Relationship between total and segmental bone mineral
density and diferent domains of physical activity among
children and adolescents: cross-sectional study
Tiego Aparecido Diniz
I, Ricardo Ribeiro Agostinete
II, Paulo Costa Junior
II, Bruna Thamyres Ciccotti Saraiva
III, Diego Kanashiro
Sonvenso
IV, Ismael Forte Freitas Junior
V, Rômulo Araujo Fernandes
V, Diego Giulliano Destro Christofaro
VUniversidade Estadual Paulista Júlio de Mesquita Filho (UNESP), Presidente Prudente (SP), Brazil
ABSTRACT
BACKGROUND: This study aimed to investigate the relationship between total and segmental bone mi-neral density (BDM) and physical activity (PA) in diferent domains (school, leisure and sports) among ado-lescents and children.
DESIGN AND SETTING: Cross-sectional study in the Universidade Estadual Paulista Júlio de Mesquita Filho (UNESP).
METHODS: The study sample consisted of 173 children and adolescents (10.31 ± 1.87 years). The BMDs for the whole body (WB) and the regions of the trunk and legs were measured using dual energy X-ray absorptiometry (DXA). PA was measured using the Baecke questionnaire. A regression model was used to analyze the relationship between all the BMDs and the diferent domains of PA.
RESULTS: 41.5% of the adolescents had high percentages of body fat. Regarding the comparison be-tween physically active and insuiciently active adolescents, there were no statistically signiicant dife-rences in any BMD variables (P > 0.05). The BMD of the legs showed positive relationships with the total PA (β = 0.009; P = 0.013) and sports PA (β = 0.010; P = 0.049) after insertion of the confounders. Similarly, the WB BMD showed the same relationships (total PA: β = 0.005; P = 0.045; and sports PA: β = 0.008; P = 0.049). No relationship was found between leisure and school PA and any of the BMDs (P > 0.05).
CONCLUSION: The results indicated that practice of sport was related to higher BMD values, independent of sex, age and body fatness.
IDoctoral Student, Department of Cell and
Developmental Biology, Institute of Biomedical Sciences, University of São Paulo, São Paulo (SP), Brazil.
IIMaster’s Student, Department of Physiotherapy,
Universidade Estadual Paulista Júlio de Mesquita Filho (UNESP), Presidente Prudente (SP), Brazil.
IIIMaster’s Student, Department of Physical
Exercise, Universidade Estadual Paulista Júlio de Mesquita Filho (UNESP), São Paulo (SP), Brazil.
IVUndergraduate Student, Department of Physical
Exercise, Universidade Estadual Paulista Júlio de Mesquita Filho (UNESP), São Paulo (SP), Brazil.
VAssociate Professor, Department of Physical
Exercise, Department of Physical Education, Universidade Estadual Paulista Júlio de Mesquita Filho (UNESP), Presidente Prudente (SP), Brazil.
KEY WORDS:
Bone density. Leisure activities. Motor activity. Sports.
INTRODUCTION
Development of human tissue, including bone tissue, is determined by biological events during childhood and adolescence.1 Bone mineral density (BMD) represents the amount
of inorganic material (calcium and phosphorus) stored in the bones, which varies over the course of life. It can be measured either for the whole body or in segments.1,2 Low BMD
val-ues are related to development of osteoporosis, mainly in later life, but also in pediatric pop-ulations.2 Bone health in adulthood is determined by bone development over the course of
early life, which can be afected by a large variety of variables, such as genetics, nutrition, hormone action, biological maturation and physical activity (PA).3,4
PA exerts signiicant inluence on BMD accrual during growth,4 which can be categorized
into domains (school, leisure and sports). School PA denotes activities performed during school activities,5,6 while leisure PA denotes activities performed during free time.7-9 Moreover, in young
populations, sport PA can itself be considered to be a PA domain.10-12
PA at vigorous intensity, including mechanical loading on the bones, positively afects bone mass due to:
1. Muscle action, which promotes high load and stress on the bones, thereby afecting and modi-fying bone strength and geometry;
In this way, PA can have a greater inluence on some speciic BMD segments in the body.3,11 he BMD of the legs comprises one
compo-nent of weight-bearing joints and may be indicative of a speciic site where bone-loading occurs and tends to have greater impact. On the other hand, upper limbs are used more speciically in activities such as combat sports11 and gymnastics.14 hus, it appears to be of interest
to investigate the efect of PA on BMD in diferent body segments. Moreover, although BMD and PA have been correlated in stud-ies involving organized physical activity (physical exercise and types of sport),15 there are fewer data on the relationship between bone
health and leisure PA. he absence of data on this issue is more rel-evant among young people, because important confounders (body fat, age and gender) afect growth and it is not clear whether the impact of PA is independent of these confounders.
