paraodiagnósticoeavaliac¸ãoinicialdaartrite reumatoide.RevBrasReumatol.2011;51:207–19.
2. MotaLMH,CruzBA,BrenolCV,PereiraIA,Rezende-FronzaLS, BertoloMB,etal.Consenso2012daSociedadeBrasileirade Reumatologiaparaotratamentodaartritereumatoide.Rev BrasReumatol.2012;52:152–74.
3. WassermanAM.Diagnosisandmanagementofrheumatoid arthritis.AmFamPhysician.2011;84:1245–52.
4. FuruyaT,YamagiwaK,IkaiT,InoueE,TaniguchiA, MomoharaS,etal.Associatedfactorsforfallsandfearof
fallinginJapanesepatientswithrheumatoidarthritis.Clin Rheumatol.2009;28:1325–30.
5.KazKazH,JohnsonD,KerryS,ChinappenU,TweedK,PatelS. Fall-relatedriskfactorsandosteoporosisinwomenwith rheumatoidarthritis.Rheumatology(Oxford).
2004;43:1267–71.
6.HäkkinenA,KautiainenH,HannonenP,YlinenJ,MäkinenH, SokkaT.Musclestrength,pain,anddiseaseactivityexplain individualsubdimensionsoftheHealthAssessment Questionnairedisabilityindex,especiallyinwomenwith rheumatoidarthritis.AnnRheumDis.2006;65:30–4.
7.DuyurC¸akatB,NacirB,ErdemHR,KaragozA,Sarac¸ogluM. Fearoffalling,fallrisk,anddisabilityinpatientswith rheumatoidarthritis.TurkJRheumatol.2011;26:217–25.
8.JamisonM,NeubergerGB,MillerPA.Correlatesoffallsand fearoffallingamongadultswithrheumatoidarthritis. ArthritisRheum.2003;49:673–80.
9.HayashibaraM,HaginoH,KatagiriH,OkanoT,OkadaJ, TeshimaR.Incidenceandriskfactorsoffallinginambulatory patientswithrheumatoidarthritis:aprospective1-year study.OsteoporosInt.2010;21:1825–33.
10.FesselKD,NevittMC.Correlatesoffearoffallingandactivity limitationamongpersonswithrheumatoidarthritis.Arthritis CareRes.1997;10:222–8.
11.ArmstrongC,SwarbrickCM,PyeSR,O’NeillTW.Occurrence andriskfactorsforfallsinrheumatoidarthritis.AnnRheum Dis.2005;64:1602–4.
12.StanmoreEK,OldhamJ,SkeltonDA,O’NeillT,PillingM, CampbellAJ,etal.Fallincidenceandoutcomesoffallsina prospectivestudyofadultswithrheumatoidarthritis. ArthritisCareRes.2013;65:737–44.
13.SmuldersE,SchrevenC,WeerdesteynV,VandenHoogenFH, LaanR,VanLankveldW.Fallincidenceandfallriskfactorsin peoplewithrheumatoidarthritis.AnnRheumDis.
2009;68:1795–6.
14.StanmoreEK,OldhamJ,SkeltonDA,O’NeillT,PillingM, CampbellAJ,etal.Riskfactorsforfallsinadultswith rheumatoidarthritis:aprospectivestudy.ArthritisCareRes. 2013;65:1251–8.
15.YamagiwaK,IijimaS,FuruyaT,IkaiT,InoueE,TaniguchiA, etal.IncidenceoffallsandfearoffallinginJapanesepatients withrheumatoidarthritis.ModRheumatol.2011;21:51–6.
16.BugdayciD,PakerN,RezvaniA,KesiktasN,YilmazO,Sahin M,etal.Frequencyandpredictorsforfallsintheambulatory patientswithrheumatoidarthritis:alongitudinalprospective study.RheumatolInt.2013;33:2523–7.
17.BöhlerC,RadnerH,ErnstM,BinderA,StammT,AletahaD, etal.Rheumatoidarthritisandfalls:theinfluenceofdisease activity.Rheumatology(Oxford).2012;51:2051–7.
18.MarquesWV,CruzVA,RegoJ,SilvaNA.Influênciada capacidadefuncionalnoriscodequedasemadultoscom artritereumatoide.RevBrasReumatol.2014;54:404–8.
19.CharanJ,BiswasT.Howtocalculatesamplesizefordifferent studydesignsinmedicalresearch.IndianJPsycholMed. 2013;35:121–6.
20.FullerR.Critériodeclassificac¸ãodaartritereumatoide ACR-Eular2010[Editorial].RevBrasReumatol.2010;50:481–6.