OBJECTIVE
Thus, the objectives of this study were to compare BDM (both total and segmental), between physically active and insuffi-ciently active adolescents, and to evaluate the relationship between the practice of physical activities in different domains (school, sports and leisure), and whole-body and appendicu-lar BMD.
METHODS
Compliance with ethical standards
his study was approved by the ethics board of Universidade Estadual Paulista Júlio de Mesquita Filho (UNESP), Presidente Prudente campus (procedural number: 26702414.0.0000.5402). All procedures performed in this study were in accordance with the ethical standards of the institutional and/or the national research committee, and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Written consent was obtained from all parents before the adolescents were included in the study.
Study design and subjects
his was a cross-sectional study evaluating the level of physical activity and BDM among adolescents in Presidente Prudente at Universidade Estadual Paulista Júlio de Mesquita Filho (UNESP). he study sample was composed of 173 adolescents, aged between 10-14 years (mean = 11.68 years; standard deviation, SD = 1.44), who formed part of a Brazilian social project with activities at a philanthropic institution in Presidente Prudente, state of São Paulo, Brazil. All the children and adolescents of this social project were invited to participate in the study and those who accepted formed part of the study sample. All participants presented a consent statement signed by a parent or guardian, authorizing them to participate in this study.
Anthropometric measurements and biological maturation
Body mass was obtained using a digital scale accurate to 0.1 kg. Height was measured using a ixed stadiometer accurate to 0.1 cm, with a maximum length of two meters. From these mea-surements, body mass index (BMI) was calculated and the z score was generated. Leg length and seated height were measured using standardized techniques. hese measurements were used to cal-culate the maturity ofset, which denotes the time (years) from/to the age of peak height velocity (APHV), which is an important maturational event.16
Bone mineral density
Dual energy X-ray absorptiometry (DXA) was used to assess BDM. DXA can be used to analyze the whole-body, trunk region and leg BMDs (WB BDM, trunk BMD and leg BDM, respectively) in g/m2, along with the percentage body fat (%BF). he
equip-ment used was the Lunar-DPX-NT model (General Electric, GE). he results were expressed as means, which were calculated using speciic sotware supplied with the equipment.
Body fat levels were classiied high if they were above 25% and above 30% for male and female adolescents respectively, in accor-dance with the cutofs proposed by Williams et al.17
Physical activity
Habitual PA was assessed using the questionnaire developed by Baecke et al.,10 which has been validated for use among
Brazilian adolescents.18 This questionnaire assesses habitual
PA according to three different domains: school, leisure and sports outside school. The school score was assessed from questions relating to the amount of time spent performing the following activities during school time: sitting, standing, walking, lifting heavy loads, fatigue and sweating. The lei-sure PA score specifically asked about time spent on watch-ing television, walkwatch-ing, cyclwatch-ing and active transportation (via walking and/or cycling). Finally, the sport PA score was calculated by asking about which two specific sports the adolescent participated in most frequently, their number of hours per week and months per year of participation and their degree of sweating; and by making comparisons of PA levels with other individuals of the same age. The total score was calculated by adding together the individual scores for school, leisure and sport PA.
Moreover, this questionnaire had previously been validated against the gold standard method (doubly labeled water) for mea-surement of PA.19 Children and adolescents located in the highest
Statistical analysis
he data were subjected to the Kolmogorov-Smirnov test to ver-ify normality. If the distribution was found to be normal, the vari-ables of the sample were characterized in terms of the mean and standard deviation. he Pearson correlation was used to examine the relationship between PA and BMD values among the ado-lescents. Regression models were used to evaluate the relation-ship between BMD and PA (treated in this statistical analysis in the continuous form) either with each PA domain or with the total PA, using independent variables. In the irst multivariate analysis, the variables of sex and age were inserted in order to eliminate possible confounding factors when analyzing the rela-tionships between the diferent PA domains and trunk BMD, leg BMD and WB BMD. In the second multivariate model, %BF assessed by means of DXA and maturation was inserted to ver-ify whether the relationships between the PA domains and trunk BMD, leg BMD and WB BMD remained. Firstly, the relation-ship between the diferent domains of physical activity and bone mineral density was evaluated separately; and secondly, these domains were inserted simultaneously in order to verify whether any of the domains overlapped on the others (e.g. situations in which physical activity in school and sports practice were cor-related with higher bone mineral density of the legs, both when analyzed separately and when inserted simultaneously). he sta-tistical signiicance level adopted was 5%.
RESULTS
he DXA evaluation showed that the percentage of the adoles-cents with high levels of body fat (≥ 25% for boys and ≥ 30% for girls) was 41.5%. Girls had a higher percentage of body fat than boys: 38.0% and 49.5% respectively. Table 1 shows the character-istic information of the sample according to the PA level (physi-cally active, moderately or inactive).
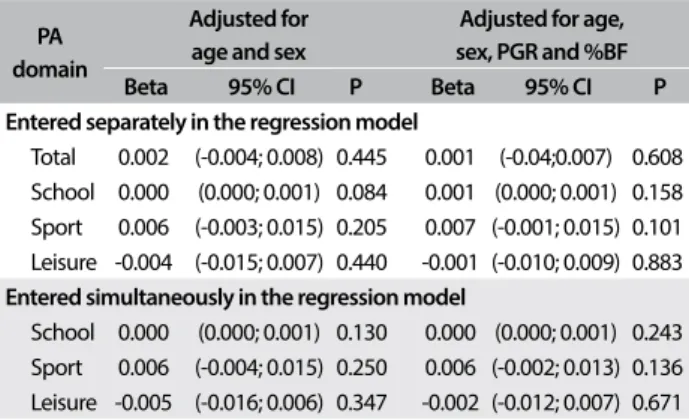
he following PA correlations among the young people were not signiicant: between PA at school and trunk BMD (r = 0.14; P = 0.063); between PA in sports activities outside the school envi-ronment and trunk BMD (r = 0.13; P = 0.077); and between PA during leisure time and trunk BMD (r = 0.06; P = 0.430). Table 2 shows the multivariate analysis information on the relationship between BMD and the diferent physical activity domains. No sig-niicant relationships between the diferent domains of physical activity and trunk BMD were observed.
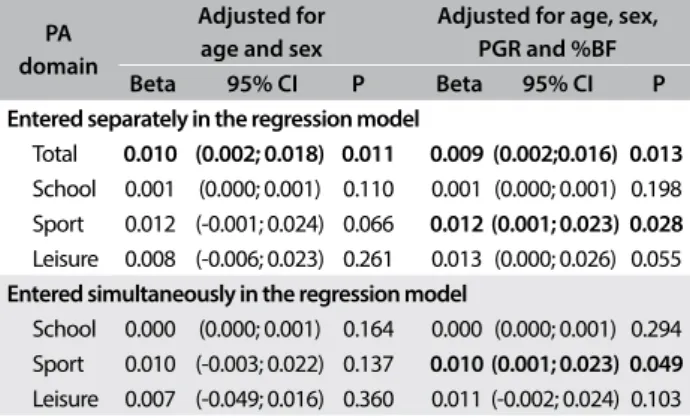
PA performed by the young people at school was not sig-niicantly related to leg BMD (r = 0.13; P = 0.075). However, PA during leisure time showed a signiicant relationship with leg BMD (r = 0.21; P = 0.005) and practicing sports activities outside the school was signiicantly associated with leg BMD (r = 0.20; P = 0.008). In Table 3, in the multivariate analysis, only the sports practice and total PA were related to higher leg BMD.