21.AletahaD,NeogiT,SilmanAJ,FunovitsJ,FelsonDT,Bingham CO,etal.2010Rheumatoidarthritisclassificationcriteria:an AmericanCollegeofRheumatology/EuropeanLeagueAgainst Rheumatismcollaborativeinitiative.ArthritisRheum. 2010;62:2569–81.
22.SociedadeBrasileiradeGeriatriaeGerontologia.Quedasem idosos:prevenc¸ão.In:Associac¸ãoMédicaBrasileira,Conselho FederaldeMedicina.ProjetoDiretrizes;2008.p.1–15.
24.MelloFM.Análisedacorrelac¸ãodosescoresdeatividadede doenc¸anaartritereumatóide.[dissertation]Florianópolis,SC: UniversidadeFederaldeSantaCatarina;2008,66pp.
25.PrevooMLL,Van’tHofMA,KuperHH,VanLeeuwenMA,Van dePutteLBA,VanRielPLCM.Modifieddiseaseactivityscores thatincludetwenty-eight-jointcounts.Developmentand validationinaprospectivelongitudinalstudyofpatientswith rheumatoidarthritis.ArthritisRheum.1995;38:44–8.
26.AletahaD,SmolenJ.TheSimplifiedDiseaseActivityIndex (SDAI)andtheClinicalDiseaseActivityIndex(CDAI):areview oftheirusefulnessandvalidityinrheumatoidarthritis.Clin ExpRheumatol.2005;23Suppl.39:S100–8.
27.CorbachoMI,DapuetoJJ.Avaliac¸ãodacapacidadefuncionale daqualidadedevidadepacientescomartritereumatoide. RevBrasReumatol.2010;50:31–43.
28.BruceB,FriesJF.TheHealthAssessmentQuestionnaire (HAQ).ClinExpRheumatol.2005;23Suppl.39:S14–8.
29.FerrazMB,OliveiraLM,AraujoPM,AtraE,TugwellP. Crossculturalreliabilityofthephysicalabilitydimensionof thehealthassessmentquestionnaire.JRheumatol. 1990;17:813–7.
30.MiyamotoST,LombardiJuniorI,BergKO,RamosLR,NatourJ. BrazilianversionoftheBergbalancescale.BrazJMedBiol Res.2004;37:1411–21.
31.FigueiredoKMOB,LimaKC,GuerraRO.Instrumentosde avaliac¸ãodoequilíbriocorporalemidosos.RevBras CineantropomDesempenhoHumano.2007;9:408–13.
32.ResendeS,RassiC,VianaF.Efeitosdahidroterapiana recuperac¸ãodoequilíbrioeprevenc¸ãodequedasemidosas. RevBrasFisioter.2008;12:57–63.
33.Shumway-CookA,BrauerS,WoollacottM.Predictingthe probabilityforfallsincommunity-dwellingolderadultsusing theTimedUp&GoTest.PhysTher.2000;80:896–903.
34.GuimarãesLHCT,GaldinoDCA,MartinsFLM,VitorinoDFM, PereiraKL,CarvalhoEM.Comparac¸ãodapropensãode quedasentreidososquepraticamatividadefísicaeidosos sedentários.Neurociências.2004;12:68–72.
35.AmericanThoracicSociety.ATSstatement:guidelinesforthe six-minutewalktest.AmJRespirCritCareMed.
2002;166:111–7.
36.AmericanCollegeofRheumatology.Sixminutewalktest(6 MWT);2011.Availablein:http://ww2.rheumatology.org/ practice/clinical/clinicianresearchers/outcomes-instrumentation/6MWT.asp[accessed02.05.14]. 37.RondelliRR,OliveiraAN,DalCorsoS,MalagutiC.Uma
atualizac¸ãoepropostadepadronizac¸ãodotestede caminhadadeseisminutos.FisioterMov.2009;22: 249–59.
38.NakanoMM.VersãobrasileiradaShortPhysicalPerformance Battery(SPPB):adaptac¸ãoculturaleestudodaconfiabilidade. [dissertation]Campinas,SP:UniversidadeEstadualde Campinas;2007,163pp.
39.AlfieriFM,RibertoM,GatzLS,RibeiroCPC,BattistellaLR.Uso detestesclínicosparaverificac¸ãodocontroleposturalem idosossaudáveissubmetidosaprogramasdeexercícios físicos.ActaFisiatr.2010;17:153–8.
40.UhlerCR.Análisedocontroleposturaldeidososjovense idososmuitoidososcomhistóriadequedas.[dissertation] SãoPaulo:UniversidadeCidadedeSãoPaulo;2008,86pp.
41.MukakaMM.StatisticsCorner:aguidetoappropriateuseof correlationcoefficientinmedicalresearch.MalawiMedJ. 2012;24:69–71.