PA at school was not signiicantly related to WB BMD (r = 0.16; P = 0.111). PA in sports was related to WB BMD (r = 0.18; P = 0.003) and PA during leisure time did not show any signiicant relation-ship with WB BMD (r = -0.13; P = 0.079). Sports practice and total PA were correlated with higher WB BMD in the multivari-ate analysis. his information is shown in Table 4.
he sum of the three PA domains was unrelated to trunk BMD (r = 0.06; P = 0.418), but this sum had statistically signiicant rela-tionships with leg BMD (r = 0.17; P = 0.027) and WB BMD (r = 0.15; P = 0.048).
Ater all adjustments, with the variables entered separately in the multivariate models, it was observed that PA at school and during lei-sure time was not related to the diferent BMDs analyzed (P > 0.05). Sports practice among the adolescents was signiicantly related to higher leg BMD (β = 0.012; 95% conidence interval, CI = 0.001-0.023; P = 0.028) and WB BMD (β = 0.009; 95% CI = 0.001-0.017; P = 0.036) (Tables 2, 3 and 4). Regarding the total PA, which was the sum of the three PA domains, we found positive relationships with leg BMD (β = 0.009; 95% CI = 0.002-0.016; P = 0.013) and WB BMD
Table 1. Characteristics of the subjects according to physical active level
Inactive Mean (SD)
Moderately active Mean (SD)
Suiciently active Mean (SD)
P
Age (years) 10.02 (1.92) 10.45 (1.86) 10.30 (1.94) 0.479 Weight (kg) 42.47 (16.83) 42.50 (13.18) 44.46 (13.39) 0.733 Height (cm) 144.50 (12.41) 146.61 (11.68) 147.32 (13.17) 0.528 BMI (kg/m2) 19.76 (4.98) 19.35 (3.99) 20.23 (4.75) 0.565
Z-score for BMI 0.06 (1.13) -0.06 (0.83) 0.13 (1.06) 0.572 Body fat (%) 25.94 (12.86) 25.08 (11.82) 25.73 (15.80) 0.567 Trunk BMD (g/cm2) 0.76 (0.09) 0.77 (0.08) 0.79 (0.07) 0.231
Leg BMD (g/cm2) 0.95 (0.13) 0.93 (0.12) 1.03 (0.12)a 0.009
WB BMD (g/cm2) 0.93 (0.09) 0.95 (0.07) 0.99 (0.07)a 0.001
SD = standard deviation; BMI = body mass index; BMD = bone mineral density; WB = whole body. astatistically signiicant in relation to the
inactive group.
Table 2. Relationship between trunk bone mineral density and diferent physical activity domains
PA domain
Adjusted for age and sex
Adjusted for age, sex, PGR and %BF Beta 95% CI P Beta 95% CI P Entered separately in the regression model
Total 0.002 (-0.004; 0.008) 0.445 0.001 (-0.04;0.007) 0.608 School 0.000 (0.000; 0.001) 0.084 0.001 (0.000; 0.001) 0.158 Sport 0.006 (-0.003; 0.015) 0.205 0.007 (-0.001; 0.015) 0.101 Leisure -0.004 (-0.015; 0.007) 0.440 -0.001 (-0.010; 0.009) 0.883
Entered simultaneously in the regression model
School 0.000 (0.000; 0.001) 0.130 0.000 (0.000; 0.001) 0.243 Sport 0.006 (-0.004; 0.015) 0.250 0.006 (-0.002; 0.013) 0.136 Leisure -0.005 (-0.016; 0.006) 0.347 -0.002 (-0.012; 0.007) 0.671
(β = 0.005; 95% CI = 0.000-0.011; P = 0.045). When the variables were entered simultaneously in the regression model, only the rela-tionships between the sports domain and leg BMD (β = 0.010; 95% CI = 0.001-0.023; P = 0.049) and WB BMD (β = 0.008; 95% CI = 0.001- 0.015; P = 0.049) remained signiicant.
DISCUSSION
he relationship between PA in diferent domains (school, sports and leisure) and whole-body and segmental BMD measured by means of DXA among children and adolescents was examined. Ater adjusting for confounding variables (age, sex and %BF), the analysis showed that sports practice had a positive relationship with total and segmental BMD, and with total PA analyzed as the sum of the three diferent PA domains.
PA practice appears to be essential for maintaining bone health.20 However, studies have demonstrated that only
physi-cal activities of moderate and vigorous intensity beneit BMD.5,13
In this respect, our study showed that the suiciently active ado-lescents did not show higher total and segmented BMD than that
of the insuiciently active (Table 1). Corroborating our indings, Gracia-Marco et al.21 found that children classiied as physically
active showed no diferences in BMD, compared with sedentary individuals. heir categorization took total PA into account, which may have included sedentary and light activities, which have a less positive relationship regarding addition of BMD.22
he present study demonstrated that total PA (i.e. the sum of school, sports and leisure PA) presented a positive relationship with WB BMD, trunk BMD and leg BMD, even ater all statistical adjustments. Corroborating this, Tobias et al.22 showed that
prac-ticing moderate to vigorous PA had a positive correlation with the BMD of the lower limbs ater adjustments for height, lean body mass and body fat. Neville et al.23 found data similar to ours, i.e. that the
sum of PA, derived from the Baecke questionnaire, was positively associated with increases in lumbar spine and femoral neck BMD. However, the participants in the sample of Neville et al.23 were
15 years or over, while it has been reported that the greatest accrual of bone mass occurs at around 13 and 11 years, respectively, in boys and girls.11 Furthermore, the Baecke questionnaire was used only to
evaluate the total PA, thus missing a lot of information regarding the diferent PA domains (school, sports and leisure).
herefore, we investigated the relationships of all PA domains with total and segmental BMD. It was found that physical activity at school showed no relationship with total or segmental BMD. Agreeing with our results, Heidemann et al.5 found from a
two-year follow-up that increased physical activity at school (e.g. the number of days of physical education) did not give rise to any signiicant increase in BMD. Valdimarsson et al.6 found that girls
who engaged in more than 3 hours of physical education at school per week during a one-year follow-up did not present higher total and leg BMD than those at a traditional school (1 hour of physical education per week). hese indings suggest that physical activity performed only in a school environment is insuicient to generate increases in BMD. Since no details on the type of activities per-formed in these interventions were reported in those studies, we assume that these indings were due to low weight-bearing activi-ties in the interventions.
On the other hand, some studies have demonstrated benei-cial efects on BMD sites from interventions during school time, even ater three years.24 In the study by Meyer et al.,24 the physical
education classes were composed of a multi-component PA inter-vention that included daily physical education with at least 10 min-utes of jumping or strength-training exercises of various intensi-ties. A similar protocol was used by Heidemann et al.,5 comprising
increased numbers of physical education classes, but the results were diferent. In their study, the adolescents who participated in the nine-month intervention program demonstrated increased total BMD. However, comparisons between the results from these studies showed that there were some limitations regarding the type,
Table 3. Relationship between leg bone mineral density and diferent physical activity domains
PA domain
Adjusted for age and sex
Adjusted for age, sex, PGR and %BF Beta 95% CI P Beta 95% CI P Entered separately in the regression model
Total 0.010 (0.002; 0.018) 0.011 0.009 (0.002;0.016) 0.013
School 0.001 (0.000; 0.001) 0.110 0.001 (0.000; 0.001) 0.198 Sport 0.012 (-0.001; 0.024) 0.066 0.012 (0.001; 0.023) 0.028
Leisure 0.008 (-0.006; 0.023) 0.261 0.013 (0.000; 0.026) 0.055
Entered simultaneously in the regression model
School 0.000 (0.000; 0.001) 0.164 0.000 (0.000; 0.001) 0.294 Sport 0.010 (-0.003; 0.022) 0.137 0.010 (0.001; 0.023) 0.049
Leisure 0.007 (-0.049; 0.016) 0.360 0.011 (-0.002; 0.024) 0.103
%BF = body fat: PA = physical activity; PGR = peak growth rate; 95% CI = 95% conidence interval; SD = standard deviation.
Table 4. Relationship between whole body bone mineral density and diferent physical activity domains
PA domain
Adjusted for age and sex
Adjusted for age, sex, PGR and %BF Beta 95% CI P Beta 95% CI P Entered separately in the regression model
Total 0.006 (0.000; 0.012) 0.039 0.005 (0.000; 0.011) 0.045
School 0.001 (0.000; 0.001) 0.179 0.000 (0.000; 0.001) 0.335 Sport 0.008 (-0.001; 0.017) .0074 0.009 (0.001; 0.017) 0.036
Leisure 0.001 (-0.009; 0.012) 0.813 0.004 (-0.005; 0.014) 0.400
Entered simultaneously in the regression model
School 0.000 (0.000; 0.001) 0.273 0.001 (0.000; 0.001) 0.493 Sport 0.007 (-0.002; 0.016) 0.113 0.008 (0.001; 0.015) 0.049
Leisure -0.001 (-0.010; 0.010) 0.995 0.003 (-0.007; 0.012) 0.598
frequency and duration of PA and pubertal maturation, which makes it diicult to establish a pattern in the relationship between school PA and BMD.
In our investigation on the relationship between leisure PA and BMD sites, it was found that school PA was unlikely to be suicient to increase total and segmental BMD. In the Baecke questionnaire, there are two important questions in this section that address how long adolescents spend walking and/or cycling. hus, adolescents who are active with regard to leisure PA must spend more time on these activities. Park et al.9 found that the practice of regular
walk-ing was not positively correlated with total or segmental BMD in adolescents. Corroborating this, in the study by Deere et al.7
ado-lescents who practiced running or high-impact activities presented higher values for hip BMD. In contrast, the practice of jogging showed little beneit at the BMD sites. Another type of leisure PA considered in the questionnaire was cycling. A large number of studies have demonstrated that the practice of cycling is insui-cient to increase total and segmental BMD.8,15 hese results
dem-onstrated that physical activity performed without or with little weight-bearing showed no beneits at the BMD sites.
Moreover, in our study, the practice of sports PA was related to whole-body and leg BMD, even ater introduction of confound-ing variables in the multivariate model. Corroboratconfound-ing this, Nasri et al.11 found that adolescents who practiced combat sports had
higher values for total hip and lumbar spine (L2-L4) BMD, com-pared with sedentary individuals. Silva et al.12 found that
adoles-cents who engaged in practicing sports such as soccer and tennis had greater BMD than the control group. On the other hand, ado-lescents who practiced swimming did not present increased BMD. Furthermore, sports can be categorized as vigorous PA. It is known that vigorous PA promotes gains in BMD.11 In this regard,
Cardadeiro et al.13 found that an additional 10 minutes of vigorous
PA per day suggested a 1-2% increase in BMD in children. hese indings are consistent with the results from a 15-year monitoring epidemiological study.25 Moreover, Heidemann et al.5 found
simi-lar indings in their two-year follow-up. Adolescents who increased their amounts of high-intensity PA had greater gains in BMD than did those with lower levels.
hese positive relationships between PA, especially sports, and total and segmental BMD can be explained by the action of osteocytes, which are embedded within the mineralized bone. In response to mechanical loads or microlesions, these provide signals to osteoclasts, which carry out resorption. Moreover, it is known that in pre-pubertal children, the osteogenic process is more sensitive to the mechanical load in the bone, and this can augment the duration of the peak bone mass.4,16 Taken together,
these data suggest that performing sport during adolescence shows great beneits for bone mass, and thus, may prevent development of early osteoporosis.26
Despite the importance of the results found here, it is impor-tant to mention some limitations. he cross-sectional design does not allow any consideration of the efect of time on these ado-lescents and thus does not allow causal inferences. Some of the results were borderline, meaning that the sample size was prob-ably small. Measuring PA by means of the questionnaire of Baecke et al.10 may involve self-reporting errors, since it depends on the
reviewers’ perception. However, among the questionnaires com-monly used in epidemiological studies, use of the one described by Baecke et al.10 seems to be a good strategy for mitigating the
limitations inherent in questionnaires, since it has a high correla-tion with the gold standard for estimating PA. Furthermore, use of this questionnaire allowed us to analyze the diferent domains of PA, thereby indicating how to increase BMD and where public policy should act to provide the means for practicing PA.
CONCLUSION
In summary, in this sample composed of adolescents, sport prac-tice was correlated with higher BMD values, independent of sex, age and body fatness.
REFERENCES
1. Kim J, Jung M, Hong YP, Park JD, Choi BS. Physical activity in adolescence
has a positive efect on bone mineral density in young men. J Prev
Med Public Health. 2013;46(2):89-95.
2. Campos LMA, Liphaus BL, Silva CAA, Pereira RMR. Osteoporose na
infância e na adolescência [Osteoporosis in childhood and adolescence].
J Pediatr (Rio J). 2003;79(6):481-8.
3. Tenforde AS, Fredericson M. Inluence of sports participation on
bone health in the young athlete: a review of the literature. PM R.
2011;3(9):861-7.
4. Vicente-Rodriguez G. How does exercise afect bone development
during growth? Sports Med. 2006;36(7):561-9.
5. Heidemann M, Jespersen E, Holst R, et al. The impact on children’s bone
health of a school-based physical education program and participation in
leisure time sports: the Childhood Health, Activity and Motor Performance
School (the CHAMPS) study, Denmark. Prev Med. 2013;57(2):87-91.
6. Valdimarsson O, Linden C, Johnell O, Gardsell P, Karlsson MK. Daily
physical education in the school curriculum in prepubertal girls during 1
year is followed by an increase in bone mineral accrual and bone
width--data from the prospective controlled Malmö pediatric osteoporosis
prevention study. Calcif Tissue Int. 2006;78(2):65-71.
7. Deere K, Sayers A, Rittweger J, Tobias JH. Habitual levels of high, but
not moderate or low, impact activity are positively related to hip BMD
and geometry: results from a population-based study of adolescents.
J Bone Miner Res. 2012;27(9):1887-95.
8. Duncan CS, Blimkie CJ, Cowell CT, et al. Bone mineral density in
adolescent female athletes: relationship to exercise type and muscle
9. Park S, Park CY, Ham JO, Lee BK. Familial interactions and physical,
lifestyle, and dietary factors to afect bone mineral density of children
in the KNHANES 2009-2010. J Bone Miner Metab. 2014;32(4):455-67.
10. Baecke JA, Burema J, Frijters JE. A short questionnaire for the
measurement of habitual physical activity in epidemiological studies.
Am J Clin Nutr. 1982;36(5):936-42.
11. Nasri R, Hassen Zrour S, Rebai H, et al. Combat sports practice favors
bone mineral density among adolescent male athletes. J Clin Densitom.
2015;18(1):54-9.
12. Silva CC, Goldberg TB, Teixeira AS, Dalmas JC. The impact of diferent
types of physical activity on total and regional bone mineral density
in young Brazilian athletes. J Sports Sci. 2011;29(3):227-34.
13. Cardadeiro G, Baptista F, Ornelas R, Janz KF, Sardinha LB. Sex speciic
association of physical activity on proximal femur BMD in 9 to 10
year-old children. PloS One. 2012;7(11):e50657.
14. Maïmoun L, Coste O, Mariano-Goulart D, et al. In peripubertal girls,
artistic gymnastics improves areal bone mineral density and femoral
bone geometry without afecting serum OPG/RANKL levels. Osteoporos
Int. 2011;22(12):3055-66.
15. Gómez-Bruton A, González-Agüero A, Olmedillas H, et al. Do calcium
and vitamin D intake inluence the efect of cycling on bone mass
through adolescence? Nutr Hosp. 2013;28(4):1136-9.
16. Mirwald RL, Baxter-Jones AD, Bailey DA, Beunen GP. An assessment of
maturity from anthropometric measurements. Med Sci Sports Exerc.
2002;34(4):689-94.
17. Williams DP, Going SB, Lohman TG, et al. Body fatness and risk for
elevated blood pressure, total cholesterol, and serum lipoprotein ratios
in children and adolescents. Am J Public Health. 1992;82(3):358-63.
18. Guedes DP, Lopes CC, Guedes JERP, Stanganelli LC. Reprodutibilidade
e validade do questionário Baecke para avaliação da atividade
física habitual em adolescentes [Reproducibility and validity of the
Baecke questionnaire for assessing of the habitual physical activity in
adolescentes]. Rev Port Ciên Desp. 2006;6(3):265-74.
19. Philippaerts RM, Westerterp KR, Lefevre J. Doubly labelled water
validation of three physical activity questionnaires. Int J Sports Med.
1999;20(5):284-9.
20. Constantini NW, Dubnov-Raz G, Chodick G, et al. Physical activity and
bone mineral density in adolescents with vitamin D deiciency. Med
Sci Sports Exerc. 2010;42(4):646-50.
21. Gracia-Marco L, Tomas C, Vicente-Rodriguez G, et al. Extra-curricular
participation in sports and socio-demographic factors in Spanish
adolescents: the AVENA study. J Sports Sci. 2010;28(13):1383-9.
22. Tobias JH, Steer CD, Mattocks CG, Riddoch C, Ness AR. Habitual levels
of physical activity inluence bone mass in 11‐year‐old children from
the United Kingdom: indings from a large population‐based cohort.
J Bone Miner Res. 2007;22(1):101-9.
23. Neville CE, Robson PJ, Murray LJ, et al. The efect of nutrient intake
on bone mineral status in young adults: the Northern Ireland young
hearts project. Calcif Tissue Int. 2002;70(2):89-98.
24. Meyer U, Ernst D, Zahner L, et al. 3-Year follow-up results of bone mineral
content and density after a school-based physical activity randomized
intervention trial. Bone. 2013;55(1):16-22.
25. Kemper HC, Twisk JW, van Mechelen W, et al. A ifteen-year longitudinal
study in young adults on the relation of physical activity and itness
with the development of the bone mass: The Amsterdam Growth And
Health Longitudinal Study. Bone. 2000;27(6):847-53.
26. Gass M, Dawson-Hughes B. Preventing osteoporosis-related fractures:
an overview. Am J Med. 2006;119(4 Suppl 1):S3-S11.
Sources of interest: None
Conlicts of interest: None
Date of irst submission: February 8, 2017
Last received: March 30, 2017
Accepted: April 7, 2017
Address for correspondence:
Tiego Aparecido Diniz
Departamento de Biologia Celular e Desenvolvimento, Universidade de
São Paulo (USP), Instituto de Ciências Biomédicas
Av. Professor Lineu Prestes, 1.524
Cidade Universitária (SP) — Brasil
Tel. (+55 11) 3091-0883
CEP 05508-900